
Abstract
Objective
This study aimed to present our experience of concomitant management of renal calculi and recurrent ureteropelvic junction obstruction (UPJO) with percutaneous nephrolithotomy (PCNL) and antegrade balloon dilation.
Methods
We retrospectively reviewed 31 patients who underwent PCNL and antegrade balloon dilation for treatment of renal calculi and recurrent UPJO. The inclusion criterion was the presence of UPJO after failed pyeloplasty with ipsilateral renal calculi. Success was defined as achievement of both symptomatic and radiographic resolution of any stones and obstruction.
Results
All operations were successful without grade III or higher postoperative complications. A stone-free status was observed in all patients and the overall success rate of the procedure was 87.1% (27/31). The success rate of the procedure was significantly higher in patients with mild or moderate preoperative hydronephrosis (96%) than in those with high-grade preoperative hydronephrosis (50%). Moreover, the success rate of the procedure was lower in patients with poor preoperative renal function (0%) than in those with good or moderate renal function (93.1%).
Conclusion
Combined PCNL and antegrade balloon dilation management represents a safe and effective approach for patients with renal calculi and recurrent UPJO after failed pyeloplasty.
Keywords
Introduction
Ureteropelvic junction (UPJ) obstruction is the most common cause of antenatal and neonatal hydronephrosis, which occurs in 1/1000 to 1500 newborns. 1 The prevalence of renal calculi combined with UPJ obstruction (UPJO) has been reported to be as high as 16% to 30%. 2 Surgical management of UPJO with calculi has traditionally comprised open pyelolithotomy with pyeloplasty. This procedure has several disadvantages, such as pain caused by flank incisions and a prolonged recovery period. 3 Moreover, this procedure is associated with a risk of forming a hernia. 4 With advances in surgical techniques, minimally invasive surgeries, such as percutaneous nephrolithotomy (PCNL) with endopyelotomy (EP), laparoscopic pyeloplasty (LP), and robotic-assisted laparoscopic pyeloplasty (RALP) with concomitant pyelolithotomy, have been more widely adopted in managing these cases.5–7 However, each of these procedures has its own limitations, and there is controversy regarding whether one of these procedures is superior to the others regarding management of individual patients.
We have started combining PCNL and antegrade balloon dilation to treat patients with renal calculi and recurrent UPJO after failed open pyeloplasty or LP to ensure complete stone clearance via PCNL and to facilitate successful repair of the UPJ. This study aimed to present our initial experience with this procedure.
Methods
Patients
Between April 2010 and December 2017, 31 patients with renal calculi and recurrent UPJO after failed pyeloplasty were treated with PCNL and antegrade balloon dilation, which were performed by a single surgeon (Prof. Xiude Chen). Patients who had UPJO after failed pyeloplasty and ipsilateral renal calculi were included in this study. Patients with relatively long obstruction segments (>2 cm) or patients with calculi impacted at the UPJ were excluded from this study. The diagnosis of renal calculi and recurrent UPJO was initially made on the basis of symptomatology. This diagnosis was then confirmed via complete workups, including ultrasonography, computed tomography (CT), nuclear renal scintigraphy, and retrograde pyelography. Patients with UPJO had an obvious stricture segment at retrograde pyelography. Midstream urine tests and urine cultures were performed in all cases. All patients with urinary tract infections received sensitive antibiotics, which were chosen on the basis of preoperative urine culture results and documented negative urine culture before undergoing surgery.
Hydronephrosis was classified as grade 1 (mild), grade 2 (moderate), grade 3 (severe), and grade 4 (massive) using preoperative radiographic imaging. Renal function was assessed by nuclear renal scintigraphy and was classified as good, moderate, or poor if the affected kidney contributed >40%, 25% to 40%, or <25% of the body’s total renal function, respectively.5,8 Stones were classified according to Guy’s stone score. 9
Surgical technique
All procedures performed were in accordance with the ethical standards of the Ethics Committee of Shandong Provincial Hospital Affiliated to Shandong First Medical University. Written informed consent was obtained from all participants. In our procedure, PCNL was followed by antegrade balloon dilation under general anesthesia. The patient was placed in the lateral and jackknife position, with the affected side up (Figure 1a). An 18-gauge coaxial needle was introduced into the targeted calyx (usually a midpolar calyx) through the fornix under ultrasonographic guidance. When urine reflux was observed, a J-tip guidewire was inserted through the needle into the collecting system, and its position was confirmed via ultrasonography. A 1-cm skin incision was made at the puncture site and percutaneous access was dilated to 24F using a balloon dilation device (CR Bard, Covington, GA, USA). Nephroscopy was then performed using a 22F nephroscope. The stones were fragmented and removed using ultrasonic and pneumatic lithotripsy with a LithoClast device (EMS Electro Medical System, Nyon, Switzerland) (Figure 1b). Complete clearance of the stones was confirmed visually and ultrasonographically. A hydrophilic guidewire was then introduced in the antegrade direction and advanced to the ureter (Figure 1c), over which a balloon dilation device (Wellead, Guangzhou, China) was placed. The balloon (4 cm in length) in the nephroscopic view was <2 cm, which guaranteed that the balloon was totally across the UPJ stenosis. The balloon, which could be inflated to 18F, was inflated to 30 atm of pressure for 3 minutes. This process was monitored in real-time using a nephroscope (Figure 1d). After dilation, the balloon dilation device was removed, and an 8/9.8F rigid ureteroscope was easily advanced down to the ureter, which indicated that UPJ stenosis had been successfully dilated (Figure 1e). At the end of the surgery, two double-J ureteral stents (5F) were positioned over the guidewires to achieve better dilation and drainage (Figure 1f). A 20F nephrostomy tube was then placed. All stone fragments were collected for subsequent analysis via infrared spectrophotometry (Lanmode, Tianjin, China).

Concomitant management of renal calculi and recurrent ureteropelvic junction obstruction with percutaneous nephrolithotomy and antegrade balloon dilation. (a) The patient was placed in the lateral and jackknife position with the affected side up. (b) Percutaneous nephrolithotomy was performed via ultrasonic and pneumatic lithotripsy using a LithoClast device. (c) Stenosis of the ureteropelvic junction was observed before antegrade balloon dilation and a hydrophilic guidewire was placed. (d) Antegrade balloon dilation was performed. The dilated balloon was transparent, which enabled real-time monitoring of the procedure via nephroscopy. (e) Stenosis of the ureteropelvic junction was successfully dilated. (f) Two double-J ureteral stents were placed at the end of the surgery.
All patients underwent kidney–ureter–bladder radiography or CT (for radiolucent stones) to assess the results 2 days after the operation. Stones with a diameter of ≤4 mm were defined as clinically insignificant residual fragments. All patients were questioned regarding symptomatic improvement and underwent ultrasonography, CT, or nuclear renal scintigraphy at 1 month, 3 months, and 1 year, and then annually after stent removal during follow-up. Success was objectively defined as resolution of stones and attenuation of hydronephrosis shown by a radiographic examination, and subjectively defined as achievement of symptomatic improvement as reported by the patients. The Clavien–Dindo classification of surgical complications was applied for analysis of postoperative complications. 10
Statistical analysis
Statistical analysis was performed with SPSS for Windows, version 11.0 (SPSS Inc., Chicago, IL, USA). Fisher’s exact test was used to compare categorical variables. A P value <0.05 was considered statistically significant.
Results
Patients’ demographics and perioperative data are shown in Table 1. The mean age of the patients was 37.6 years (range: 16–49 years), and all patients were symptomatic and presented with gross hematuria or flank pain on the affected side. The mean time after the previous pyeloplasty was 12.6 months (range: 6–37 months). Eight (25.8%) patients had undergone open pyeloplasty previously and 23 (74.2%) had undergone laparoscopic pyeloplasty previously. Twenty-one (67.7%) patients had suffered from multiple renal stones on the side on which their previous procedure had been performed, and these stones were classified as Grade III according to Guy’s stone score. All operations were successful, and no intraoperative complications or open conversions occurred or were necessary. The mean operative duration, which comprised the times required for PCNL and antegrade balloon dilation, was 61.2 minutes (range: 48–117 minutes) without blood infusion. All of the patients recovered well and achieved symptomatic improvement. None of the patients experienced grade III or higher postoperative complications according to the Clavien–Dindo classification of surgical complications, such as blood loss requiring transfusion or sepsis. The nephrostomy tube was removed 2.4 days (range: 1–3 days) after surgery and the mean hospital stay was 3.6 days (range: 2–4 days). The stone-free status was recorded for all patients at the time of discharge from hospital. The ureteral stents were removed at 8.1 weeks (6–10 weeks) postoperatively according to the different tolerance of patients.
Patients’ demographics and perioperative data.
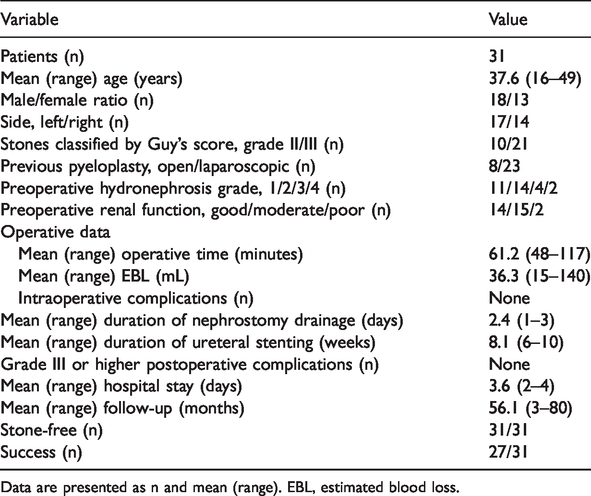
Data are presented as n and mean (range). EBL, estimated blood loss.
Thirty-one patients were enrolled in this study and underwent 56.1 months (range: 3–80 months) of follow-up. The overall success rate of the procedure was 87.1% (27/31). Failure was recorded in four patients at a mean of 3.3 months (range: 1–6 months) after stent removal as shown by radiographic obstruction. Placement of long-duration double-J ureteral stents was performed as tertiary management. Several preoperative parameters that may have affected the success rate of the procedure are shown in Table 2. There was no significant difference in the success rate between patients who had undergone previous open pyeloplasties and those who had undergone previous laparoscopic pyeloplasties. The success rate of the procedure was significantly higher in patients with mild or moderate preoperative hydronephrosis than in those with high-grade preoperative hydronephrosis (P = 0.02). Moreover, the success rate of the procedure was significantly lower in patients with poorer preoperative renal function than in those with better renal function (P = 0.01).
Success rate by preoperative parameters.

Discussion
Open pyeloplasty has been the gold standard therapy for treating UPJO for decades, with success rates as high as 90%. 11 Recent advances in laparoscopic devices and surgical techniques have led to LP being a reliable alternative for managing UPJO because this procedure has minimal invasiveness with excellent results.12–14 All primary UPJ repairs performed via open pyeloplasty or LP may fail, in which case a second operation is usually required. However, surgeons often encounter difficulty in managing recurrent UPJO via open pyeloplasty or LP because of development of fibrosis and adhesions within the region in which the previous UPJ was repaired.15–17 In retrograde intrarenal surgery, a laser is usually used to treat UPJO, which may cause postoperative scar contracture and secondary stricture. Moreover, retrograde intrarenal surgery is non-effective in managing large kidney stones. Therefore, patients and urologists are interested in development of a minimally invasive, but effective method, of treating UPJO, especially in patients with concomitant renal calculi. Antegrade endourological procedures are an appropriate option.
There have been several studies regarding the safety and efficacy of endourological procedures for treating renal calculi and UPJO. For antegrade endopyelotomy, there have been reported success rates of 64% to 85% with concomitant PCNL and 74% to 87% as a salvage method for recurrent UPJO. 18 However, no studies have reported the success rate of the combination of PCNL and antegrade balloon dilation, which is used to treat patients with renal calculi and recurrent UPJO.
We retrospectively reviewed patients’ data pertaining to all PCNL and simultaneous antegrade balloon dilation procedures that were performed at a single institution by a single surgeon over the past 6 years. All patients had recurrent UPJO after failed open or laparoscopic pyeloplasty with ipsilateral renal stones. Notably, diagnosis required confirmation via radiographic imaging studies, including ultrasonography, CT, nuclear renal scintigraphy, and retrograde pyelography. PCNL has mainly and traditionally been performed in the prone position. This position enables complete exposure of the surgical site to allow establishment of several tracts and to provide ample room for manipulating instruments. However, this position is not optimal for morbidly obese patients or patients with respiratory problems.19–21 In our PCNL procedure, all patients were placed in the lateral and jackknife position, with the affected side up, which facilitated monitoring of anesthesia and reduced the chance of injury to adjacent organs. Moreover, PCNL was performed under ultrasound guidance in our study, which enabled performance of real-time monitoring during the puncture procedure and avoided exposing patients to radiation.22,23 Antegrade balloon dilation is easy and safe to manipulate in which the degree of dilation can be well controlled by altering the balloon pressure. Moreover, this procedure can effectively reduce the possibility of postoperative scar contracture due to intraoperative heat injury that is caused by endopyelotomy with a laser or hook electrode. Two double-J ureteral stents (5F) were placed instead of one stent in our study for better dilation and drainage.
Our overall success rate of the procedure was 87.1%. This rate is comparable with the success rates of previously published studies regarding endoscopic management of secondary UPJO8,18 and higher than the success rates of previously published studies regarding endoscopic management of primary UPJO. 15 This favorable result is attributed to our critical inclusion criteria because we only included patients with secondary UPJO after failed open pyeloplasty or LP whose crossing vessels (20/31 patients, 64.5%) had been successfully displaced. Additionally, we excluded patients with stones that touched the UPJ preoperatively or those who had a stone impacted at the UPJ intraoperatively to eliminate the possibility of a pseudo-UPJO. 5 Van Cangh and colleagues 24 concluded that the presence of a crossing vessel significantly decreased long-term success rates of the procedure. This conclusion is supported by a study by Patel and coworkers who reported lower success rates for endopyelotomy for treatment of primary UPJO than secondary UPJO. 8 Therefore, patients with secondary UPJO whose crossing vessels have been displaced are better candidates for endoscopic management than those with primary UPJO whose crossing vessels have not been displaced.
Several previous studies have shown that the preoperative hydronephrosis grade and renal function are associated with the outcomes of endoscopic management for UPJO.5,8 These findings are consistent with the results of our study (Table 2) in which a higher success rate of the procedure was found in patients with mild or moderate preoperative hydronephrosis than in those with high-grade preoperative hydronephrosis. A similar trend was observed for renal function, where the success rate of the procedure was higher in patients with good and moderate renal function than in those with poor function. There was no significant relief of hydronephrosis in four patients after the operation, which was defined as failure, even though they achieved a stone-free status. In patients with severe or massive hydronephrosis, a floppy and redundant renal pelvis results in poor ureteral peristalsis, thereby limiting continuous urine flow, which may promote healing of the UPJ. A poorly functioning kidney cannot generate sufficient growth factors or mucosal regeneration modulators, which are important for successful repair of the UPJ. 25
Conclusion
PCNL combined with antegrade balloon dilation is safe and effective for patients with renal calculi and recurrent UPJO after failed open pyeloplasty or LP. This is because this procedure ensures complete clearance of stones by PCNL and facilitates successful repair of the UPJ. Although our initial data are encouraging, the relatively small number of patients included in this study and the short follow-up time of the study may have been limitations of our investigation. Additional studies are likely required to verify our findings.