
Abstract
Cognitive impairment in focal cerebellar disorders has been widely recognized and is described as cerebellar cognitive affective syndrome (CCAS). However, the relationship between CCAS and crossed cerebello-cerebral diaschisis (CCD) has rarely been discussed. The present report describes the uncommon phenomenon of CCD in two cases with isolated cerebellar infarction, and discuss its contribution to cognitive impairment. Cognitive performance was examined using the CCAS scale and a battery of neuropsychological assessments. Moreover, the relative distribution of cerebral and cerebellar blood flow was measured using three-dimensional arterial spin labeling imaging. Case 1 showed deficits in general cognition and had impaired language, episodic memory, and executive function. Case 2 showed deficits in general cognition at baseline, and cognitive deterioration of visuospatial abilities, language, episodic memory, and executive function was observed at the 3-month follow-up. Both cases met the diagnosis criteria of CCAS. Reduced cerebral blood flow was observed in the cerebral hemisphere contralateral to the cerebellar infarction at baseline in Case 1, and at the 3-month follow-up in Case 2. The present report describes cognitive decline after isolated cerebellar infarction in combination with contralateral cerebral hypoperfusion, as measured using quantitative arterial spin labeling. One possible mechanism involves the functional depression of cerebello-cerebral pathways.
Keywords
Introduction
Beyond the role of the cerebellum in motor control and motor learning, cerebellar contributions to cognition and affect have been firmly established, particularly following the first descriptions of cerebellar cognitive affective syndrome (CCAS) in 1998. 1 Patients with CCAS present with impaired linguistic and executive functions and visuospatial abilities as well as behavioral and psychiatric problems. 1 Bidirectional connections between the cerebellum and cerebrum have been suggested as the anatomic basis of the role of the cerebellum in cognition. 2 The disruption of neural circuits linking the prefrontal, posterior parietal, superior temporal, and limbic cortices to the cerebellum has been proposed as the potential cause of CCAS. 1
Cognitive dysfunction affecting multiple cognitive domains has been observed in patients with isolated cerebellar infarction.1,3 However, these cognitive impairments are usually mild or transient, 3 and may recover over time. 4 It is hypothesized that these cognitive domains are regulated and modulated—rather than generated—by the cerebellum. 5 In addition, the mild or transient cognitive impairments may be associated with the healing effect of neuronal plasticity in intracerebellar and cerebrocerebellar pathways. 4
Crossed cerebello-cerebral diaschisis (CCD) refers to the transient reduction of cerebral activity in areas without structural damage secondary to the primary cerebellar infarction. This has been suggested as a potential cause of cognitive dysfunction in patients with cerebellar lesions. 6 One quantitative single-photon emission computed tomography (SPECT) study reported contralateral hypoperfusion in the left medial frontal lobe secondary to a cerebellar lesion. This occurred in the absence of structural damage in the supratentorial brain regions, thus suggesting a functional impact of the cerebellar lesion on cerebral functioning, leading to frontal-like executive dysfunction, apathy, and disinhibition. 7
The temporal relationship between cognitive dysfunction following isolated cerebellar infarction and the development of CCD remains unclear. Arterial spin labeling (ASL) is a non-invasive magnetic resonance imaging (MRI) technique that measures tissue perfusion using a freely diffusible intrinsic tracer. 8 Recently, three-dimensional ASL was applied to examine the association between cerebral perfusion and cognitive function in patients with vascular cognitive impairment. 9 Here, we report two cases with isolated cerebellar infarction. These patients had no history of neurological or mental illnesses, presence of unconscious state or a critical condition, or presence of severe systemic diseases. Premorbid cognitive impairment was further ruled out using the Information Questionnaire on Cognitive Decline in the Elderly. 10 We applied detailed neuropsychological assessments to evaluate cognitive decline, and used ASL MRI to explore the temporal relationship between cognition and cerebral perfusion changes at baseline and a 3-month follow-up.
Case 1
A right-handed woman in her late 60s complained of intense vertigo and gait unsteadiness. She was a retired worker with a 12-year education, and had a history of diabetes and hypertension. Her vital signs were as follows: arterial blood pressure, 154/93 mmHg; heart rate, 90 beats/minute; and body temperature, 36.1°C. Neurological examination revealed disturbances of balance and motor coordination, ataxia of gait, and dysmetria in her left extremities. She had an International Cooperative Ataxia Rating Scale (ICARS) of 16 11 and a Brunel Balance Assessment (BBA) score of 10. 12 Furthermore, the assessment of fine motor skills using the Finger Tapping Test 13 and Grooved Pegboard Test 14 revealed impaired fine motor skills (Supplementary table 1). No other pathological findings were observed.
Structural MRI on day 10 after disease onset revealed a left cerebellar infarction that was restricted to the territory of the posterior inferior cerebellar artery. The lesion was localized in left lobules VII and VIII. The infarct volume was 62.5 mL (Supplementary figure 1). No supratentorial damage or atrophy was observed (Figure 1). She was given aspirin (100 mg/day) and mannitol (1 g/kg), and her neurological symptoms were greatly ameliorated at discharge. Unfortunately, Case 1 refused a follow-up interview.
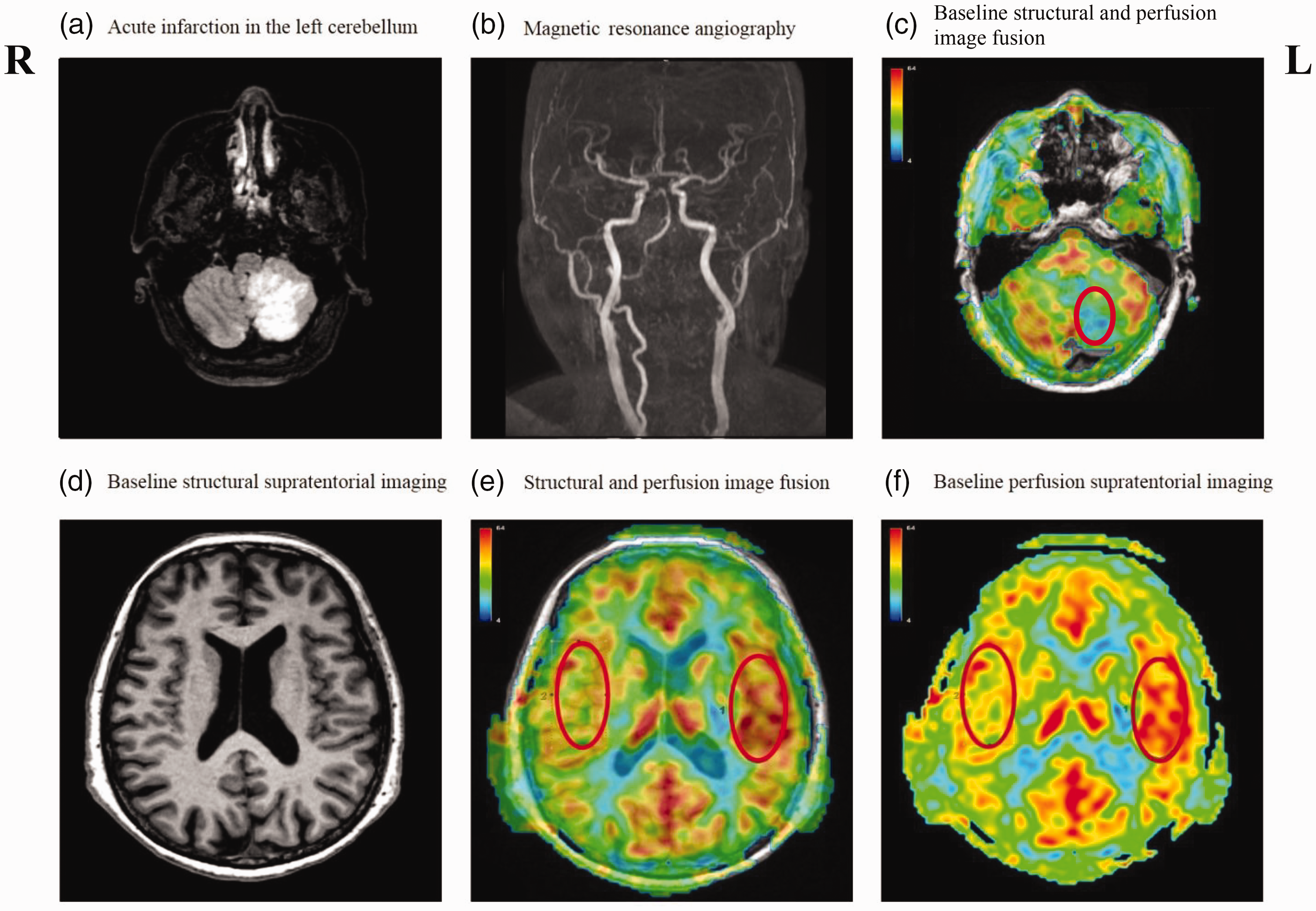
Magnetic resonance images of Case 1 on day 10 after disease onset. Fluid-attenuated inversion recovery (FLAIR) images showed (a) isolated acute cerebellar infarction caused by (b) left vertebral artery occlusion. (b, d) No supratentorial damage or atrophy or internal carotid artery stenosis was observed. (c, f) Arterial spin labeling (ASL) images showed decreased cerebral blood flow (CBF) in the lesions and the contralateral cerebral hemisphere. (c) Average CBF was 21.7 mL per 100 g/minute in the infarction regions (red circle). (e) ASL image superimposed onto a T1-weighted image and (f) CBF was 43.9 mL per 100 g/minute in the region of interest, defined as the most affected contralateral cerebral region, compared with 53.5 mL per 100 g/minute in the mirrored ipsilateral hemisphere. Scale bar shows CBF in mL per 100 g/minute. R, right; L, left.
Neuropsychological evaluation was performed on day 7 after disease onset. Addenbrooke’s Cognitive Examination III (ACE-III) and the CCAS scale (CCAS-s) were administered to evaluate general cognitive function and cerebellar cognition.15,16 In addition, a battery of neuropsychological assessments was applied to further examine cognitive functioning in attention and processing speed, working memory, visuospatial abilities, language, episodic memory, and executive function. Raw scores were converted into z-scores to enable comparisons across measures (Supplementary table 2). The patient scored 82/100 on ACE-III, meeting the diagnostic criteria for cognitive impairment in the Chinese population. 17 She scored 94/120 in the CCAS-s and failed in one item, thus meeting a diagnosis of possible CCAS. In addition, she performed markedly worse than controls on attention (z-score = −1.29) and had impaired language (z-score =−0.81) and episodic memory (z-score =−0.75) (Table 1).
Z-transformed neuropsychological scores in Cases 1 and 2.

ACE-III, Addenbrooke’s Cognitive Examination-III; CCAS-s, cerebellar cognitive affective syndrome scale.
Brain perfusion imaging was acquired using a three-dimensional pseudo-continuous ASL sequence on a 3T MRI scanner (SIGNA Premier; GE HealthCare, Chicago, IL, USA). Hypoperfusion was observed in the infarct regions as well as the contralateral temporal and frontal lobes (Figure 1). The average cerebral blood flow (CBF) of the infarction regions was 21.7 mL per 100 g/minute. The average CBF in the region of interest, placed in the most affected contralateral cerebral region, was 43.9 mL per 100 g/minute; it was 53.5 mL per 100 g/minute in the mirrored ipsilateral hemisphere. In addition, to overcome the potential deviations in CBF quantification, the asymmetry index (AI) was calculated as 17.9% using the following formula: AICBF = (IpsilateralCBF − ContralateralCBF) ∕ IpsilateralCBF. 18
Case 2
A right-handed woman in her late 40s complained of dizziness and memory loss. She had a 9-year education, and had a history of diabetes, hypertension, and hyperlipemia. Her vital signs were as follows: arterial blood pressure, 133/78 mmHg; heart rate, 76 beats/minute; and body temperature, 36.4°C. Neurological examination revealed no abnormalities. She had an ICARS score of 0 and a BBA score of 12, with no balance or motor coordination problems; however, her fine motor control was impaired at baseline and had partially improved at follow-up (Supplementary table 1). Structural MRI on day 15 after disease onset revealed an isolated cerebellar infarction localized in left lobules VII and VIII. The infarct volume was 17.2 mL (Supplementary figure 2). Structural MRI on day 90 after onset showed that the lesion had not expanded. No supratentorial damage or atrophy was observed at either baseline or follow-up (Figure 2). The patient was given aspirin (100 mg/day) and clopidogrel (75 mg/day) and was discharged on day 16 after onset with no neurological symptoms.
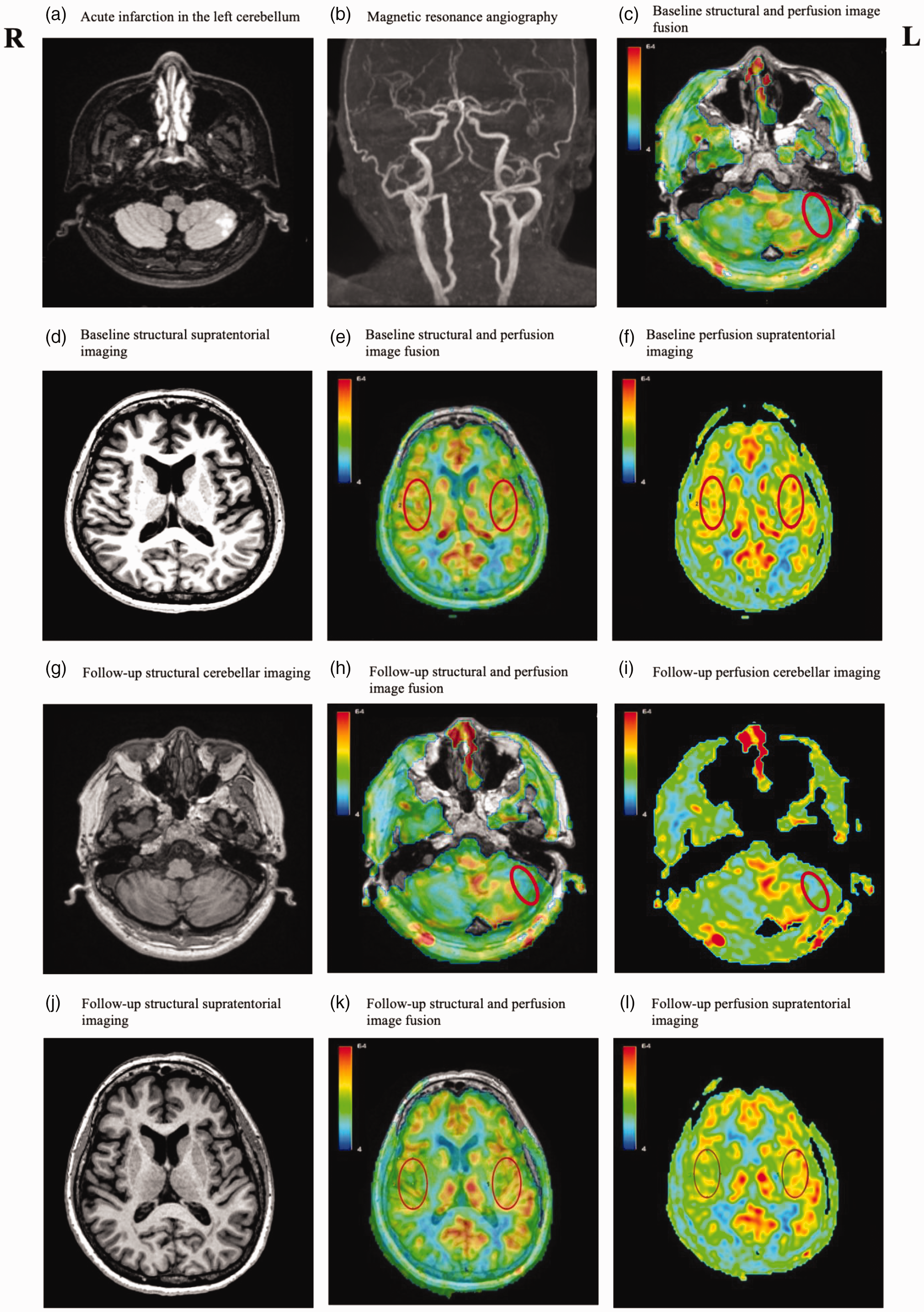
Magnetic resonance images of Case 2 on days 15 and 90 after disease onset. Fluid-attenuated inversion recovery (FLAIR) images showed (a) acute infarction in the left cerebellum, which may be caused by (b) occlusion of the left posterior inferior cerebellar artery. (d, j) No supratentorial damage or atrophy or Continued.internal carotid artery stenosis was observed at baseline or follow-up. (c) At baseline, average cerebral blood flow (CBF) was 20.2 mL per 100 g/minute in the core infarction regions (red circle), identified with spin-labeling (ASL) images. (e, f) At baseline, average CBF was 41.1 mL per 100 g/minute in the ipsilateral supratentorial regions and 41.2 mL per 100 g/minute in the contralateral supratentorial regions. (g) At the 3-month follow-up, a T1-weighted image showed left cerebellar infarct; (h, i) average CBF in the infarction regions was 19.4 mL per 100 g/minute and (k, l) average CBF was 42.0 mL per 100 g/minute in the ipsilateral supratentorial regions and 36.0 mL per 100 g/minute in the contralateral supratentorial regions, which decreased 12.6% from the baseline. (c, e, h, k) ASL images superimposed onto T1-weighted images. Scale bar shows CBF in mL per 100 g/minute. R, right; L, left.
Cognitive assessments were performed on days 14 and 90 after onset. The patient scored 86/100 on the ACE-III at baseline and 84/100 at the follow-up. She had a CCAS-s score of 94/120 and failed in one item at baseline, meeting the diagnosis of possible CCAS.15,16 Her CCAS-s score had decreased to 84/120 and she failed in three items at the follow-up, thus meeting the diagnosis of definite CCAS. Cognitive deterioration of visuospatial abilities (z-score = −3.2), language (z-score = −1.33), episodic memory (z-score = −2.44), and executive function (z-score = −0.46) was observed at the 3-month follow-up (Supplementary table 2 and Table 1).
The average CBF of the infarction regions was 20.2 mL per 100 g/minute at baseline and 19.4 mL per 100 g/minute at the 3-month follow-up (Figure 2). ASL MRI did not reveal any cortical perfusion abnormalities at baseline. Evident hypoperfusion in the contralateral frontal lobe was noted at the 3-month follow-up (Figure 2) with an average CBF of 36.0 mL per 100 g/minute, which was decreased by 12.6% from the baseline (41.2 mL per 100 g/minute). By contrast, the average CBF in the ipsilateral frontal lobe was 41.1 mL per 100 g/minute at baseline and 42.0 mL per 100 g/minute at the follow-up. The AI was 0.0% at baseline and increased to 14.3% at follow-up.
All treatments were administered after acquiring written consent from the patients, and the two patients’ details are de-identified. The reporting of this study conforms to CARE guidelines (for CAse REports). 19 Prior to participating, all individuals provided written informed consent for the publication of this report, which also obtained approval from the ethics committee of Beijing Tiantan Hospital (approval number KY-2021-033-02).
Discussion
The present report identifies the profiles of cognitive changes in patients with isolated cerebellar infarction and discusses their temporal relationships to CCD. Two patients with cerebellar infarction presented deficits in attention, visuospatial abilities, language, episodic memory, and executive function. Reduced contralateral CBF was observed in both patients and was related to their cognitive decline over time. These results suggest that CCD is a potential cause of cognitive dysfunction following isolated cerebellar damage.
In the present report, we revealed cognitive dysfunction in two patients with isolated cerebellar infarction. However, these patients showed milder cognitive deficits than those in a previous study. 20 One possible explanation for this discrepancy is that our report only included patients with cerebellar infarction, whereas the previous study also included patients with cerebellar hemorrhage, which is usually accompanied by cerebral edema and may lead to severe cognitive deficits. In keeping with prior voxel–lesion symptom-mapping studies in patients with cerebellar ischemic infarction,21–23 cognitive changes were associated with lesions in lobules VII and VIII in the present study. By contrast, lesions in lobules III to VI have been associated with motor symptoms.21–23 The distinctive topographic distribution of cerebral and cerebellar cortical areas thus aligns with specialized anatomical and functional connectivity within the cerebrocerebellar circuit. 24 This dichotomy, characterized by anterior-sensorimotor/posterior-cognitive divisions in the cerebellum, is likely a consequence of functional connections between the posterior cerebellum and the frontal and/or temporal lobes. 25 Consistent with previous studies, reduced blood flow was also identified in the frontal and temporal regions in our two patients, and was associated with the occurrence of cognitive dysfunction, suggesting that functional disconnection may be a potential mechanism of CCAS.
A temporal association between cognitive deficits and CCD was observed in our two cases. CCD was detected in both cases; Case 1 exhibited cognitive dysfunction concurrently with CCD, and Case 2 had cognitive decline alongside cerebral hypoperfusion at the 3-month follow-up. CCD can occur in patients with focal cerebellar lesions characterized by decreased cerebral perfusion and metabolism contralateral to primary cerebellar lesions. 26 By contrast, Wallerian degeneration is characterized by structural changes (i.e., atrophy) that spread over the cerebello-cerebral tracts distant from primary cerebellar lesions. Wallerian degeneration is associated with CCD and has been proposed as a potential mechanism for cognitive dysfunction in stroke. 27 CCD can manifest within hours or even minutes following a stroke,28,29 whereas Wallerian degeneration typically occurs 7 to 21 days post-lesion. 30 The baseline cognitive dysfunction in Case 1 may thus be attributed to immediate neuronal deactivation without structural changes in the contralateral cerebral regions, whereas the cognitive decline observed in Case 2 at the 3-month follow-up may be a result of CCD stemming from Wallerian degeneration. Future multimodal neuroimaging studies will be crucial to further elucidate the causes of both early- and late-onset CCD, as well as their associations with Wallerian degeneration. This research is pivotal for advancing our understanding of cognitive dysfunction following cerebellar stroke.
CCD following an isolated cerebellar infarction has not yet been well elucidated. Case 2 showed cognitive deficits at both baseline and the 3-month follow-up, whereas CCD was only found at the follow-up. These findings suggest that CCD may be a possible cause of cognitive dysfunction following cerebellar infarction. However, the lesion size of the isolated cerebellar infarction and the disease duration should be also considered when interpreting these findings. 31 We observed CCD at baseline in Case 1, with a lesion size of 62.5 mL; by contrast, we observed CCD at follow-up in Case 2, with a lesion size of 17.2 mL. Future longitudinal cohort studies and neuroimaging analyses that take both lesion size and disease duration into account are therefore warranted. These studies will help to clarify the prevalence of CCD, how CCD contributes to cognitive changes, and the relationship between the magnitude of ASL anomalies and the severity of cognitive dysfunction in cases of isolated cerebellar infarction.
To the best of our knowledge, the present report details the first use of non-invasive ASL to explore the relationship between cognitive decline and cerebral perfusion in isolated cerebellar infarction. To date, most cases of CCD have been reported using SPECT or positron emission tomography data.7,25,32 However, ASL is more sensitive than SPECT for assessing cerebral perfusion in patients with CCD. 33 Future longitudinal studies using ASL are therefore warranted to understand the temporal progression of CCD and its associations with cognitive decline in isolated cerebellar infarction.
In summary, this report described cognitive dysfunction in patients with isolated cerebellar infarction, and identified the temporal relationship between cognitive dysfunction and the rare phenomenon of CCD for the first time. Our findings indicate that prolonged contralateral cerebral hypoperfusion in isolated cerebellar infarction might be explained—at least in part—by the interruption of cortico-ponto-cerebellar pathways. Nonetheless, more research is needed to understand the implications of CCD on cognitive changes in isolated cerebellar infarction, how CCD progresses over time, and the pathophysiological role of CCD in CCAS.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241235848 - Supplemental material for Reduced cerebral blood flow and cognitive dysfunction following isolated cerebellar infarction: two case reports
Supplemental material, sj-pdf-1-imr-10.1177_03000605241235848 for Reduced cerebral blood flow and cognitive dysfunction following isolated cerebellar infarction: two case reports by Qi Liu, Yingkui Zhang, Chang Liu, Yu Chen and Yumei Zhang in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605241235848 - Supplemental material for Reduced cerebral blood flow and cognitive dysfunction following isolated cerebellar infarction: two case reports
Supplemental material, sj-pdf-2-imr-10.1177_03000605241235848 for Reduced cerebral blood flow and cognitive dysfunction following isolated cerebellar infarction: two case reports by Qi Liu, Yingkui Zhang, Chang Liu, Yu Chen and Yumei Zhang in Journal of International Medical Research
Footnotes
Acknowledgements
The authors are grateful to the patients and their families for their continued support of our research.
Author contributions
Y.C. had access to all study data and was responsible for ensuring the data’s integrity and the accuracy of the analysis. Q.L. and Y.C. developed the study concept, conducted the statistical analysis, and drafted the paper. Q.L., C.L., and Y.C. contributed to data collection. Yi.Z. and Yu.Z. contributed to the study concept. Q.L. and Y.C. revised the manuscript for important intellectual content. All authors approved the submitted version.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was supported by a National Natural Science Foundation of China Youth Program (82001124), an early career research fellowship funded by Beijing Tiantan Hospital, Capital Medical University (2020MP06), a National Natural Science Foundation of general project (82372555, 81972144), and the State Fund from China Scholarship Council (202308110231).
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.