
Abstract
Objectives
To investigate the effects of sevoflurane and propofol anesthesia on inflammatory or anti-inflammatory responses in patients undergoing laparoscopic cholecystectomy (LC).
Methods
Patients undergoing LC (n = 23) were divided into sevoflurane (S) (n = 11) and propofol (P) (n = 12) anesthesia groups. A blood sample was taken before induction (T0), after induction but before pneumoperitoneum (T1), 15 minutes after pneumoperitoneum (T2), immediately after extubation (T3), and 30 minutes after extubation (T4). P-selectin-positive platelets and intercellular cell adhesion molecule-1 (ICAM-1)-positive lymphocytes, and plasma P-selectin, ICAM-1 and thrombomodulin (TM) levels were analyzed.
Results
Sevoflurane significantly increased P-selectin expression in platelets at T2, T3, and T4 and in plasma at T1, T2, T3, and T4, but it did not affect ICAM-1 and TM. Propofol had no significant effects on P-selectin, ICAM-1, and TM expression during anesthesia and surgery. P-selectin, ICAM-1, and TM expression was higher in the S compared with P group at T1, T2, and T3 for platelet P-selectin; T2 and T4 for plasma P-selectin; T1 and T2 for lymphocyte ICAM-1; and T1, T2, and T3 for plasma TM.
Conclusions
Propofol anesthesia can delay the inflammatory reactions during laparoscopic surgery and better maintain the structure stability and function in vascular endothelial cells.
Keywords
Introduction
In clinical practice, anesthesiologists often have patients who require strong stimulation and surgery such as laparoscopic cholecystectomy (LC). Sevoflurane and/or propofol are useful anesthesia methods for elective LC, but their effects on the inflammatory response in patients undergoing LC require further investigation. The inflammatory response induces leukocyte adhesion molecule expression including P-selectin (CD62P) and intercellular adhesion molecule 1 (ICAM-1) (CD54) on the surface of endothelial cells and an essential anticoagulant protein thrombomodulin (TM) (CD141) in the vasculature. 1 Vascular endothelial cells are mainly involved in hemostasis, coagulation, uptake cellular nutrient in the body, and regulating vasomotor function. 2 In addition, vascular endothelial cells undergo profound changes during systemic inflammatory response syndrome (SIRS), and activation and dysfunction of endothelial cells are central to the deterioration of systemic inflammatory response. 3 As general anesthetic drugs, sevoflurane and propofol have excellent properties such as fast onset, good controllability and rapid recovery. 4 In addition to the sedative and analgesic effects, both sevoflurane and propofol have certain anti-inflammatory effects that make it ideal for clinical application and for use in basic research.5,6
In this study, we observed and compared P-selectin, ICAM-1, and TM expression in the blood of patients undergoing LC during anesthesia using sevoflurane or propofol by flow cytometry and immunoenzymatic techniques. The study explored the different effects of sevoflurane and propofol on vascular endothelial cells during laparoscopic surgery. Our results may help to screen out the anesthetic drugs that effectively inhibit the traumatic inflammatory response and provide a theoretical basis for rational clinical anesthesia drug use.
Methods
Study design and subjects
This study was approved by the Ethics Committee of Zhongshan Hospital affiliated with Fudan University. Informed consent was obtained from each patient. Twenty-three patients undergoing LC were enrolled into this study, and they met the following inclusion criteria: weight ≥45 kg; 18 kg/m2 < BMI < 32 kg/m2; age 18 to 65 years; American Society of Anesthesiologists (ASA) physical status classification 1 to 2; and were scheduled to undergo LC. Preoperative exclusion criteria include the following: (1) history of hypertension, diabetes mellitus, or tumor; (2) severe cardiovascular and cerebrovascular diseases (e.g. congestive heart failure, myocardial infarction, or stroke); (3) severe liver or kidney dysfunction; or history of blood, embolic disease, or coagulopathy; (4) history of chronic infection, immune, or endocrine disease; or regular use of antiplatelet or anticoagulant drugs; (5) previous immunotherapy or endocrine therapy; (6) received blood transfusion or surgery in the last month; (7) pregnant or lactating woman; (8) preoperative white blood cell count and neutrophil percentage that were not within the normal range; (9) preoperative hemoglobin <80 g/L or abnormal blood coagulation; (10) postoperative mechanical ventilation time >30 minutes; or (11) the patient requested to withdraw from the study or their study participation was terminated because of surgical changes or intraoperative complications. Based on the requirements for this group sequential trial, patients undergoing elective LC who met the above criteria were randomly divided into two groups: sevoflurane anesthesia (S) and propofol anesthesia (P) groups.
Anesthetic technique
Anesthesiologists and surgeons
Four anesthesiologists and five surgeons with 3 to 10 years of the experience were involved in this study.
Pre-anesthesia medication and preparation
At this point, patients had not received preanesthetic medication. In the operating room, the patient was placed in the supine position. Routine cardiovascular monitoring was used, including electrocardiogram (ECG, lead II), pulse oximetry, and indirect arterial pressure (M1166A, Hewlett-Packard, Palo Alto, CA, USA). After the peripheral intravenous line was secured, lactated Ringer’s solution was administered at a rate of 5 mL/kg/hour. A continuous 256-s ECG was recorded in the awake stage.
Anesthesia induction
In the S group, the patient’s anesthesia was induced using a step-wise method for sevoflurane (S122H909, Baxter, Old Toongabbie, Australia) inhalation in oxygen using a facemask. Oxygen was administered for 3 minutes, then the face mask was connected to the sevoflurane-primed anesthetic circuit. The patient spontaneously breathed sevoflurane in oxygen with the sevoflurane vaporizer set at 8% and an oxygen flow rate 6 L/minute. In the P group, anesthesia was induced using target-controlled infusions (TCI) for propofol (to a target plasma concentration of 4 μg/mL) (GB544, AstraZeneca, Caponago, Italy) intravenously (Graseby infusion pump, Marcal Medical, Millersville, MD, USA). Anesthesia in both groups was maintained using a fentanyl (4 μg/kg) intravenous drip. After loss of consciousness, rocuronium was given to the patient (0.6 mg/kg) to induce intubation. When the end-expiratory concentration of sevoflurane reached 2.0 to 2.5 minimum alveolar concentration (MAC) in the S group or when the plasma concentration of propofol in the P group reached 2.5 to 3.0 μg/mL, a single-chamber endotracheal intubation was performed using a Glidescope laryngoscope (Bothell, WA, USA). After the tracheal tube was fixed, intermittent positive pressure ventilation was performed. The anesthesia machine parameters were as follows: tidal volume (VT) 8 mL/kg, respiratory frequency 10 cycles/minute, inspiration and expiration ratio 1:2, inhaled oxygen concentration 60%, and gas flow rate 1.2 L/minute.
Anesthesia maintenance
In the S group, the end-tidal concentration of sevoflurane was 1.0 to 1.5 MAC. In the P group, the target plasma concentration of propofol was set to 4.0 to 6.0 μg/mL by propofol TCI. In the S and P groups, fentanyl (0.05 mg/time) was added as needed to maintain the mean arterial pressure (MAP) of the patient at 60 to 100 mmHg and the heart rate at 60 to 80 beats/minute.
Anesthesia recovery
Patients in both the S and P groups had the drug discontinued when the incision was closed. The inhaled anesthetic was eluted at a flow rate of 6 L/minute. After the patient awaked and muscle tone was restored, the tube was removed.
Sample collection
Blood samples from patients in both the S and P groups were collected five times, as follows: before the induction of anesthesia (T0), after tracheal intubation but before pneumoperitoneum was established (T1), 15 minutes after the establishment of pneumoperitoneum (T2), immediately after extubation (T3), and 30 minutes after extubation (T4). Blood was collected from the median vein of the left arm elbow using a trocar. The first 2 to 3 mL of peripheral blood was discarded to avoid interference by the interstitial fluid, and then 3 mL of peripheral venous blood was collected in 3.8% sodium citrate anticoagulation tube after replacing the syringe.
Outcome measures
Characteristics of the patient
The following patient characteristics were recorded: name, gender, age, height, weight, ASA grade; preoperative white blood cell count and neutrophil percentage; operation time and anesthesia time; surgical bleeding volume; and intraoperative fentanyl dosage.
Detection of P-selectin, ICAM-1, and TM by ELISA
The anticoagulated blood (1 mL) was stored in a refrigerator at 4°C (generally within 24 hours; the shelf life was up to 3 days). After centrifugation at 1,000 rpm for 10 minutes, 50 μL of the supernatant (plasma) was taken for analysis. Commercial enzyme-linked immunosorbent assay (ELISA) kits were used to detect levels of P-selectin (Jining Biotechnology Co., Ltd, Shanghai, China), intercellular adhesion molecule-1 (ICAM-1) and thrombomodulin (TM) (Jiancheng Bioengineering Institute, Nanjing, China), in accordance with the corresponding manufacturers’ instructions.
Flow cytometry for detection of P-selectin-positive platelets and ICAM-1-positive lymphocytes
The anticoagulated blood (1 mL for P-selectin and 1 mL for ICAM-1) was fixed in an equal volume of 1% paraformaldehyde at 4°C for 30 minutes, and then stored at 4°C. Naturally precipitated platelet-rich plasma (PRP) (50 μL) was obtained. Platelets were washed twice with phosphate-buffered saline (PBS) with centrifugation at 3,000 rpm for 10 minutes. After re-suspension in 1 mL of PBS, platelets were adjusted to 1 × 107/mL. The platelet resuspension (50 μL) and fluorescein isothiocyanate (FITC)-labeled P-selectin monoclonal antibody (Becton Dickinson, San Jose, CA, USA) (10 μL) were added to the flow tube and incubated at room temperature for 30 minutes in the dark. For ICAM-1 detection, the blood (1 mL) was mixed with 6 mL of the red blood cell lysate, shaken well, and placed for 30 minutes. The mixture was centrifuged at 1,000 rpm for 10 minutes. The pelleted lymphocytes were washed twice with PBS (3,000 rpm for 10 minutes). Lymphocytes were resuspended in 1 mL of PBS, and then adjusted to 1 × 106/mL. The resuspension containing lymphocytes (50 μL) and the FITC-labeled ICAM-1 monoclonal antibody (Becton Dickinson) (10 μL) were added to the flow tube for incubation at room temperature for 30 minutes in the dark. After washing with PBS, platelets or lymphocytes were resuspended in 0.5 mL of PBS, respectively, and shaken for 1 hour. Platelets or lymphocytes were selected by forward light scattering (FSC) and lateral light scattering (SSC). Fluorescence detection was performed after logarithmic amplification to detect specific fluorescence signals on the surface of 5,000 to 10,000 platelets. Data were analyzed on an Apple Vision computer using Cell Quest Plot software (BD Biosciences, San Jose, CA, USA).
Statistical analysis
The data were statistically processed using SPSS version 16.0 (SPSS Inc., Chicago, IL, USA). The data were expressed as the mean ± standard deviation SD. The Student’s t-test was used to determine a significant difference between two groups. P < 0.05 was considered to be a significant difference and P < 0.01 was considered to be a very significant difference.
Results
No significant differences in patient characteristics between the S and P groups
Between 1 March 2010 and 31 March 2010, 30 patients met the trial criteria for LC (n = 15 in the S group, n = 15 in the P group). Among them, two patients in each group withdrew from the trial for personal or surgical reasons, and two patients who received sevoflurane anesthesia and one patient who received propofol anesthesia were withdrawn because of agglutinative blood samples after surgery. Therefore, the final analyses included 23 subjects (n = 11 in the S group, n = 12 in the P group). Subject characteristics were comparable between the two groups (Table 1). There were no significant differences in gender, age, body mass index, ASA grade, preoperative white blood cell count and percentage of neutrophils, operative and anesthesia time, surgical bleeding volume, and intraoperative fentanyl dosage.
Subject characteristics in the sevoflurane (S) and propofol (P) groups.

Note: BMI, body mass index; ASA, American Society of Anesthesiologists.
P-selectin levels increased in patients during surgery in the sevoflurane group
In the S group, P-selectin-positive platelets were investigated using flow cytometry and the results compared with T0 are as follows: 31.02±9.54 at T0, 38.75±10.01 at T1, 57.61±16.29 at T2 (P = 0.0001), 45.46±14.37 at T3 (P = 0.0116), and 50.91±19.43 mean fluorescence intensity (MIF) (P = 0.0064) at T4. The differences were significant at T2, T3, and T4. Therefore, the P-selectin-positive platelets from patients receiving sevoflurane anesthesia were gradually increased during anesthesia and surgery, with a peak at T2, and then a slight decrease at T3, followed by an increase at T4 (Figure 1a). P-selectin expression in PRP was determined by ELISA, and the results compared with T0 were as follows: 31.43±4.96 at T0, 37.02±5.03 at T1 (P = 0.0162), 39.27±4.31 at T2 (P = 0.0008), 37.19±5.83 at T3 (P = 0.0214), and 38.87±5.26 ng/mL (P = 0.0028) at T4. There were significant differences at T1, T2, T3, and T4. P-selectin expression levels in the peripheral blood were also gradually increased during anesthesia and surgery, with a peak at T2, a slight decrease at T3, and an increase at T4 (Figure 1b).

P-selectin, ICAM-1, and TM expression levels in patients during surgery in the sevoflurane (S) group (n=11). P-selectin-positive platelets (a) and ICAM-1-positive lymphocytes (c) were investigated using flow cytometry, and plasma P-selectin (b), ICAM-1 (d), and TM (e) levels were detected using ELISA at T0, T1, T2, T3, and T4 (see Methods). *, P < 0.05; **, P < 0.01. ICAM-1, intercellular adhesion molecule-1; TM , thrombomodulin; ELISA, enzyme linked immunosorbent assay
Almost no significant changes in ICAM-1 levels in patients during surgery in the sevoflurane group
In the S group, the ICAM-1-positive lymphocytes were investigated using flow cytometry and the results compared with T0 were as follows: 18.03±3.65 at T0, 19.94±3.37 at T1, 19.31±3.15 at T2, 19.12±3.76 at T3, and 18.69±3.18 MIF at T4. There were no significant differences (Figure 1c). Plasma ICAM-1 expression was determined by ELISA and the results compared with T0 were as follows: 13.59± 2.73 at T0, 14.03±3.21 at T1, 15.06±2.40 at T2, 14.72±1.81 at T3, and 16.10±2.71 ng/mL (P = 0.0427) at T4, which was the peak. The difference was only significant at T4 (Figure 1d).
No changes of TM levels in patients during surgery in the sevoflurane group
In the S group, plasma TM expression was determined using ELISA and the results compared with T0 were as follows: 13.09± 5.08 at T0, 13.05±5.43 at T1, 20.24±12.31 at T2, 22.45±16.09 at T3, and 17.95±11.03 ng/mL at T4. None of the differences were significant (Figure 1e).
Almost no significant changes in P-selectin levels in patients during surgery in the propofol group
In the P group, P-selectin-positive platelets were investigated using flow cytometry and the results compared with T0 were as follows: 30.01±8.03 at T0, 30.24±7.83 at T1, 37.82±7.37 at T2 (P = 0.0212), 34.08±7.23 at T3, and 38.92±16.26 MIF at T4 (Figure 2a). The P-selectin-positive platelets from patients receiving propofol anesthesia were slightly increased with anesthesia and surgery, with a peak at T2 that showed a significant difference. P-selectin expression in plasma was determined by ELISA, and the results compared with T0 were as follows: 32.15±4.43 at T0, 33.84±3.63 at T1, 34.88±4.37 at T2, 34.73±5.14 at T3, and 34.70±4.12 ng/mL at T4. There were no significant differences (Figure 2b).

P-selectin, ICAM-1, and TM expression levels in patients during surgery in the propofol (P) group (n=12). P-selectin-positive platelets (a) and ICAM-1-positive lymphocytes (c) were investigated using flow cytometry, and plasma P-selectin (b), ICAM-1 (d), and TM (e) levels were detected by ELISA at T0, T1, T2, T3, and T4 (see Methods). *, P<0.05; **, P<0.01. ICAM-1, intercellular adhesion molecule-1; TM , thrombomodulin; ELISA, enzyme linked immunosorbent assay
No significant changes in ICAM-1 levels in patients during surgery in the propofol group
In the P group, ICAM-1-positive lymphocytes were investigated using flow cytometry, and the results compared with T0 were as follows: 16.69±1.42 at T0, 16.71±2.51 at T1, 16.38±2.45 at T2, 16.19±3.15 at T3, and 16.11±2.94 ng/mL at T4 MIF at T4. There were no significant differences (Figure 2c). Plasma ICAM-1 expression was determined by ELISA and the results compared with T0 were as follows: 13.64±3.42 at T0, 13.92±3.87 at T1, 13.96±4.25 at T2, 15.50±4.32 at T3, and 14.12±4.37 ng/mL at T4. There were no significant differences (Figure 2d).
TM expression levels in patients in P group during surgery
In the P group, plasma TM expression was determined by ELISA, and the results compared with T0 were as follows: 10.24±6.38 at T0, 9.15±2.83 at T1, 11.53±3.64 at T2, 12.43±3.02 at T3, and 11.38±3.63 ng/mL at T4. There were no significant differences (Figure 2e).
Increase in P-selectin-positive platelets in patients during surgery in the sevoflurane group but not in the propofol group
Using flow cytometry, P-selectin-positive platelet results in the S and P groups were as follows: 31.02±9.54 and 30.01±8.03 at T0, 38.75±10.01 and 30.24±7.83 at T1, 57.61±16.29 and 37.82±7.37 at T2 (P = 0.0010), 45.46±14.37 and 34.08±7.23 at T3 (P = 0.0241), and 50.91±19.43 and 38.92±16.26 MIF at T4. There were significant differences at T1, T2, and T3 (Figure 3a). Using ELISA, plasma P-selectin levels in patients in the S and P groups were 31.43±4.96 and 32.15±4.43 at T0, 37.02±5.03 and 33.84±3.63 at T1, 39.27±4.31 and 34.88±4.37 at T2 (P = 0.0245), 37.19±5.83 and 34.73±5.14 at T3, and 38.87±5.26 and 34.70±4.12 ng/mL at T4 (P = 0.0455). There were significant differences at T2 and T4 (Figure 3b). The results suggest that sevoflurane but not propofol-induced anesthesia increases P-selectin expression levels.
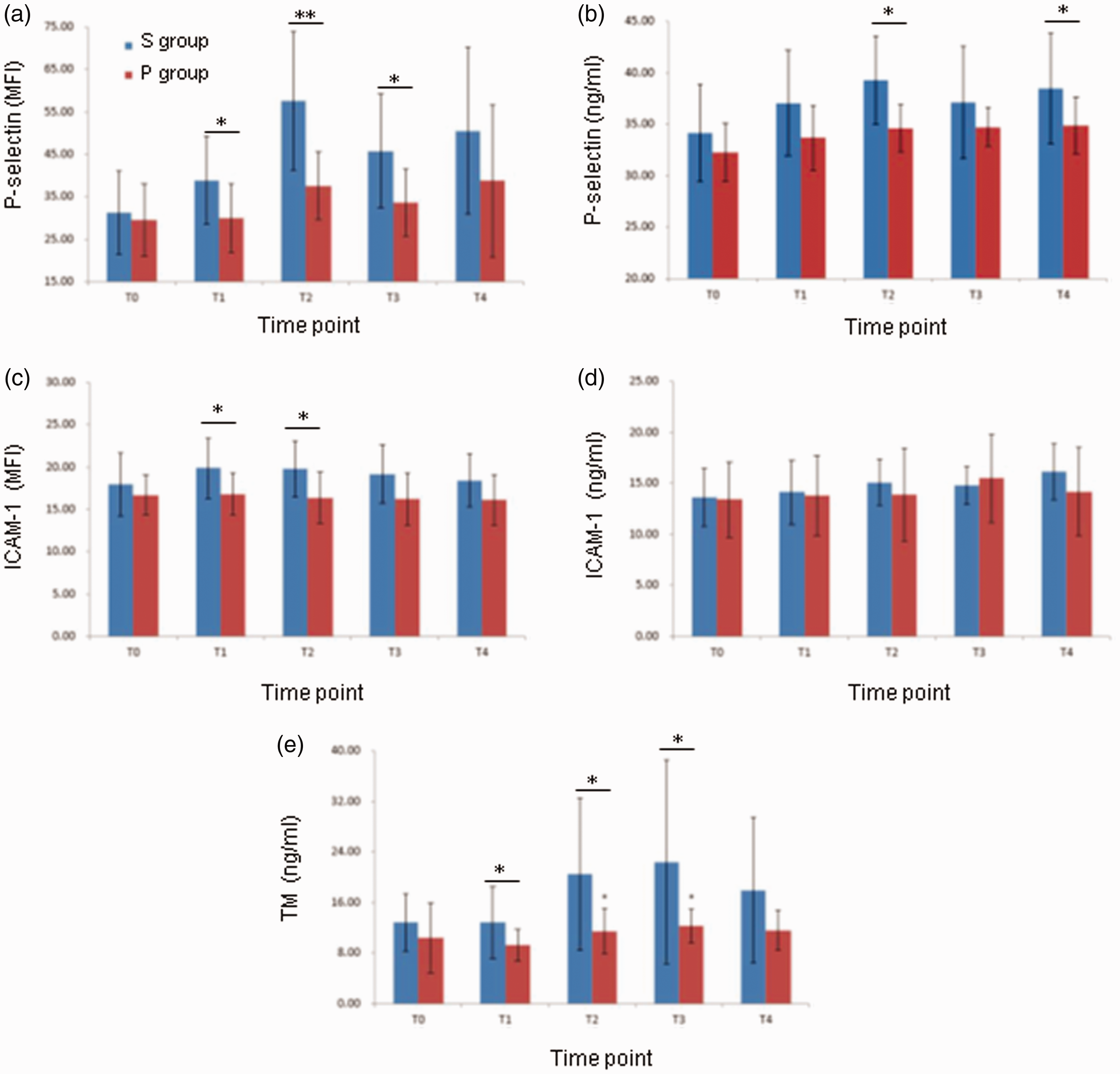
Comparison of P-selectin, ICAM-1, and TM levels in patients during surgery in the sevoflurane (S) (n=11) and propofol (P) (n=12) groups. P-selectin-positive platelets (a) and ICAM-1-positive lymphocytes (c) were investigated using flow cytometry, and plasma P-selectin (b), ICAM-1 (d), and TM (e) levels were detected by ELISA at T0, T1, T2, T3, and T4 (see Methods). *, P<0.05; **, P<0.01. ICAM-1, intercellular adhesion molecule-1; TM , thrombomodulin; ELISA, enzyme linked immunosorbent assay
A slight increase in ICAM-1 levels in patients during surgery in the sevoflurane group but not in the propofol group
Using flow cytometry, the ICAM-1-positive lymphocytes in the S and P groups were as follows: 18.03±3.65 and 16.69±1.42 at T0, 19.94±3.37 and 16.71±2.51 at T1 (P = 0.0159), 19.31±3.15 and 16.38±2.45 at T2 (P = 0.0207), 19.12±3.76 and 16.19±3.15 at T3, and 18.69±3.18 and 16.11±2.94 MIF at T4. There were significant differences at T1 and T2 (Figure 3c). Using ELISA, plasma ICAM-1 expression levels in patients in the S and P groups were 13.59±2.73 and 13.64±3.42 at T0, 14.03±3.21 and 13.92±3.87 at T1, 15.06±2.40 and 13.96±4.25 at T2, 14.72±1.81 and 15.50±4.32 at T3, and 16.10±2.71 and 14.12±4.37 ng/mL at T4. There were no significant differences (Figure 3d). The results suggest that sevoflurane slightly increases ICAM-1 expression levels compared with propofol.
The increase in TM levels in patients during surgery in the sevoflurane group but not in the propofol group
Using ELISA, plasma TM expression levels in patients in the S and P groups were as follows: 13.09±5.08 and 10.24±6.38 at T0, 13.05±5.43 and 9.15±2.83 at T1, 20.24±12.31 and 11.53±3.64 (P = 0.0239) at T2, 22.45±16.09 and 12.43±3.02 at T3 (P = 0.0460), and 17.95±11.03 and 11.38±3.63 ng/ml at T4. There were significant differences at T1, T2, and T3 (Figure 3e). The results suggest that sevoflurane but not propofol used for anesthesia increases TM expression levels.
Discussion
In the present study, we investigated the changes in the inflammatory response by measuring the endothelial cell activation and damage markers (P-selectin, ICAM-1, and TM) in the blood of patients undergoing LC using sevoflurane or propofol anesthesia. Our results showed that sevoflurane significantly increased P-selectin expression levels, but there were no effects on ICAM-1 and TM during the anesthesia and surgery periods; propofol showed no significant effects on P-selectin, ICAM-1, and TM expression. However, P-selectin, ICAM-1, and TM expression levels in the S group were all higher compared with those in the P group, with significant differences at some time points during anesthesia and surgery. Our results showed different effects of sevoflurane and propofol anesthesia on inflammatory and anti-inflammatory responses.
Under normal circumstances, P-selectin and ICAM-1, which belong to the family of vascular adhesion molecules, are either not expressed or expressed only a small amount on the surface of endothelial cells. Sevoflurane, similar to inflammatory factors such as tumor necrosis factor (TNF)-α and endotoxin, might stimulate endothelial cells to express P-selectin and ICAM-1, which promote the adhesion of neutrophils and vascular endothelial cells for the inflammatory response. 7 As a thrombin receptor that is synthesized by vascular endothelial cells, TM detaches from the cell membrane surface and releases when the vascular endothelial cells are damaged; thus, the plasma soluble TM levels are increased. 8 We did not observe significant changes in TM expression level in patients with sevoflurane anesthesia, which may indicate potential pathological changes in the endothelial cells and changes in vascular endothelial cell function.9,10
We did not observe significant changes in P-selectin, ICAM-1, and TM expression in the blood of patients undergoing LC with propofol anesthesia compared with the pre-operative resting state. The results indicate that propofol might not induce an inflammatory response, but sevoflurane anesthesia induces functional changes in endothelial cells.11–13 Therefore, we showed that patients undergoing LC using propofol anesthesia had a lower inflammatory response during surgery. Propofol might help to maintain the structure and function of endothelial cells.
Some drugs with potential anti-inflammatory effects were found in some in vitro studies,14–16 but most of these drugs could not work together with the anti-inflammatory system. However, propofol has a similar in chemical structure as the endogenous antioxidant vitamin E and the known antioxidant-butylated hydroxytoluene. 17 Therefore, propofol may be transferred by hydrogen atoms and react via lipid peroxidation to form a relatively stable propofol phenolic group and a lipid hydroperoxide, and thereby, it could play a role in exerting anti-inflammatory and anti-oxidation effects. In addition, propofol inhibits cytokine expression that is associated with adhesion molecules, which is the most direct mechanism to inhibit endothelial cell activation.18,19
In conclusion, we showed that, in patients undergoing LC, sevoflurane anesthesia increases plasma P-selectin and ICAM-1 levels but not TM levels during the anesthesia and surgery periods. We also showed that propofol anesthesia does not significantly affect P-selectin, ICAM-1, or TM levels; however, P-selectin, ICAM-1, and TM levels in the S group are all higher compared with those in the P group. Our findings suggest that propofol anesthesia can delay the occurrence and development of inflammatory reactions during laparoscopic surgery, and it better maintains the structure stability and function in vascular endothelial cells. We will continue to improve our experiments, including increasing the sample size, investigating additional types of surgery, and assessing more inflammatory and anti-inflammatory markers.