
Abstract
Objective
To retrospectively compare the differences in the surgical efficacy and prognosis of laparoscopic pyeloplasty for hydronephrosis caused by symptomatic versus asymptomatic ureteropelvic junction obstruction (UPJO) in children and determine whether clinical symptoms affect the surgical outcome and prognosis.
Methods
Children who underwent laparoscopic pyeloplasty in our hospital from January 2018 to December 2022 were retrospectively analyzed. The children were divided into symptomatic and asymptomatic groups according to their main symptoms. The primary outcomes were the surgical success rate, change in renal parenchymal thickness, and change in renal pelvis anteroposterior diameter. The secondary outcomes were postoperative complications, reoperation rate, operative duration, intraoperative blood loss, and drainage tube indwelling time.
Results
In total, 224 children with UPJO were enrolled; 148 (66.1%) were symptomatic and 76 (33.9%) were asymptomatic. The symptomatic group showed a significantly greater mean change in renal parenchymal thickness, significantly higher surgical success rate, and significantly lower postoperative complication rate.
Conclusions
In the present study, asymptomatic children had a lower surgical success rate, less postoperative imaging improvement, and more postoperative complications than symptomatic children. The presence or absence of clinical symptoms may affect the surgical outcome and prognosis.
Introduction
Hydronephrosis is defined as swelling and dilatation of the kidneys due to urine buildup, and it is usually caused by blockage of the free flow of urine from the kidneys. 1 Ureteropelvic junction obstruction (UPJO) is the main cause of congenital hydronephrosis. 1 Its clinical manifestations include lateral abdominal pain, hematuria, urinary tract infection, renal insufficiency, nausea, hypertension, an increased creatinine concentration, and an abdominal mass. However, UPJO may also be incidentally diagnosed in patients with no symptoms. 2 UPJO can be divided into intrinsic and extrinsic obstruction. Intrinsic obstruction is characterized by disrupted development of the muscular tissue of the ureter or abnormal development of the collagen fibers separating the muscle fibers. Both of these problems result in the inability of the ureter to contract. Extrinsic obstruction is caused by lower-pole crossing vessels, adhesions of fibrous bands, and kinks at the normal ureteropelvic junction, among other abnormalities.3,4 If left untreated, obstruction can lead to progressive renal damage and subsequent renal failure. 5 Since its description by Anderson and Hynes 6 in 1949, dismembered pyeloplasty has been considered the gold standard procedure for the treatment of both endogenous and exogenous UPJO, 7 and it can be performed in an open, purely laparoscopic, or robot-assisted manner. 8 The main goal of treatment is to maintain or improve renal function. 9 Many studies have proven the safety and effectiveness of laparoscopic pyeloplasty (LP) in children, and the reported success rate of LP is >90%.10–12
Nevertheless, a considerable number of children develop recurrent disease after surgery, and urological studies in adults indicate that clinical symptoms are among main factors affecting the development of postoperative hydronephrosis. However, the sample sizes of relevant studies are small, and there is a lack of studies involving children. The present study was performed in an effort to fill these knowledge gaps.
Methods
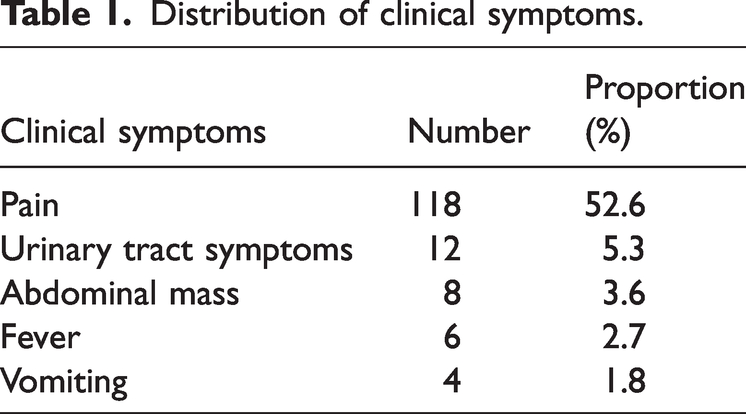
This retrospective analysis involved 224 children who underwent LP by the same surgeon in our hospital from January 2018 to December 2022. Urinary ultrasonography was performed at 1, 3, 6, and 12 months after LP. The postoperative renal parenchymal thickness (PT) and the anteroposterior diameter of the renal pelvis were collected. Other information collected included patient demographics, preoperative examination findings, and postoperative outcomes. For inclusion in the study, the patients were required to have both preoperative and postoperative complete data and documentation of their major symptoms. The enrolled children were divided into a symptomatic group and asymptomatic group according to the presence or absence of clinical symptoms, including but not limited to pain, an abdominal mass, vomiting, hematuria, infection (Table 1). The inclusion criteria were an age of 3 to 14 years, treatment by LP, diagnosis of primary endogenous UPJO by postoperative pathology, and follow-up of ≥6 months. Children with other diseases and those who underwent secondary surgery were excluded. To prevent retrospective bias caused by unclear chief complaints of younger children, children aged <3 years were excluded.
Distribution of clinical symptoms.
All patients had at least one of the following surgical indications: the presence of clinical symptoms related to hydronephrosis, such as pain or urinary tract infection; initial evaluation showing renal function on the affected side to be <40% with a renal tubular half-life of >20 minutes; aggravation of hydronephrosis or persistent hydronephrosis accompanied by thinning of the renal parenchyma, detected via ultrasound follow-up; decline in split renal function of greater than 5% to 10%, detected via renal radionuclide imaging; renal PT of <0.4 cm; and anteroposterior diameter of the renal pelvis of >3.0 cm, or >2.0 cm with calyceal dilatation.
Surgical success was defined as a reduction in clinical symptoms accompanied by improvement in the renal PT and anteroposterior diameter of the renal pelvis at the 6-month follow-up without the need for secondary surgery.
For protection of patient privacy, all patients’ detailed personal information has been deleted. This article is reported in accordance with the STROBE statement. 13
Statistical analysis
Statistical analyses were performed to compare the demographics, surgical success rate, postoperative symptoms, and radiological findings between the two groups. The Shapiro–Wilk test and graphics were used to evaluate whether quantitative data were normally distributed. Measurement data with a normal distribution are presented as mean ± standard deviation and were compared using an independent-samples t test. Measurement data with a non-normal distribution are presented as median and interquartile range and were compared using the Mann–Whitney U test. Pearson’s chi-square test or Fisher’s exact test was used to compare the distributions of categorical variables between the groups. IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis, and a p value of <0.050 was considered statistically significant.
Results
In total, 224 children with at least 6 months of follow-up were included in the study. The children comprised 88 (78.6%) boys and 24 (21.4%) girls. Left LP was performed in 170 (75.9%) patients and right LP in 54 (24.1%). The symptomatic group comprised 148 (66.1%) children, and the asymptomatic group comprised 76 (33.9%) children. The median age at surgery was 71 (45–107.75) months, the median weight was 23.25 (17.93–34.0) kg, and the median follow-up time was 10.0 (7.0–15.0) months (Table 2).
Patient characteristics and preoperative parameters.

Data are presented as median (range) or n (%).
Mann–Whitney U test.
Pearson chi-square test.
The mean operation time was significantly shorter in the asymptomatic than symptomatic group (140.0 ± 43.0 vs. 160.23 ± 48.82 minutes, respectively; p = 0.041). Additionally, the median body weight was significantly lower in the asymptomatic than symptomatic group [18.75 (16.38–24.6) vs. 28 (19–137) kg, respectively; p < 0.01] (Table 2). The asymptomatic and symptomatic groups showed no significant difference in intraoperative blood loss [5.0 (5.0–6.5) vs. 5.0 (5.0–10.0) mL, respectively], length of hospital stay (12.82 ± 3.1 vs. 13.68 ± 3.15 days, respectively), or postoperative drainage tube indwelling time (5.03 ± 1.33 vs. 4.98 ± 1.23 days, respectively) (Table 3). The preoperative renal PT of the two groups was also comparable [0.5 (0.4–0.8) vs. 0.5 (0.3–0.85) cm, respectively]. There was a statistically significant difference in the change in PT between the symptomatic and asymptomatic groups (0.32 ± 0.26 vs. 0.11 ± 0.13 cm, respectively; p < 0.01) (Table 4). The preoperative anteroposterior width of the renal pelvis was also significantly different between the symptomatic and asymptomatic groups [3.20 (2.10–4.03) vs. 2.40 (1.70–3.23) cm, respectively; p = 0.013]. The recovery of the anteroposterior diameter in the symptomatic group was significantly better than that in the asymptomatic group (p < 0.01) (Table 5). The success rate of surgery was 96.0% in the symptomatic group and 78.9% in the asymptomatic group, with a statistically statistical difference (p = 0.012). Two patients in the symptomatic group developed urinary tract infection and hematuria as postoperative complications, which disappeared after anti-inflammatory treatment and double-J tube removal, respectively. Ten patients in the asymptomatic group developed postoperative complications: four patients developed a urinary tract infection, which improved after antibiotic therapy according to the results of urine culture and drug sensitivity testing; two patients developed hematuria, which disappeared after removal of the double-J tube; two patients experienced urine leakage, which improved after conservative treatment; and two patients had malpositioning of the double-J tube, which was reinserted after removal of the ureteroscope. In all children with urinary tract infection, the urine was positive for white blood cells, negative for protein, and positive for bacterial culture growth, and other urinary diseases were excluded by urinary computed tomography or B-ultrasound. Reoperation was required in two patients in the symptomatic group and six patients in the asymptomatic group, with no significant difference (Table 3). The postoperative review showed that the preoperative degree of hydronephrosis had become aggravated, renal PT thinning had occurred, and the renal pelvis diameter had increased.
Perioperative and postoperative outcomes.
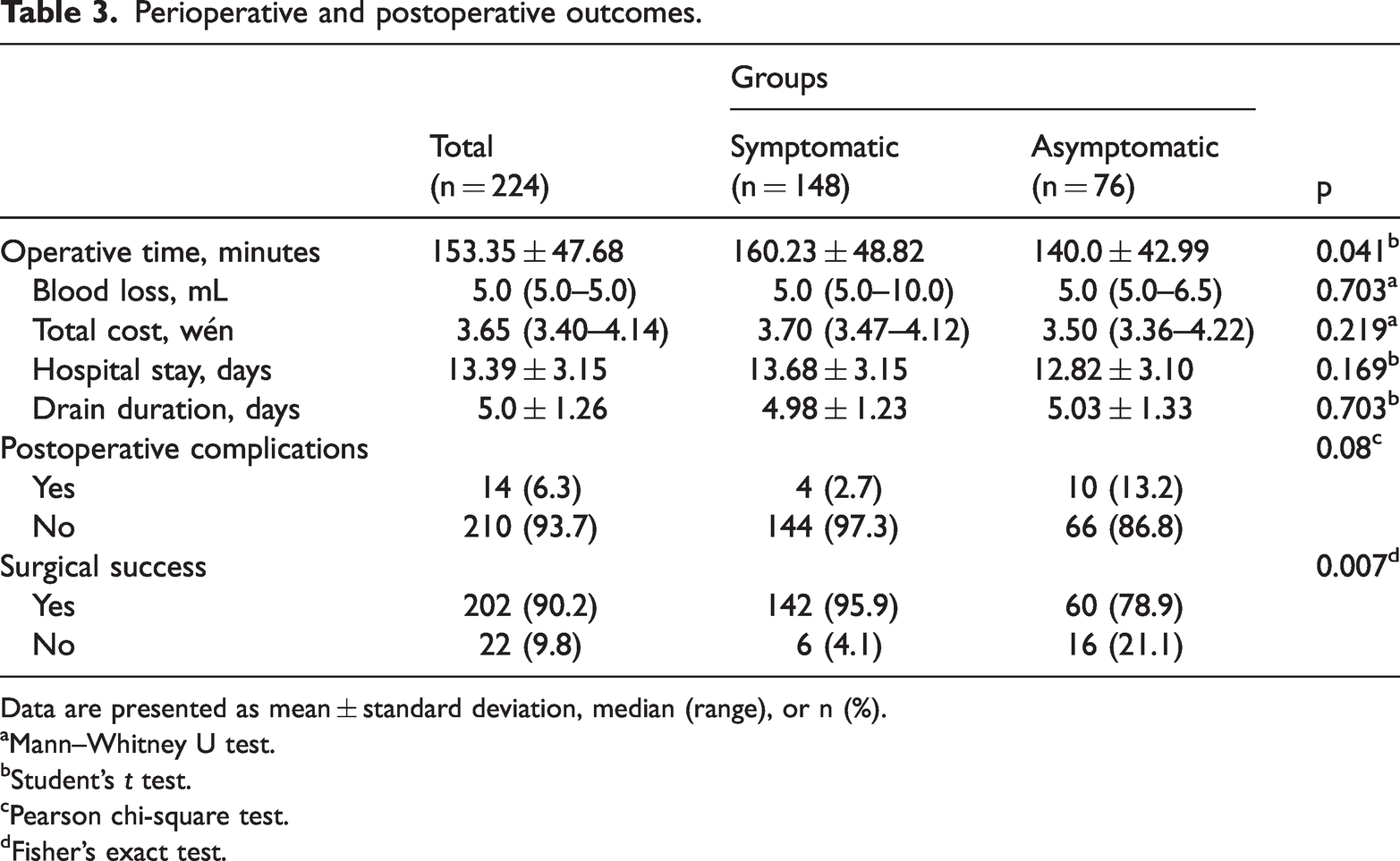
Data are presented as mean ± standard deviation, median (range), or n (%).
Mann–Whitney U test.
Student’s t test.
Pearson chi-square test.
Fisher’s exact test.
Renal parenchymal thickness of the groups.

Data are presented as median (range) or mean ± standard deviation.
Mann–Whitney U test.
Student’s t test.
Anteroposterior diameter of renal pelvis.
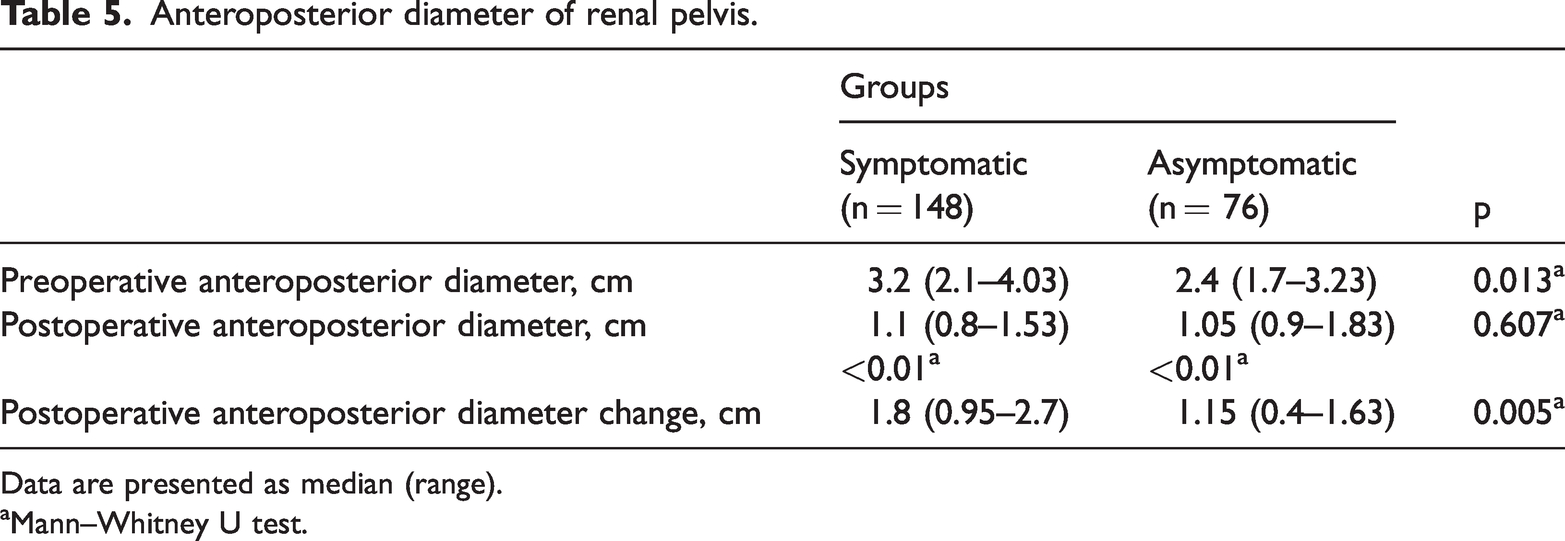
Data are presented as median (range).
Mann–Whitney U test.
To mitigate confounding bias, we constructed a multivariate logistic regression equation to account for differences in age, weight, sex, and symptoms between the two groups. The results showed that the presence or absence of symptoms had a statistically significant effect on the surgical success rate (odds ratio, 5.30; 95% confidence interval, 1.06–26.51; p = 0.042). However, age, weight, and sex had no significant effect on the surgical success rate (Table 6).
Logistic regression.
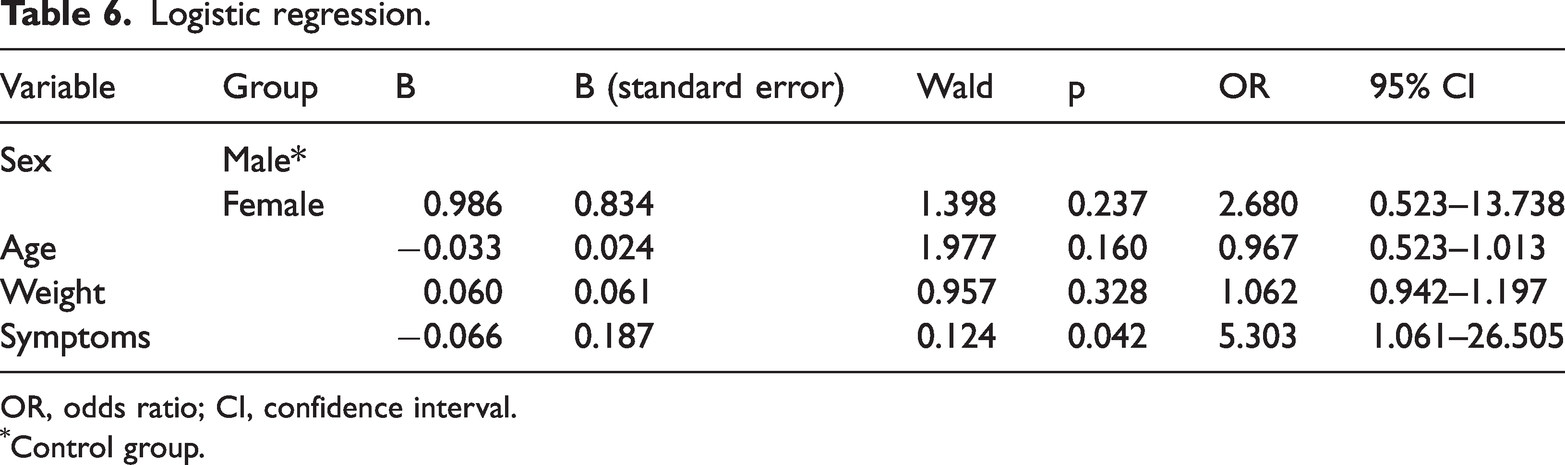
OR, odds ratio; CI, confidence interval.
Control group.
Discussion
During the last two decades, minimally invasive pyeloplasty has been widely used in the treatment of pediatric UPJO and has become an important alternative to open pyeloplasty. 14 Since the first description of LP in children, 15 LP has been widely used in the treatment of pediatric UPJO and has been proven to be a feasible and effective technique, providing good results for children and infants weighing <10 kg and aged <2 years. 16 The success rate and recurrence rate of LP are similar to those of open pyeloplasty. 17 The advantages of LP include reduced pain, a shorter hospital stay, and a better cosmetic effect on the abdominal wall. 16 The treatment decision for UPJO was historically based on clinical symptoms and auxiliary examination results. 18 However, many studies of UPJO only included children with clinical symptoms and did not consider asymptomatic children.19,20 The recent increase in the number of asymptomatic children with UPJO has caused uncertainty in clinical consultations and treatment results.
The treatment and counseling of children with UPJO are complicated because of the variety of chief complaints, wide range of surgical success rates, and uncertain imaging results. Our study aims to provide a basis for addressing these issues.
The renal PT measured by B-ultrasound is the main method for evaluating the recovery of the diseased kidney after surgical treatment of children with hydronephrosis. In children with obstruction, the PT is significantly correlated with the glomerular filtration rate of the ipsilateral kidney, which can effectively reflect the renal function. 21 The recovery of renal PT was significantly different between the two groups in the present study; the median PT in the symptomatic group (0.32 cm) was higher than that in the asymptomatic group (0.11 cm). Compared with the asymptomatic group, the symptomatic group had more significant improvement in the PT after LP, and their renal function recovery was better. Furthermore, the recovery of the anteroposterior diameter of the renal pelvis after LP was significantly better in symptomatic than asymptomatic children.
The overall success rate among all 224 children was 90.2%, which is comparable to previous series of minimally invasive pyeloplasty. The surgical success rate in the symptomatic group was 96%. The renal PT and anteroposterior diameter of the renal pelvis neither changed nor worsened in six patients during the >6-month postoperative follow-up period. In the asymptomatic group, 16 patients showed no improvement in the anteroposterior diameter of the renal parenchyma or renal pelvis at the 6-month follow-up, and the surgical success rate was 78.9%. The results of our study showed that asymptomatic children had worse surgical outcomes than those with obvious clinical symptoms. Stamm et al. 22 suggested that asymptomatic UPJO was immature before surgery and that postoperative stenosis was still progressing. This leads to further aggravation of postoperative hydronephrosis, compression of the renal parenchyma, renal ischemia and necrosis, further thinning of the renal parenchyma, and further loss of renal function. 22
The complications of LP reported in the relevant literature include urinary tract infection, stent-related complications, urine leakage, bleeding, and wound infection, among others. 23 The incidence of complications in most studies is <10%. 24 In the present study, four patients developed postoperative complications in the symptomatic group, whereas 10 patients developed postoperative complications in the asymptomatic group. Among these complications were two cases of urinary tract infection and four cases of hematuria, all of which resolved with appropriate management. The postoperative complication rate in the asymptomatic group was 13.2%, which was higher than that reported in most of the literature and significantly higher than that in the symptomatic group (p = 0.08).
The median age at surgery in the asymptomatic group was 47 months, which was significantly lower than that in the symptomatic group (90 months, p < 0.01); it was also lower than the median age of all 224 children (71 months). Moreover, 12 of 16 patients in the asymptomatic group were younger than the overall group, and the median age at surgery was 38 months (lower than the age of the overall group and the asymptomatic group). Our study suggests that asymptomatic UPJO is more likely to occur in younger children, and the cases of treatment failure in the asymptomatic group were more concentrated among the younger children in this group. Considering both our results and those reported by Stamm et al., 22 we believe that the pathophysiology and pathogenesis of UPJO in asymptomatic children may differ from that of general UPJO, and this may contribute to the differences in radiographic improvement and postoperative symptoms observed between the two groups. We believe that surgery should be performed as soon as possible in children with clinical symptoms and surgical indications. For asymptomatic children, basic research is needed to further explore the pathogenesis of the disease and thus determine the most appropriate surgical timing.
Our preliminary study findings show that in addition to the operator’s proficiency, key factors affecting the success rate and prognosis of LP include the children’s renal function or presence of hydronephrosis, intraoperative and postoperative care, and the different clinical phenotypes of UPJO. We found a significant difference in the surgical treatment effect between children with and without clinical symptoms. This indicates the need to provide more personalized, accurate diagnosis and treatment for children with UPJO.
To the best of our knowledge, this is the first study to compare the surgical treatment outcomes between symptomatic and asymptomatic UPJO in children. A novel finding of this study is that the presence of clinical symptoms may be a factor that influences the therapeutic effects.
This study has some limitations, including its retrospective, single-center design and small sample size. Additionally, the classification of clinical symptoms depends on the children’s chief complaints, which inevitably leads to retrospective bias. Large-sample prospective trials are needed for further exploration.
Conclusions
Our findings suggest that clinical symptoms may be a key factor affecting the outcome of LP. In our study, the surgical treatment effect and postoperative complications were worse in asymptomatic than symptomatic children.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241232968 - Supplemental material for Efficacy of laparoscopic pyeloplasty for pediatric hydronephrosis caused by symptomatic versus asymptomatic endogenous ureteropelvic junction obstruction: a retrospective analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605241232968 for Efficacy of laparoscopic pyeloplasty for pediatric hydronephrosis caused by symptomatic versus asymptomatic endogenous ureteropelvic junction obstruction: a retrospective analysis by Guanghui Shao, Zhihao Sun, Zhihang Zhou, Weizhen Wang and Aiwu Li in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605241232968 - Supplemental material for Efficacy of laparoscopic pyeloplasty for pediatric hydronephrosis caused by symptomatic versus asymptomatic endogenous ureteropelvic junction obstruction: a retrospective analysis
Supplemental material, sj-pdf-2-imr-10.1177_03000605241232968 for Efficacy of laparoscopic pyeloplasty for pediatric hydronephrosis caused by symptomatic versus asymptomatic endogenous ureteropelvic junction obstruction: a retrospective analysis by Guanghui Shao, Zhihao Sun, Zhihang Zhou, Weizhen Wang and Aiwu Li in Journal of International Medical Research
Footnotes
Acknowledgements
We thank JISHI Translation Studio (China) for the critical revision of the English language and grammar in this manuscript.
Author contributions
G.S.: Literature reading, data processing, manuscript writing. Z.S.: Literature quality evaluation. Z.Z.: Data collection and sorting. W.W.: Literature reading, table and chart creation. A.L.: Review and editing, supervision.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
All the authors declare that there are no conflicts of interest.
Ethics and consent
This study was approved by the Ethics Committee of Qilu Hospital of Shandong University (approval no. KYLL-202308-022). Because of the anonymized data and retrospective nature of the study, the committee waived the requirement for patient informed consent.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.