
Abstract
Drowning is a common cause of childhood morbidity and mortality worldwide. Anoxia, hypothermia, and metabolic acidosis are mainly responsible for this morbidity. Drowning may lead to multiple organ damage, especially cardiac damage, in cases in which severe hypothermia and hypoxemia occur. We report a case of a 4-year-old girl who was admitted to our hospital’s Emergency Department because of drowning. She had elevated troponin I concentrations and ST-segment elevation with T wave inversion. However, cardiovascular computed tomography showed no obvious abnormalities in the coronary arteries. We suggest that cardiac damage in this situation is caused by coronary artery spasms. To the best of our knowledge, this is the first case of cardiac damage with electrocardiographic changes after drowning in a preschool child.
Introduction
Drowning is a major cause of morbidity and mortality worldwide, predominately affecting low- and middle-income countries.1,2 The pathophysiological changes of drowning mainly include anoxia, hypothermia, and metabolic acidosis. 3 Drowning may lead to multiple organ damage, and the most immediate threat in drowning is dysfunction of the cardiac and central nervous systems, particularly in cases of severe hypothermia and hypoxemia. 4 Despite improvement in the management of drowning,5,6 the prognosis of serious drowning in patients remains closely associated with the occurrence of drowning-related cardiac injury. 6 During cardiac injury, a series of abnormalities may appear on an electrocardiogram. The current report presents a child case of coronary spasm after drowning in whom electrocardiographic (ECG) results showed ST-segment elevation with T wave inversion, which mimicked acute myocardial infarction.
Case presentation
This case report was approved for publication by the local Ethics Committee of the Children’s Hospital of Soochow University (approval number: 2020CS076). We have de-identified the details of this patient and obtained the patient's verbal consent for treatment and publication. The reporting of this study conforms to the CARE guidelines. 7
A 4-year-old girl was admitted to the intensive care unit of our hospital because of drowning in cold water in August 2018. The child fell into a river at approximately 6:00 pm, and she was pulled out by her parents within 1 minute after falling into the water. After being rescued, she was conscious but short of breath, accompanied by coughing. She had a fever the next early morning. She was taken to our hospital and admitted to the Emergency Department. Her parents reported that she had no medical history. Upon arrival, the girl was conscious, with a transtympanic body temperature of 35.7°C, a heart rate of 167 beats/minute, a respiratory rate of 54 breaths/minute, a blood pressure of 107/63 mmHg, and an O2 saturation of 92%.
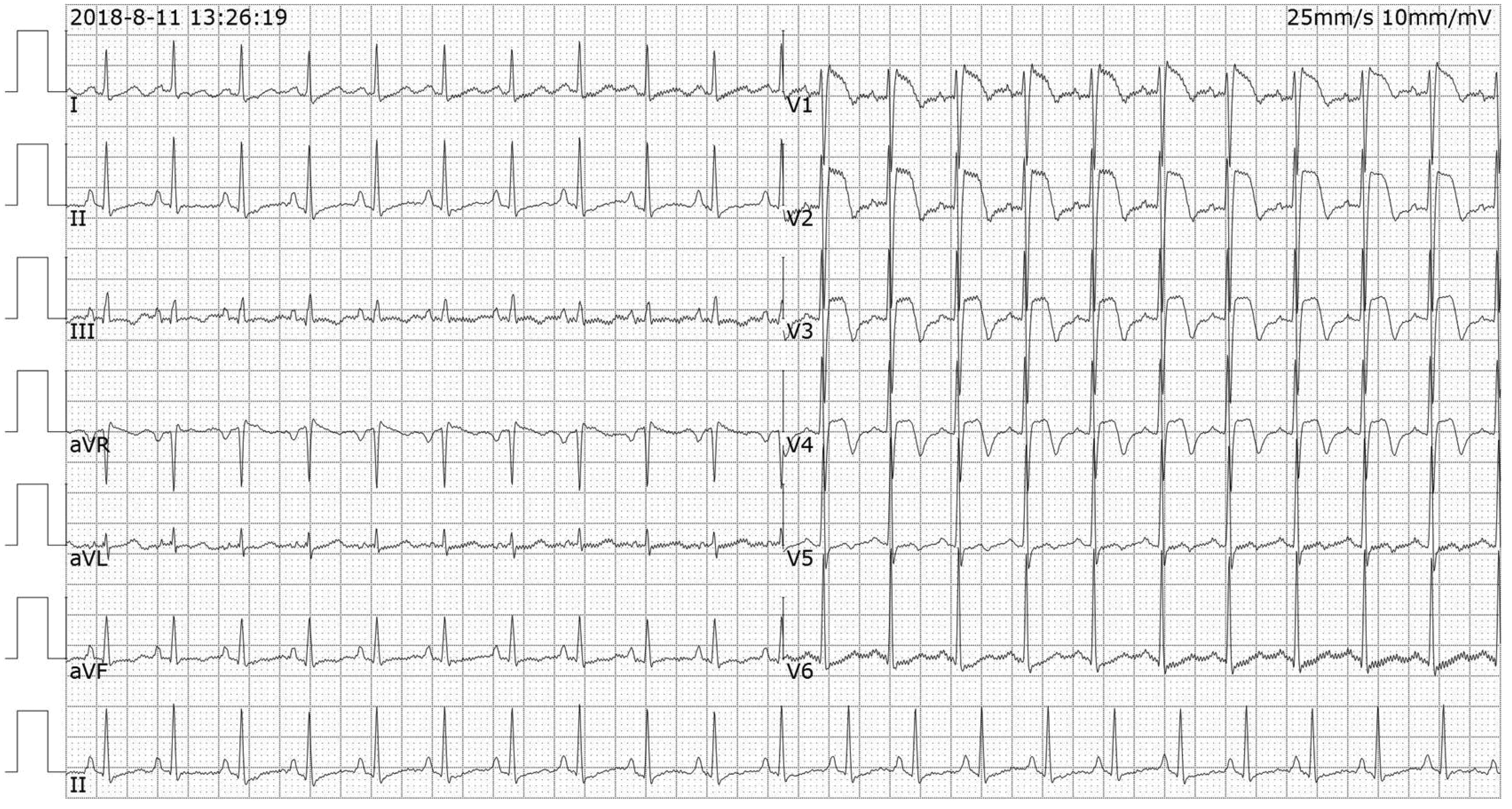
Routine blood tests showed an elevated white blood cell count (18.51 × 109/L) with a high neutrophil ratio (84%). The patient’s high-sensitivity C-reactive protein concentration was 18.57 mg/L. Urinary and feces routine parameters, liver and kidney function, electrolytes, procalcitonin, blood ammonia, and coagulation routine parameters were normal. An emergency ECG showed sinus tachycardia and ST-segment elevation in leads V1–V3 with T wave inversion (Figure 1). An echocardiogram also showed an enlarged right atrium and right ventricle (Figure 5a), poorly coordinated ventricular septum, and left ventricular posterior wall movement, with mild to moderate tricuspid regurgitation and tachycardia. A chest computed tomography scan showed multifocal patchy shadows in both lungs and localized thickening of the left lung pleura, which suggested drowning-related lung injury. Local bone attached to the left side of the cervical spine was rough, and the transverse foramen was large. A head computed tomography scan showed no obvious abnormalities.

Electrocardiogram on admission.
Electrocardiogram 11 hours after admission.
The following laboratory results were detected. The troponin I concentration was 8.06 ng/mL (0.0–0.09 ng/mL), creatinine kinase-MB concentration was 77.2 ng/mL (0.0–3.7 ng/mL), and myoglobin concentration was 202.1 ng/mL (11.6–73.0 ng/mL). The serum sodium concentration was 138 mmol/L (136–145 mmol/L) and the serum potassium concentration was 3.6 mmol/L (3.5–5.2 mmol/L). The blood urea concentration was 4.16 mmol/L (2.9–8.2 mmol/L), blood creatinine concentration was 23.8 µmol/L (45–84 µmol/L), blood glucose concentration was 7.5 mmol/L (3.92–6.44 mmol/L), blood aspartate aminotransferase (AST) concentration was 96.7 U/L (10–67 U/L), and blood alanine aminotransferase (ALT) concentration was 25.5 U/L (5–35 U/L). The pH was 7.514 (7.35–7.45) and PaCO2 was 20.7 mmHg (36–44 mmHg).
After admission, the patient was immediately provided high-flow oxygen inhalation (10 L/minute), vitamin C (3 g, once daily), and creatine phosphate (1 g, once daily) to protect the myocardium. The girl’s troponin I concentration increased to 12.92 ng/mL 11 hours after admission (Table 1). ST-segment saddleback morphology in V1–V3 leads could still be detected in her ECG 12 hours after admission (Figure 2). On the third day after admission, her troponin I concentration was decreased to 2.27 ng/mL (Table 1), and the ST-segment arch-type elevation in her ECG was improved (Figure 3). In addition, cardiovascular computed tomography at 7 days after admission showed that there were no obvious abnormalities in the coronary arteries, and her troponin I concentrations had returned to the normal range (Table 1). After 10 days, there was no obvious ST-T segment change on an ECG (Figure 4), and the right atrium and ventricle returned to a normal size as shown by an echocardiogram (Figure 5b). The girl was diagnosed with near-drowning and myocardial injury, and discharged from the hospital 10 days after admission.
Changes in myocardial injury biomarkers during hospitalization.

CK-MB, creatine kinase-MB; cTnI, cardiac troponin I.

Electrocardiogram on the third day after admission.

Electrocardiogram on the 10th day after admission.

Echocardiogram on admission (a) and 10 days after admission (b).
Discussion
Drowning is a major public health problem, especially in children.8–10 Papadodima et al. retrospectively analyzed 197 drowning cases by autopsy and through laboratory examinations, and found that 23 patients died because of complications of coronary artery disease. 11 This finding suggests that cardiovascular complications after drowning induce cardiovascular damage, including coronary artery injury. Myocardial infarction after drowning was also reported in an 82-year-old male patient. 12 However, to date, limited studies on cardiovascular damage after drowning in children have been published. Omar et al. reported a 16-year-old boy who was rescued after drowning for 15 minutes, and his ECG showed acute myocardial infarction. 13 The boy eventually died. Cardiovascular effects are secondary to hypoxia and hypothermia in drowning cases. 14 Therefore, the exposure times of hypoxia and hypothermia are essential factors in determining the degree of cardiovascular damage in drowning cases. In the present case, the child drowned for approximately 1 minute, which is a short time, and her temperature and blood oxygen saturation were not considerably decreased on admission. Therefore, the abnormal ECG, elevated troponin I concentrations, and myocardial enzyme spectrum were most likely due to coronary artery spasm rather than myocardial infarction.
There are several reasons that may underlie the mechanism for coronary artery spasm after drowning. First, a drowning patient's sudden exposure to cold water stimulates the vagus nerve, which results in a prolonged Q-T interval. 15 Second, a large amount of catecholamine release 16 may cause coronary artery spasm. Third, the fluid inhaled from the respiratory tract after drowning greatly impairs gas exchange, inactivates lung surfactants, and causes reflex laryngospasm, leading to respiratory disturbance and hypoxia. Hypoxemia causes tissue hypoxia and coronary artery spasm. 17 In addition, coronary spasm may also be emotionally induced owing to extreme distress during the drowning process. 18 Coronary artery spasm can cause different degrees of myocardial ischemia, and severe cases can cause myocardial infarction or even death.
Conclusion
Drowning is a major cause of morbidity and mortality. ST-segment elevation, which is highly specific for primary ischemic heart diseases, may also occur in children with near-drowning without primary ischemic heart disease. Therefore, monitoring dynamic changes in the ECG, myocardial enzymes, cardiac troponin concentrations, and echocardiography may help to differentiate ST-segment elevation due to coronary spasm after drowning from acute myocardial infarction.
Footnotes
Author contributions
Jianmin Zhang, Haitao Lv, and Miao Hou designed the study; Jianmin Zhang, Yunjia Tang, and Miao Hou wrote the manuscript; Jianmin Zhang and Xue Jiang collected the clinical information; Haitao Lv revised the manuscript; all authors have read and approved the final manuscript.
Data availability statement
The data of this study are available from the corresponding author upon reasonable request
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors