
Abstract
Measuring patients’ core body temperature during surgery is essential and commonly performed with an esophageal temperature probe. The probe must be placed in the lower third of the esophagus for accurate measurement. In this case report, we describe our experience of discovering an inadvertently malpositioned esophageal temperature probe in the right inferior lobar bronchus, which led to ventilation-related problems in a patient undergoing prostate surgery.
Keywords
Introduction
Measuring patients’ core body temperature during surgery is essential to detect and prevent perioperative thermal disturbances. 1 General anesthesia and surgical procedures reduce the patient’s body temperature, and failure to prevent hypothermia can result in adverse physiological phenomena such as coagulopathy, 2 reduced wound healing, increased risk of infection, 3 and delayed postanesthetic recovery. 4 Therefore, the core temperature must be monitored in patients undergoing general anesthesia for more than 30 minutes. 1 The American Society of Anesthesiologists recommends that all patients undergoing anesthesia receive proper temperature monitoring for maintenance of proper body temperature. 5
Previous case reports have described inadvertent tracheal insertion of esophageal temperature probes during surgeries.6–10 In two of these case reports, the patients developed abnormal ventilation.6,7 In another report, the patient maintained normal ventilation but had an abnormally low body temperature measurement. 8 In two other cases, the patients maintained normal ventilation and normothermia; however, part of the temperature probe was found after lung resection, indicating that the temperature probe had been placed into a bronchus.9,10
We herein report a case involving the malpositioning of an esophageal temperature probe in the right inferior lobar bronchus. The patient’s ventilation became impaired when we applied the steep Trendelenburg position and positive end-expiratory pressure (PEEP) for robot-assisted radical prostatectomy (RARP). The problem was identified before the operation and resolved with adequate treatment. Along with this case report, we also provide a review of the relevant literature.
Case report
A man in his early 70 s (height, 157 cm; body weight, 65.9 kg) was diagnosed with prostate cancer and scheduled to undergo RARP. The patient had no underlying conditions or distinctive characteristics except for a history of appendectomy and hernia repair 40 years prior. Preoperative electrocardiography, chest radiography, echocardiography, pulmonary function tests, and blood tests showed no abnormalities.
In the operating room, the patient underwent monitoring by noninvasive blood pressure measurement, electrocardiography, and pulse oximetry. His baseline vital signs were as follows: blood pressure, 129/85 mmHg; heart rate, 61 beats/minute; oxygen saturation, 100%; respiratory rate, 15 breaths/minute; and body temperature, 36.5°C. The ambient temperature in the operating room was 22°C, and a heating circuit for heating and humidification was used as a breathing circuit. Before induction of general anesthesia, the 3M™ Bair Hugger™ Warming Blanket System (3M, Saint Paul, MN, USA) was used to warm the patient.
To induce anesthesia, 30 µg fentanyl and 130 mg propofol were administered intravenously. After confirming loss of consciousness, 50 mg rocuronium was administered intravenously, followed by 70 mg lidocaine 1.5 minutes later. After 2 minutes, the patient was intubated with a cuffed endotracheal tube with an internal diameter of 7.5 mm using a direct laryngoscope with a size 3 Macintosh blade. Direct laryngoscopy revealed a Cormack–Lehane grade 3 view, showing only the epiglottis with almost no glottis. After intubation, a size 4 oropharyngeal airway was inserted into the mouth.
General anesthesia was maintained using propofol target-controlled infusion to achieve a bispectral index of 40 to 60 with continuous infusion of remifentanil (0.1–0.5 µg/kg/minute). The fraction of inspired oxygen was set to 0.5. Nitrous oxide was not used to prevent bowel distention.
An 18-Fr esophageal temperature probe (MONITEMP®; Ace Medical, Seoul, Korea) was blindly inserted through the patient’s mouth. As the probe was inserted, the usual level of oropharyngeal resistance was felt, and the probe was inserted to a maximum of 34 cm from the upper incisors. After insertion, the body temperature was measured as 36.1°C, and there were no changes in the peak inflation pressure (PIP), tidal volume, or oxygen saturation.
For initiation of surgery, a left radial arterial line and right external jugular vein route were secured. Before assuming the Trendelenburg position, the patient’s PIP was maintained at <15 cmH2O. The patient was then placed in the steep Trendelenburg position, after which his PIP was measured as approximately 20 cmH2O. To prevent hypoxia secondary to the steep Trendelenburg position and pneumoperitoneum, PEEP of 5 cmH2O was applied. The ventilator monitor then indicated circuit leakage, and the sound of air leaking from the patient’s mouth was noted. However, the oxygen saturation was maintained at 100% with a fraction of inspired oxygen of 0.5. Leakage was only noticeable when PEEP was applied. Considering the possibility of leakage due to insufficient inflation of the endotracheal tube cuff, the cuff was deflated and the balloon reinflated. However, ventilator leakage was still detected. For more accurate assessment, the Macintosh laryngoscope with a size 3 blade that had been previously used for endotracheal intubation was now used to reassess the patient’s oral cavity. Because the exact cause of the leakage could not be identified, we addressed the issue by replacing the existing endotracheal tube. A new endotracheal tube with an internal diameter of 7.0 mm was used for reintubation after passing a leak test. The reintubation was again performed using the Macintosh laryngoscope with a size 3 blade. However, even after reintubation, circuit leakage persisted. Therefore, anteroposterior portable chest X-rays were acquired to identify the cause. The radiographs showed that the tip of the temperature probe was malpositioned in the right lower lobe (Figure 1).

Portable chest radiograph showing the esophageal temperature probe positioned in the right lower lobe.
For confirmation, a fiberoptic bronchoscope was inserted through the right main bronchus to the point at which the right middle lobar bronchus and inferior lobar bronchus diverged. Bronchoscopic examination showed that the temperature probe had entered the right inferior lobar bronchus (Figure 2). Because of concern regarding why the temperature probe was not visible during reintubation, the patient’s oral cavity was reassessed using a video laryngoscope with a size 3 blade (AceScope®; Ace Medical). This examination showed that the esophageal temperature probe had been inserted into the glottis along with the endotracheal tube after being hidden by the patient’s tongue and epiglottis (Figure 3). The temperature probe was therefore removed and reinserted into the esophagus to a maximum of 34 cm from the upper incisors under video laryngoscope guidance. After repositioning the temperature probe into the esophagus, circuit leakage was no longer observed. No other notable events occurred throughout the surgery. Pyridostigmine 15 mg and glycopyrrolate 0.4 mg were administered as the patient returned to spontaneous breathing after the surgery. After recovering consciousness, the patient was extubated and transferred to the post-anesthesia care unit.
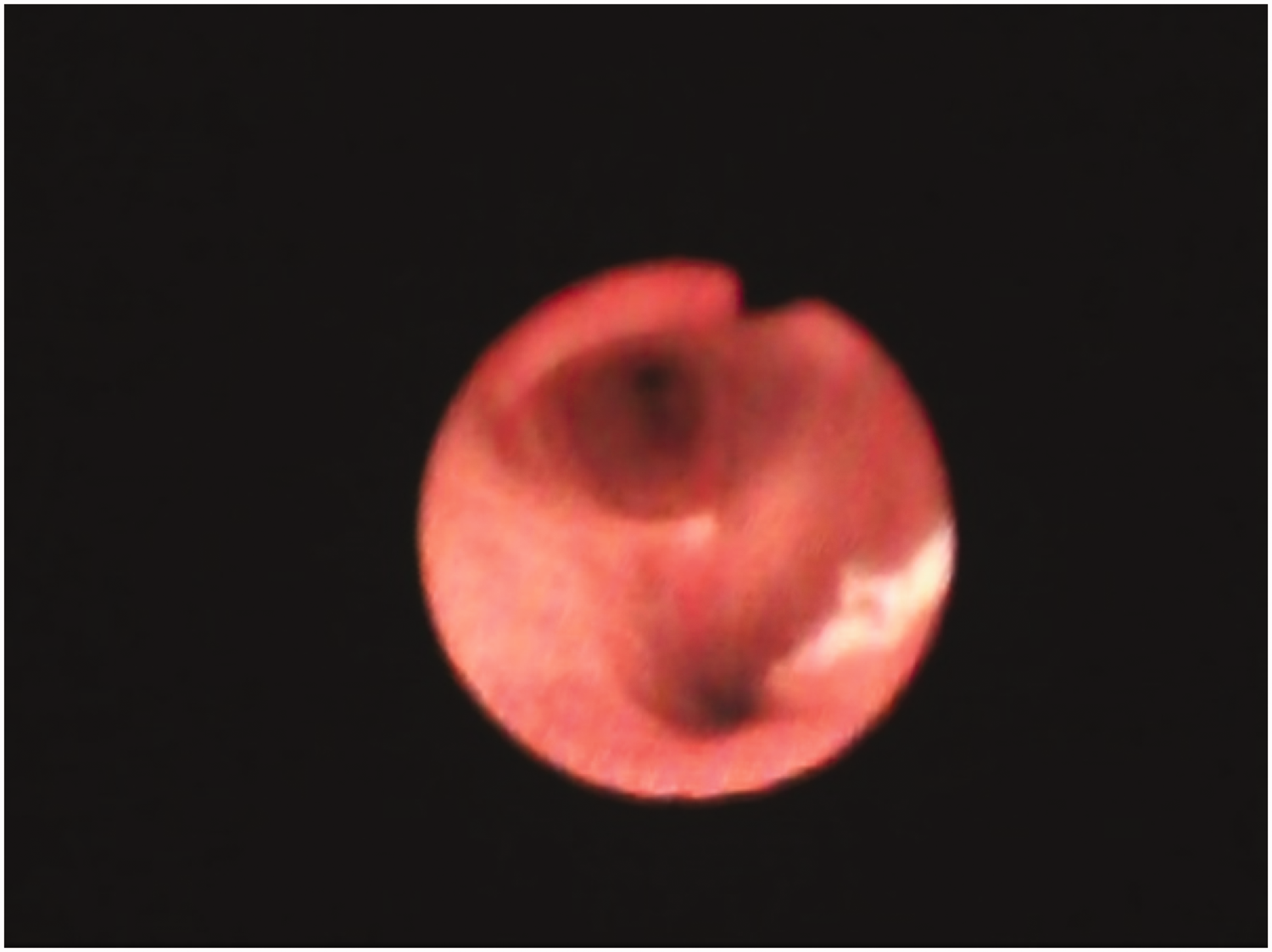
Fiberoptic bronchoscopy showing the esophageal temperature probe tip in the right inferior lobar bronchus.

Video laryngoscopy image showing insertion of the esophageal temperature probe into the glottis with the endotracheal tube.
In the post-anesthesia care unit, the patient was supported with a reservoir oxygen mask at 7 L/minute of oxygen. He was alert, and his vital signs were as follows: blood pressure, 122/91 mmHg; heart rate, 78 beats/minute; respiratory rate, 18 breaths/minute; body temperature, 36.0°C; oxygen saturation, 100%. Complications such as nausea and vomiting were not observed. The patient was monitored for 1 hour before being transferred to the general ward. He was discharged 7 days after surgery without any complications.
The reporting of this study conforms to the CARE guidelines. 11 Written informed consent was obtained from the patient’s family before publication of his anonymized data. This study was reviewed and approved by the Institutional Review Board of Daejeon Eulji University Medical Center (IRB approval no. 2023-05-008-001).
Discussion
Hypothermia, defined as a body temperature of <36°C, is one of the most common thermal disturbances encountered by anesthesiologists during surgery. General anesthetics act on the hypothalamus to inhibit the central thermoregulation mechanism that maintains the core body temperature. Other factors, such as low ambient temperature, prolonged wound exposure, and intravenous fluid injection, also contribute to unintended hypothermia. 12
Of the different temperatures that can be measured, the core temperature best represents the core compartment temperature and is therefore the most commonly measured. 13 Core temperature can be measured in areas with a sufficient blood supply from the core compartment, such as the pulmonary artery, distal esophagus, nasopharynx, and tympanic membrane. 1 In patients who have undergone endotracheal intubation, the core temperature is commonly measured using an esophageal temperature probe because of its accuracy and relative ease of operation. An esophageal temperature probe was also used to measure the core temperature in the present case. Although there may be subtle differences depending on the patients’ height, the tip of the esophageal temperature probe must be placed in the lower third of the esophagus, approximately 34 ± 3 cm from the upper incisors. 14
Previous case reports have described malpositioning of esophageal temperature probes in the bronchus. Pickard and Reid 6 reported a case involving a patient who underwent ventriculoperitoneal shunt. When the esophageal temperature probe was inserted into the trachea after intubation and PEEP was applied to improve the patient’s oxygen saturation, hypoxia worsened. Bechara De Souza Hobaika and Ricardo Botrel e Silva 7 reported a case of ventilatory disorder during myocardial revascularization surgery. Tracheal insertion of the temperature probe was recognized because the patient's PIP decreased, the measured temperature was low, and the sound of air leakage was heard after insertion of the esophageal temperature probe. Suzuki et al. 8 described a patient who underwent anterior resection of rectal cancer. Although there were no ventilation-related problems, the patient’s body temperature did not rise above 36.2°C, and tracheal insertion of the temperature probe was recognized through a routinely performed portable chest X-ray examination after surgery. Lee et al. 9 and Dabbous et al. 10 reported similar cases involving patients who underwent lobectomy. No abnormalities in ventilation or body temperature occurred during surgery, but part of the temperature probe was found in the resected lung, and tracheal insertion of the temperature probe was thus recognized.
There are several differences between our case and the above-mentioned case reports. First, in our case, airway leakage occurred after placing the patient in the steep Trendelenburg position for RARP and applying a PEEP of 5 cmH2O. RARP usually requires the lithotomy position, pneumoperitoneum, and the steep Trendelenburg position to obtain the optimal operation field. 15 However, these manipulations may cause adverse effects on the patient’s cardiopulmonary system. Pneumoperitoneum causes a cephalad shift of the abdominal viscera and diaphragm, increasing the airway pressure and decreasing the functional residual capacity, total lung volume, and pulmonary compliance. These adverse effects are further aggravated by the lithotomy and Trendelenburg positions.15,16 Changes in lung mechanics during surgery caused by the above-mentioned manipulations for RARP may increase stress on the lung, causing ventilator-induced lung injury. To prevent this, anesthesiologists apply an intraoperative lung protective strategy represented by limited tidal volume and sufficient PEEP. 15 Meininger et al. 17 studied the effect of PEEP in patients undergoing robotic prostatectomy and reported that 5 cmH2O of PEEP effectively improved arterial oxygenation in patients during pneumoperitoneum.
Second, our patient’s temperature measured with an esophageal temperature probe did not significantly deviate from the normal range. In the above-mentioned cases reported by Bechara De Souza Hobaika and Ricardo Botrel e Silva 7 and Suzuki et al., 8 the intraoperatively measured body temperature was abnormally low. In our case, sufficient warming was provided before induction of general anesthesia, and it can be assumed that the patient’s body temperature measured after intubation decreased to a lesser degree. If the esophageal temperature probe is inserted into the trachea, the inspired air temperature will be measured instead of the core temperature. The body temperature measured in this way may differ from the actual core temperature, making it difficult to prevent the above-mentioned detrimental physiological changes. Therefore, if the patient’s body temperature measured after insertion of the esophageal temperature probe is abnormally low, tracheal insertion of the temperature probe should be suspected.
When airway leakage occurred in the present case, we initially assumed that it had been caused by underinflation or rupture of the endotracheal cuff. Therefore, we deflated the cuff and reinflated the balloon. After intubation, when manual ventilation was performed several times to ensure that the PIP was >20 cmH2O, no air leakage occurred; therefore, we did not measure the cuff pressure. However, we believe that the cuff pressure should have been measured to identify the problem more clearly. Airway leakage persisted even after sufficient inflation of the cuff was achieved. This may have been caused by leakage by the physical gap due to the inability of the probe to be completely suppressed based on the low-pressure and high-volume characteristics of the endotracheal tube cuff. Reintubation was performed using an endotracheal tube with an internal diameter of 7.0 mm (one size smaller than the existing tube). Because the patient had already undergone intubation once, we considered the possibility that the airway was narrower than before because of airway soft tissue edema. Thus, we used a tube that was one size smaller to minimize soft tissue injury due to reintubation. However, we did not consider the risk that airway leakage may become more severe as a result of the smaller endotracheal tube.
If airway leakage is suddenly observed when PEEP is applied, as in our case, the possibility of tracheal insertion of the temperature probe must be considered. In many cases, however, airway leakage is not observed when PEEP is applied. Therefore, many surgeries are performed without applying PEEP and proceed without knowledge of tracheal malpositioning of the temperature probe.
Appukutty and Shroff 18 evaluated 200 patients who underwent general anesthesia. The most common sites of impaction during insertion of the nasogastric tube were the piriform sinus and arytenoid cartilage. To avoid impaction, the patient’s neck was flexed and their head was turned to one side, and the nasogastric tube was then inserted along the posterior or lateral nasogastric tube; this significantly increased the success rate of nasogastric tube insertion on the first attempt. The time required for insertion and the rates of complications such as kinking, knotting, and bleeding were also reduced. 18 These findings indicate that the same results may be achieved for esophageal temperature tube insertion. Flexing the neck and turning the head to one side may help to prevent tracheal malpositioning during insertion of temperature probes. However, such maneuvers cannot completely rule out incorrect positioning of the temperature probe.
What are the signs of tracheal insertion of the esophageal temperature probe? The clinician may notice difficulty of insertion of the temperature probe, the endotracheal tube moving together with movement of the temperature probe, more air entering than expected when inflating the endotracheal tube cuff, and a lower-than-expected body temperature measurement. A more reliable way to identify tracheal insertion of the esophageal temperature probe is to take a portable chest radiograph in the operating room. This has the advantage of being able to reliably show the location of the temperature probe; notably, however, it has the disadvantage of being inconvenient and time-consuming.
Noppens et al. 19 reported that video laryngoscopy using the superior laryngeal view was more accurate than direct laryngoscopy using a Macintosh blade. They found that this technique increased the intubation success rate and lowered the complication rate in cases of difficult intubation. 19
Therefore, when tracheal insertion of an esophageal temperature probe is suspected, video laryngoscopy can help to quickly and simply detect the position of the probe and enable easier repositioning of the probe.
Conclusion
As described in this case study, sudden airway leakage upon application of PEEP may be related to tracheal insertion of an esophageal temperature probe. Tracheal insertion of an esophageal temperature probe can lead to measurement of the inspired air temperature rather than the patient’s core temperature, resulting in differences in the measured temperature and actual core temperature with resultant complications.
Our experience in this case as well as experiences described in past case reports indicate that malpositioning of esophageal temperature probes may occur without knowledge in many patients. Although esophageal temperature probes are often used for convenient measurement of body temperature, unintentional tracheal insertion can result in complications such as inaccurate temperature measurement and hypoxemia due to abnormal ventilation. Therefore, esophageal temperature probes must be accurately inserted and placed. Prior research has indicated that this can be achieved by flexing and turning the head to one side. In addition, if airway leakage of unknown cause is observed when PEEP is applied, tracheal insertion of the probe must be suspected. Video laryngoscopy can enable rapid and convenient identification of the probe’s position, which can help to prevent complications of tracheal malpositioning. Therefore, anesthesiologists must exercise caution when inserting an esophageal temperature probe and should consider the possibility of tracheal insertion of a temperature probe if unexpected airway leakage occurs when applying PEEP. If such malpositioning is suspected, we recommend a quick visual inspection of the glottis using a video laryngoscope.
Footnotes
Acknowledgements
We would like to thank the patient and the hospital staff for their cooperation.
Data availability statement
The data are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.