
Abstract
Objective
This study aimed to determine the characteristics of vulvo-vaginal infections in 14- to 18-year-old girls in late puberty.
Methods
From July 2016 to June 2019, 487 14- to 18-year-old girls with vulvo-vaginal infection in late puberty in West China Second University Hospital were retrospectively studied. The incidence of bacterial vaginosis (BV), the intermediate type of BV, vulvo-vaginal candidiasis (VVC), Trichomonas vaginalis (TV), and differences among the incidence of these infections for patients with different ages were analyzed.
Results
The incidence of BV, the intermediate type of BV, TV, VVC, and unknown pathogenic vaginitis was 25.67%, 19.30%, 2.46%, 29.37%, and 23.20%, respectively. The incidence of BV and VVC was significantly higher than that of TV. The incidence of BV in the 17-year-old group was significantly higher than that in other age groups. The incidence of VVC and non-albicans Candida infection in the 17- and 18-year-old groups was significantly higher than that in the 14-year-old group.
Conclusion
Girls in late puberty are more susceptible to suffer from BV and VVC than TV infections. Therefore, more attention should be paid to the effects of menstrual hygiene, female estrogen levels, the vaginal internal environment, and hygiene in vulvo-vaginal infection at this stage.
Introduction
Vulvo-vaginal infection is one of the most common gynecological diseases. 1 The physical condition of the female genital tract is important for female growth both physically and psychologically. 2 Puberty is a transitional period from childhood to adulthood, and a key developmental period of the female reproductive system from immaturity to maturity. Significant changes in physical growth, gonadal development, secondary sexual characteristics, and psychological behavior occur during puberty. 3 Puberty is divided into three stages, including early puberty (6–8 years old), rapid puberty (9–13 years old), and late puberty (14–18 years old). 4 Puberty is a sensitive period for female physical and mental development. Studies have shown that, in China, girls in late puberty have deficient knowledge regarding prevention of genital diseases in puberty. 2 For most families, the physical level of neglect of girls in late puberty is significantly higher than that of girls in early and rapid puberty. 5 The health condition of the genital tract directly affects female physical and mental development. 6 For girls in late puberty, reproductive organs gradually develop into maturity. Periodical activity is gradually established by the gonadal axis, and sex hormone levels tend to be stable, reaching adult levels.
Vulvo-vaginal infections of girls in late puberty are mainly caused by poor hygiene, decreased immunity, and deficiency of parents’ care and knowledge of reproductive health.7,8 Therefore, investigation of the conditions and differences of vulvo-vaginal infections is important for the reproductive health of girls in late puberty. Vulvo-vaginal candidiasis is one of the most important vulvo-vaginal infections, which is caused by different types of Candida species (spp.) when immunoactivity is lowered locally in the vagina or systemically in girls in late puberty. This study aimed to determine the characteristics of vulvo-vaginal infections of 14- to 18-year-old girls in late puberty and the differences and incidence of these infections.
Materials and methods
Patients
From July 2016 to June 2019, 14- to 18-year-old female patients in West China Second University Hospital were included in the study and divided into five age groups, including groups of 14, 15, 16, 17, and 18 years old. Inclusion criteria were as follows: 1) informed consent was acquired from patients and their guardians, and patients were in late puberty aged from 14 to 18 years old; 2) patients who had clinical symptoms of vulvar discomfort or vulvar redness and swelling, dysuria, pruritus vulvae, and abnormal vaginal discharge; and 3) female patients with a recent diagnosis in our hospital and who were not previously treated with anti-infective drugs for vaginitis. Exclusion criteria were as follows: 1) patients who were treated with anti-infective agents for vaginitis, or with other cleaning agents or pharmaceuticals that would cause interference for diagnosis; and 2) patients who were reexamined in our hospital for the same condition (to exclude those with recurrent infection).
Methods
The patient was placed in the bladder lithotomy position, and a vaginal speculum, which was cleaned with a small amount of saline, was inserted by a gynecologist to expose the cervix. Vaginal discharge in the lateral wall of the upper one third of the vagina was swabbed with sterile cotton and smeared on a sterile glass slide. Vaginal discharge in the same place was swabbed with sterile dry cotton and placed in a culture tube containing sterile saline solution. A cotton swab moistened with sterile physiological saline was used to collect material when encountering a small amount of vaginal discharge. For patients without a sexual life, samples were taken only by inserting sterile dry cotton into the vagina using the same method mentioned above. 9 According to the National Guide to Clinical Laboratory Procedures (Fourth Edition), 10 the smears were taken, heated, and fixed. Then, Gram staining was performed. Gram-positive rods appear blue-violet under a microscope and Gram-negative rods appear red. Cedar wood oil was added under a 1000× oil immersion microscope to observe morphological indicators, such as leukocytes, epithelial cells, Lactobacillus, Trichomonas vaginalis (TV), Candida spp., Gram-negative cocci, Gardnerella vaginalis and Bacteroides, and Gram-variable Mobiluncus spp. The results of all morphological tests were checked by two experienced personnel. The collected vaginal discharge swabs were sent to a microbiology laboratory simultaneously for fungal culture on Sabouraud-agar medium at 37°C for 24 to 96 hours. VITEK mass spectrometry (BioMerieux Industrial Microbiology, Lyon, France) was used to identify a positive fungal culture.
Written informed consent was obtained from all participants and the privacy rights of participants were also respected. All procedures and protocols were in accordance with the Helsinki Declaration as revised in 2013. The study protocol (Medical Research 2017, No. 25) was approved by the Institutional Review Board of the West China Second University Hospital, Sichuan University on 7 March 2017 before initiation of the study.
Assessment of infection
Bacterial vaginosis and the intermediate type of bacterial vaginosis
Under an oil immersion lens, semi-quantitative assessment of Lactobacillus, G. vaginalis, and Gram-variable Mobiluncus spp. was performed. With regard to the morphology of Lactobacillus, 11 Gram-staining showed a blue-purple color, with variable length, no spores, a slender and curved or sphere-rod or rod shape, a single or double chain, and an unbranched state. The morphology of G. vaginalis 11 ranged from 1.5 to 2.5 ×0.5 µm, with obtuse, round ends, variation in size and shape, and Gram-negative Brevibacterium or Gram-negative Proteus. The morphology of Bacteroides 11 was Gram-negative polymorphic Bacillus. The morphology of Gram-variable Mobiluncus spp. was curved Gram-negative Bacillus, with variation in Gram staining, and curved small Bacillus. The score was calculated according to Nugent Scoring System, 12 with the addition of three bacterial scores as the total score. The intermediate type of bacterial vaginosis (BV) was defined as 4 to 6 points and BV was defined as 7 to 10 points in the Nugent Scoring System (Table 1). 12
Nugent scoring system of Gram staining.

Calculation of scores and distribution was performed by determining the average quantity of each type of bacterium observed in every 10 oil immersion fields. 0: No bacterium was found in an oil immersion field; 1+: <1 bacterium per oil immersion field (average value); 2+: 1 to 4 bacteria per oil immersion field; 3+: 5 to 30 bacteria per oil immersion field; 4+: >30 bacteria per oil immersion field; and -: not present. The total score was calculated by addition of three bacterial scores. Normal: 0 to 3 points; intermediate type of BV: 4 to 6 points; BV: 7 to 10 points.
Vulvo-vaginal candidiasis
After Gram staining, vulvo-vaginal candidiasis (VVC) appeared blue-purple. 13 Yeast without budding, and yeast with budding and/or pseudohyphae were observed under an oil immersion lens. The morphology of Candida yeast appeared as Gram-positive oval cells that were smaller than erythrocytes, with different lengths and a diameter of 2 to 6 µm. Yeast with budding was a purple-black germ tube of the protruding cell wall of Candida yeast forms. Pseudohyphae were extending germ tubes of yeast with budding. 14 VVC infection was diagnosed after the finding of yeast without budding, yeast with budding, and/or pseudohyphae in the smears. Positive vaginal discharge was collected for culture and identification, and VVC infection was divided into Candida albicans infection and non-albicans Candida infection.
TV
The life history of TV has only trophozoites, but no cysts. The living body of TV is colorless and transparent, with refractive properties, changeable posture, and strong mobility. After Gram staining, the volume of trophozoites was larger than that of leukocytes, with a length of 10 to 30 µm and a diameter of 10 to 20 µm, and a wide, pyriform, oval, or irregular shape. 15 There was a bubble nucleus in the front end of the body. On the top edge of the nucleus, there were five matrixes arranged in rings, which produced five flagellums. These included four anterior flagellums with an identical length to the body and one posterior flagellum. The posterior flagellum was long and transparent, and protruded from the rear end by passing through the body. TV infection was diagnosed with Gram staining after detection of TV pathogen. 16
Fungal colonization
Under an oil immersion field lens after Gram staining, Candida yeast forms were found by culture, which indicated fungal colonization. 17
Statistical method
The incidence of vulvo-vaginal infection is shown by percentage. The χ2 test was used to examine the difference in incidence of different age groups and infection types. Data were analyzed using SPSS version 20.0 (IBM Corp., Armonk, NY, USA). Statistical significance was defined as P < 0.05. 18
Results
Types and overall conditions of vulvo-vaginal infections in girls in late puberty
We included 487 14- to 18-year-old female patients in this study. For girls in late puberty, the incidence of BV was 25.67% (125 cases), the intermediate type of BV was 19.30% (94 cases), VVC was 29.37% (143 cases, including 20 cases of mixed infections of BV and VVC), TV was 2.46% (12 cases, including 3 cases of mixed infections of BV and TV), and unknown pathogenic vaginitis was 23.20% (113 cases) (Table 2). The incidence of fungal colonization was 1.44% (7 cases). The mixed infection rate of BV and VVC was 4.11%, and that of BV and TV was 0.62%. All mixed infections were divided into VVC or TV. Therefore, we defined all BV and the intermediate type of BV as single infections. For VVC infection, the positive rates of C. albicans and non-albicans Candida were 57.34% (82 cases) and 42.66% (61 cases), respectively. There was no significant difference between the incidence of BV and the total incidence of VVC. The incidence of BV, VVC, and the intermediate type of BV was significantly higher than that of TV (all P < 0.0001). The incidence of BV and VVC was significantly higher than that of the intermediate type of BV (P = 0.0211 and P < 0.0001, respectively).
Differences in the prevalence of BV, VVC, TV, and the intermediate type of BV in girls in late puberty.

BV, bacterial vaginosis; VVC, vulvo-vaginal candidiasis; TV, Trichomonas vaginalis
The lowercase letters denote comparisons of the prevalence of the various infections.
Differences in the incidence of vulvo-vaginal infections and inflammation in girls of different ages
For girls in late puberty, the incidence of BV and VVC was significantly different among patients with different ages (P = 0.0008 and 0.0003, respectively). However, there was no significant difference in the incidence of TV and the intermediate type of BV among patients with different ages (Table 3). All patients were divided into five age groups, including groups of 14, 15, 16, 17 and 18 years old. In multiple comparisons, the incidence of BV in the 17-year-old group was significantly higher than that in the other age groups (all P < 0.05). The total incidence of VVC in the 17- and 18-year-old groups was significantly higher than that in the 14-year-old group (P < 0.05) (Table 4).
The incidence of vulvo-vaginal infections according to age in girls in late puberty.
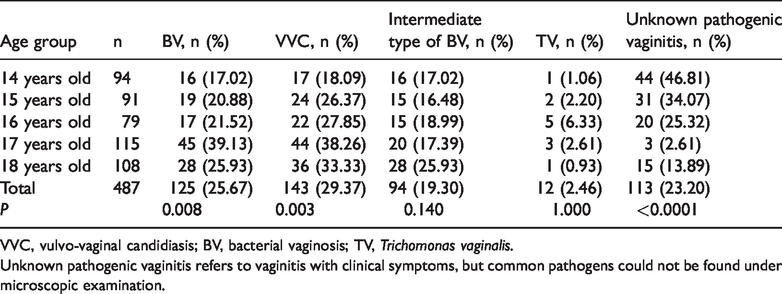
VVC, vulvo-vaginal candidiasis; BV, bacterial vaginosis; TV, Trichomonas vaginalis.
Unknown pathogenic vaginitis refers to vaginitis with clinical symptoms, but common pathogens could not be found under microscopic examination.
Multiple comparisons of the incidence of BV, VVC, TV, and the intermediate type of BV in girls in late puberty by age group.

VVC, vulvo-vaginal candidiasis; BV, bacterial vaginosis; TV, Trichomonas vaginalis; A: 14-year-old group; B: 15-year-old group; C: 16-year-old group; D: 17-year-old group; E: 18-year-old group. Bold indicates significance.
VVC infection in girls in late puberty
With regard to VVC infection in girls in late puberty, there was no significant significance in the total positive rate of C. albicans and non-albicans Candida infections (P = 0.0573). There was no significant difference in the positive rate of C. albicans with age. However, the positive rate of non-albicans Candida was significantly different with age (P = 0.0482) (Table 5). The positive rate of non-albicans Candida in the 17- and 18-year-old groups was significantly higher than that in the 14-year-old group (P = 0.0115 and P = 0.0113, respectively) (Table 6).
Incidence of VVC infections among the different age groups for girls in late puberty.

VVC, vulvo-vaginal candidiasis.
Multiple comparisons of the incidence of Candida albicans and non-albicans Candida in girls in late puberty by age group.

A: 14-year-old group; B: 15-year-old group; C: 16-year-old group; D: 17-year-old group; E: 18-year-old group. Bold indicates significance.
Discussion
Vulvo-vaginal infection is a common gynecological disease, with various infection types and conditions for people in different regions and ages.19,20 In our study, female patients in late puberty were more susceptible to BV and VVC infections than TV infection. The incidence of TV and the intermediate type of BV did not change with age. The incidence of BV in the 17-year-old group was highest in all of the age groups, and older girls (17 and 18 years old) were more susceptible to VVC, especially non-albicans Candida infection.
TV is a vaginitis caused by indirect or direct contact of exogenous TV. 15 TV has high adaptability and vitality to different environments, and it can grow and reproduce under 25°C to 42°C, as well as live for at least 102 hours in 40°C water and for 65 hours in 2°C to 3°C water. In ordinary soapy water, TV is able to live for 45 to 150 minutes, as well as live for 23 hours in damp towels. Even outside of the human body and under semi-dry conditions, TV can live for 14 to 20 hours. 15 Therefore, public areas, such as public baths, toilets, and swimming pools, are the main indirect transmission sites of Trichomonas. 21 In our study, there was no significant difference in the incidence of TV in each age group. This finding indicates that the causes of occurrence of TV in girls at this stage are common and have no obvious relationship with age. Without parents’ care, mature mental development, and full awareness of public hygiene, 22 girls in the late stage of puberty are susceptible to be infected by indirect contact of Trichomonas pathogens in public areas. Additionally, TV infection in some girls in late puberty is caused by direct contact of Trichomonas pathogen via sexual transmission, 23 which has a great effect on female physical and mental growth. This finding can be attributed mainly to female immature development of sexual psychology and low awareness of sexual health. These factors are closely related not only to parents’ improper sex education for their children, but also to a deficiency of sex education to adolescents by institutions. 6 However, studies have shown that TV-susceptible factors may also be related to the vaginal microbial community and immune-mediated factors,24–26 indicating that TV infection is caused by various factors.
BV infection is a mixed infection of G. vaginalis and some anaerobic bacteria, and is caused by poor hygiene or indirect contact. 27 Studies have shown that BV infection is caused by various factors, mainly including microbial diversity of the host vagina, the environment, genetics, and the route of infection.28,29 In our study, the incidence of BV in the 17-year-old group was the highest among the age groups, which may have been due to vaginal microbial diversity of girls at this age. Additionally, 17-year-old girls in China have a stressful life because of preparation for the College Entrance Examination, with tremendous academic pressure and a lack of exercises. This situation may easily cause BV infection by decreased immunity. 30 Furthermore, BV infection is related to contact with unclean water. 31 Female adolescents in late puberty living on campus may have unhealthy public hygiene, increasing the possibility of BV infection via indirect contact. Additionally, 17-year-old female adolescents are in a sensitive period for becoming sexually mature. Without mature mental development, full awareness of sexual health and protection, and their parents’ care, these adolescents are susceptible to having unhealthy and unsafe sexual behavior, 32 leading to BV infection.
VVC infection is a vulvo-vaginitis caused by Candida spp. when the immune response is lowered in the vagina locally or systemically, or when the ability of colonizing Candida to adhere to vaginal epithelial cells is enhanced. 33 Studies have shown that high levels of estrogen and glycogen secretion enhance the reproductive capacity of Candida yeast forms, and growth and reproduction of Candida spp. are enhanced in a warm and humid environment.34,35 In our study, the total incidence of VVC in the 17- and 18-year-old groups was higher than that in the 14-year-old group. This finding may have been due to high estrogen levels and glycogen secretion in the 17- and 18-year-old groups. This could have changed the vaginal internal environment, such as pH values, and enhanced adherence of Candida yeast forms to cause VVC infection. Additionally, the reason for this finding may also have been due to a stressful life in preparing for the College Entrance Examination, which may easily have caused VVC infection by decreased immunity. Furthermore, VVC infection can be due to growth and reproduction of Candida in a warm and humid environment, with improper hygiene, especially for menstrual health. Most 14-year-old girls are in middle school, with less academic pressure, more exercise, and a regular life style, as well as relatively low levels of estrogen and glycogen secretion. With parents’ care, these girls have a better hygiene routine, and therefore, the incidence of Candida spp. is low. For VVC infection in our study, there was no difference in the incidence of C. albicans and non-albicans Candida. This finding is different from that in a previous study, which showed that VVC infection was more easily caused by C. albicans in adult women (>18 years old). 36 However, our finding is consistent with studies in the past decades that reported a progressive shift in the epidemiology of VVC infections from C. albicans toward non-albicans Candida spp.37–39 Therefore, VVC infection varies for different people in different regions and different years. VVC infection may be related to the environment, genetic susceptibility, vaginal fungal colonization, glucocorticoid levels, and immunity.40,41 The increasing incidence of non-albicans Candida in the 17- and 18-year-old groups may be attributed to an increase in estrogen levels as nutrient media in the vagina. Therefore, this allows opportunistic microorganisms that have fewer virulence factors, such as non-albicans Candida, to cause VVC alone or with C. albicans, which has more virulence factors. Additionally, a decrease in immunity in women owing to a stressful life in this period may lead to growth of many different types of Candida.42,43 Fungal colonization was found in 1.44% of 487 girls in late puberty in our study. Fungal colonization may lead to VVC infection.44,45 Consequently, attention should be paid to personal hygiene, enhanced immunity, and a reduction in infection.
There are some limitations in our study. First, morphological observations and retrospective analysis were mainly used in our study, which may have led to some limitations of inclusion and diagnostic criteria, such as the diagnosis of VVC. We will use polymerase chain reaction or molecular biological methods to diagnose various types of vaginitis in future studies. Second, girls in late puberty with elevated white blood cells were initially included in the statistical analysis of vaginitis. However, an increase in white blood cells in vaginal discharge may not be caused by vaginitis, but may be caused by cervicitis or pelvic inflammation. Finally, as a retrospective study, there are some limitations in the inclusion and exclusion criteria of cases in our study. The results and conclusions may have been affected by some unknown factors.
In conclusion, more attention should be paid to the effect of female estrogen levels, the vaginal internal environment, and hygiene on infection. Additionally, there should be focus on a healthy life style, hygiene in public areas (not sharing swimwear, trousers, and bathing equipment, and promoting the use of showers in public toilets and public bathrooms with caution), exercise, enhancing immunity, and strengthening reproduction health education for girls in late puberty. Furthermore, parents’ and institutional awareness towards sex education should be elevated, and various vulvo-vaginal infections should be reduced for physical and mental development of girls in late puberty.
Footnotes
Acknowledgements
We would like to extend our sincere gratitude and thanks to the staff of the Department of Laboratory Medicine, the Outpatient Department of Obstetrics and Gynecology of the West China Second University Hospital, Sichuan University, China, and to investigators of the Key Laboratory of Birth Defects and Related Diseases of Women and Children (Sichuan University), Ministry of Education.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.