
Abstract
A man in his late 60s with a history of angina pectoris developed low back pain during cardiac catheterization. During this episode of back pain, ST segment elevations were noted on the electrocardiogram. The patient reported relief of the pain immediately after implantation of two drug-eluting stents, and the ST segments on the electrocardiogram normalized. The probable mechanisms of low back pain during cardiac catheterization in this patient are briefly outlined.
Keywords
Introduction
The typical manifestation of myocardial ischemia is precordial chest pain that is induced by exertion and relieved by rest or nitroglycerin. Case reports of atypical angina have described the involvement of uncommon body locations, such as angina pectoris or acute myocardial infarction with headache, 1 craniofacial pain, 2 orofacial pain, 3 neck pain, 1 pharyngeal pain, 1 belching, 4 low back pain, 5 hip pain, axillary pain, or paroxysmal hypertension as the main manifestations. There are no clear data on the incidence of low back pain during angina attacks, but several case reports have described myocardial infarction accompanied by low back pain as the main complaint.
We herein describe a patient with angina pectoris who developed low back pain during cardiac catheterization. The clinical presentation and probable mechanisms of low back pain during cardiac catheterization are discussed. We hope this case report will raise clinicians’ awareness regarding this uncommon symptom in patients with similar presentations.
Case report
A man in his late 60s with a 7-year history of episodic chest pain and chest distress underwent percutaneous coronary intervention (PCI). Coronary angiography (CAG) revealed total occlusion of the proximal left anterior descending artery, 70% to 80% stenosis of the left circumflex artery, and 50% to 60% stenosis of the right coronary artery (RCA). A stent was implanted to relieve the occlusion of the left anterior descending artery (Figure 1(a)–(c)). His coronary risk factors were type 2 diabetes and hyperlipidemia.

Coronary angiography performed 4 years previously. (a) Total occlusion of the proximal left anterior descending artery (arrow). (b) Stenosis of 70% to 80% stenosis in the left circumflex artery (arrow) and (c) Stenosis of 50% to 60% in the right coronary artery (arrow).
Four years later, the patient was admitted to our hospital because of symptom aggravation. His physical examination findings were normal. A 12-lead electrocardiogram at rest revealed normal sinus rhythm and no significant ST segment change; however, Q-waves were present in leads II, III, and aVF. Echocardiography demonstrated a segmental motion abnormality of the left ventricular wall, and the left ventricular ejection fraction was 59.2%. We obtained the patient’s written consent to perform cardiac catheterization for identification of any coronary artery lesions. During the surgery, we observed no in-stent restenosis. Plaques were present in the left main stem, and diffuse stenosis (70%) was present in the proximal and middle segments of the left circumflex artery. An ulcerated plaque was observed in the proximal RCA, and 80% stenosis was noted at the second turn (Figure 2(a)–(c)).

Coronary angiography performed in present case. (a) No in-stent restenosis in left anterior descending artery. (b) Diffuse stenosis (70%) in the proximal and middle segments of the left circumflex artery. (c) Ulcerated plaque in the proximal right coronary artery and 80% stenosis (arrow) at the second turn of the right coronary artery and (d) Two 3.0- × 18-mm and 3.5- × 19-mm drug-eluting stents implanted in the right coronary artery.
During dilation of the RCA lesion, the patient suddenly felt pain in the lower back. An instant electrocardiogram showed ST segment elevation in leads II, III, and aVF (Figure 3(a)). After intravenous injection of morphine hydrochloride and nitroglycerin, 3.0- × 18-mm and 3.5- × 19-mm drug-eluting stents were implanted in the RCA. The patient’s low back pain was relieved, and the ST segment normalized in leads II, III, and aVF (Figure 3(b)). After coronary revascularization, TIMI grade 3 flow was achieved with no residual stenosis, dissection, or side branch occlusion. Optical coherence tomography showed excellent stent apposition.
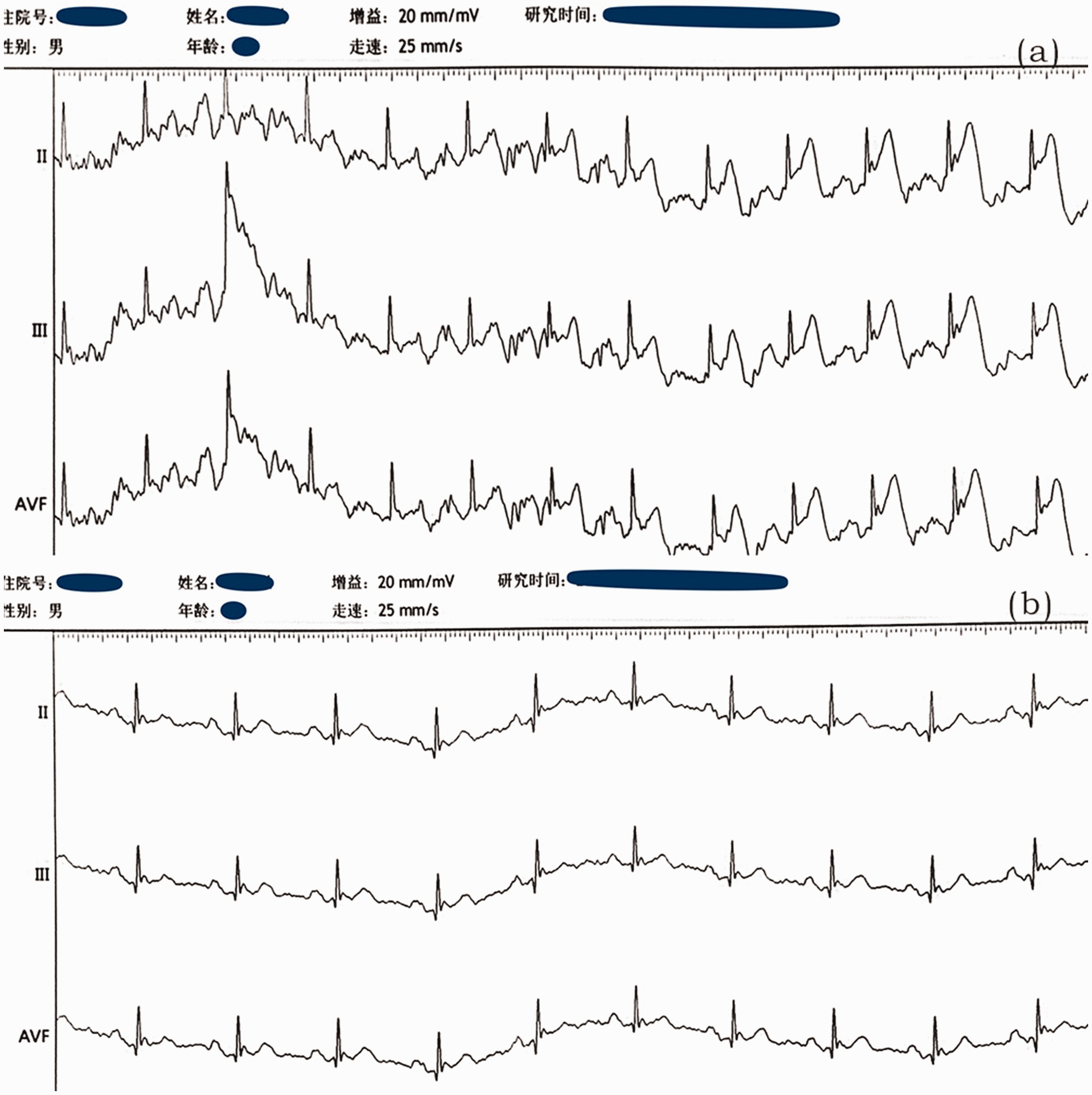
Changes in electrocardiogram during coronary angiography. (a) ST segment elevation in leads II, III, and aVF and (b) Normalized ST segment in leads II, III, and aVF.
Written informed consent was obtained from the patient for publication of this article. All patient details have been deidentified. This manuscript has been reviewed and approved by the ethics committee of The Second Hospital of Hebei Medical University. This report adheres to the CARE guidelines. 6
Discussion
In this case report, we analyzed the possible relationship between low back pain and coronary heart disease and considered why the low back pain was induced by CAG. Four possible mechanisms are as follows.
Coronary heart disease combined with atherosclerosis of the abdominal aorta or lumbar artery: Occlusion or stenosis of the lumbar artery or lumbar arterioles can cause persistent low back pain.7,8 Intervertebral disc degeneration resulting from occlusion of the middle sacral artery and subsequent lumbar ischemia is another possible cause of long-term low back pain.
9
Aortic or coronary artery dissection during CAG: Arterial dissection can manifest as progressively worsening chest pain,10,11 which is typically described as abrupt in onset and tearing in nature.
12
Intraoperative peripheral embolism: Air emboli, thrombosis, platelet aggregation, detachment of atherosclerotic plaques,13–15 and formation of cholesterol crystals during CAG can cause peripheral embolism.16,17 Peripheral embolism mainly manifests as sudden pain, limb pallor, and disappearance of peripheral artery pulsation, whereas the typical symptoms of cholesterol embolism are limb pain and skin manifestations. Femoral access PCI may cause low back pain, which may occur when the sheath enters the cardiovascular space.
18
In the present case, we performed transradial PCI, and the low back pain was not persistent. The pain appeared immediately after dilation of the balloon and was significantly relieved after implantation of the stents. The low back pain was considered closely related to myocardial ischemia. In the 1980 s, the horseradish peroxidase technique was used to investigate the segmental distribution of visceral afferent neurons of the cardiac nerve in cats. 19 The study revealed the presence of labeled dorsal root ganglion cells in the spinal cord segments from C7 to T7, and the distribution varied greatly among animals. 19
The afferent nerve fibers of the subcortical nerves that project to the spinal cord segments are much wider than previously thought.19,20 Research has shown that some human cardiac sympathetic nerves are distributed in the lower sympathetic ganglia and that angina pectoris can be projected to the corresponding dermatomes, 20 which include the lower back.
Conclusion
Uncommon symptoms of angina pectoris, such as paroxysmal low back pain in this case, should be taken seriously by clinicians to prevent the development of a critical clinical condition.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231187946 - Supplemental material for Attack of angina pectoris with low back pain alone: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605231187946 for Attack of angina pectoris with low back pain alone: a case report by Fang Duan, Shuoyuan Ji, Guoqiang Gu, Demin Liu and Wei Cui in Journal of International Medical Research
Footnotes
Acknowledgements
The authors would like to thank all members of the study team as well as the patient and his family.
Author contributions
Fang Duan collected the patient’s information and drafted the manuscript. Shuoyuan Ji and Demin Liu edited the manuscript. Guoqiang Gu collected the figures. Wei Cui provided guidance for the literature search. All authors have read and agreed to the published version of the manuscript.
Data availability statement
The datasets used for the current case report are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.