
Abstract
A tracheal diverticulum (TD) is a rare disease that is usually diagnosed as an incidental finding on thoracic computed tomography or bronchoscopy. TDs can be classified as congenital or acquired. In patients undergoing surgery, TDs can result in difficult intubation, difficult ventilation, pneumothorax, and other complications. We herein report a case of anesthetic management of thoracoscopic pulmonary wedge resection in a patient with a giant TD in the carina. Intraoperative double-lumen intubation and single-lung ventilation were challenging to perform. Fiberoptic-guided intubation was helpful, and intraoperative management was tailored to avoid diverticulum rupture. In this report, we also review complications related to TD in surgical patients undergoing mechanical ventilation. Ventilation is one of the most prominent anesthetic challenges. The close collaboration of the entire medical team was a key factor in the successful management of this rare case.
Keywords
Introduction
A tracheal diverticulum (TD) is an outflow from the wall of the trachea and a type of paratracheal air cyst. TDs vary in size and area and are uncommon in the clinical setting. They are usually located at the level of the sternum (T1–T3), and some are only the size of a needle tip.1,2 The prevalence of TDs in patients with cystic fibrosis is reportedly around 28%, with sizes ranging from 2 to 32 mm. 3 The currently reported incidence of TD ranges from 0.75% to 8.10%.4,5
Surgical patients with TDs present major challenges for anesthesiologists. A detailed preoperative examination is crucial. The exact location and size of the TD and the effect of intraoperative mechanical ventilation or laparoscopic gas on the TD should be properly evaluated. However, few studies of TD have been performed, and experience in the perioperative anesthetic management of these patients is lacking. We herein describe the anesthetic management of a patient undergoing thoracoscopic pulmonary wedge resection with a large TD at the tracheal carina and review the complications of mechanical ventilation in these patients. The reporting of this study conforms to the CARE guidelines. 6
Case report
A 48-year-old woman (body mass index, 25 kg/m2) presented with a >1-year history of a right pulmonary nodule. The nodule had been found during a physical examination. The patient also had multiple cysts in the liver. She showed no clinical discomfort. No abnormalities were found on physical examination or laboratory tests. Preoperative thoracic computed tomography (CT) revealed a ground glass focus (1.4 × 1.0 cm) in the lower lobe of the right lung, small nodules in the middle lobe of the right lung with a maximum diameter of 0.5 cm, and a large cystic gas density (2.4 × 2.0 cm) in the posterior lower part of the tracheal carina, which was suspected to be a TD (Figures 1, 2). Intraoperative pathology was required to clarify the characteristics of the right pulmonary nodule. All procedures were carried out in compliance with the established standards. The patient was prepared to undergo wedge resection of the right lower lobe by video-assisted thoracoscopic surgery under general anesthesia with bronchial intubation. She fasted overnight. After entering the operating room, oxygen was administered by mask (2–4 L/minutes), and routine monitoring was performed by electrocardiography and measurement of her oxygen saturation. A left radial artery catheter was placed under local anesthesia to measure her arterial blood pressure, and a urinary catheter was placed. A defibrillator was prepared in advance. Anesthetic induction was performed using midazolam (1.5 mg), sufentanil (20 µg), propofol (100 mg), and rocuronium bromide (50 mg).

Axial contrast-enhanced multidetector computed tomography of the chest. (a) Imaging showed a tracheal diverticulum (black arrow) that was located at the right posterior carina and connected to the right principal bronchus. (b) The tracheal diverticulum was largest in the lung window.
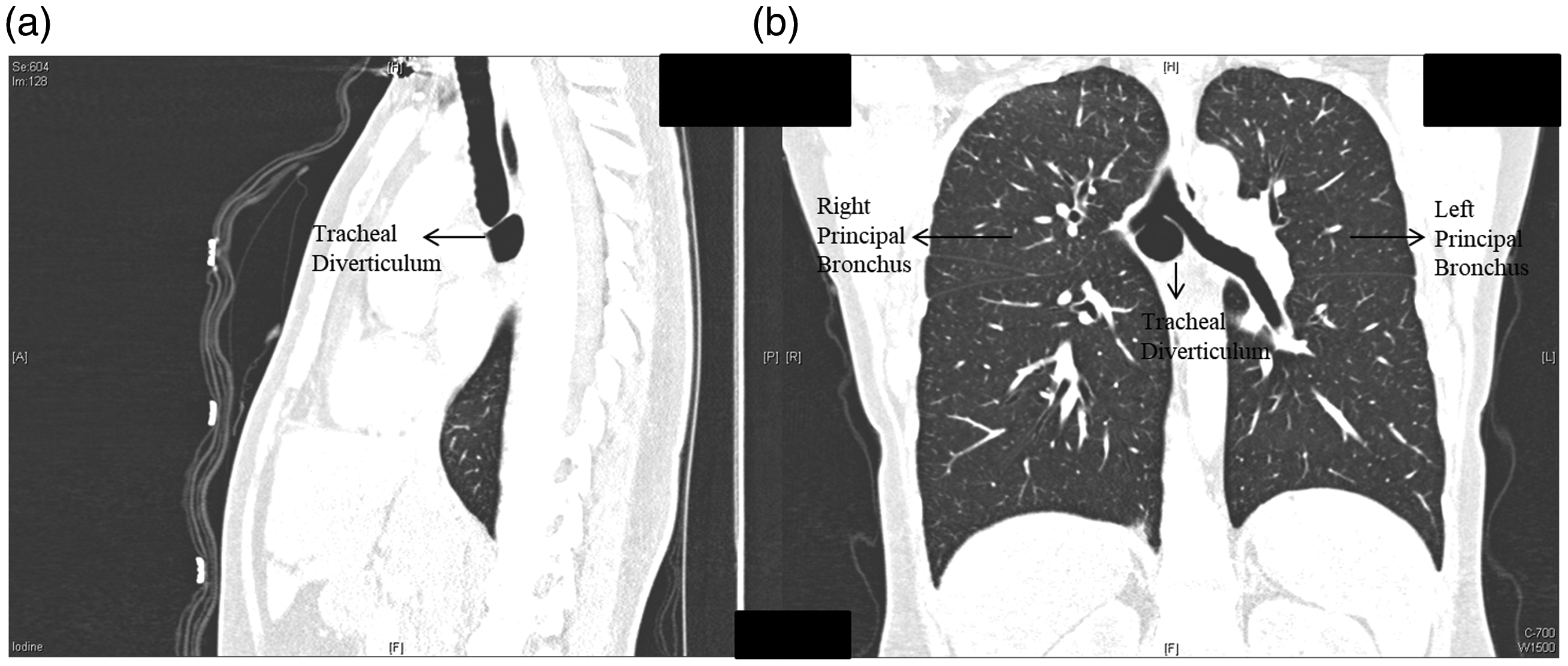
(a) Sagittal and (b) coronal images of the large tracheal diverticulum.
After 5 minutes of hand-controlled ventilation, biluminal bronchial intubation was performed using a left-sided endobronchial tube under the guidance of a fiberoptic bronchoscope. A large diverticulum was seen in the tracheal carina, which was larger than the left and right principal bronchus openings (Figure 3). The tracheal carina formed a triple-opening structure. The left-sided endobronchial tube was gently inserted into the left bronchus to a depth of about 28 cm. Mechanical ventilation was achieved with the ventilator. Intraoperative anesthesia was maintained with propofol and remifentanil. The patient’s electrocardiogram, oxygen saturation, invasive blood pressure, arterial blood gas, urine output, end-tidal carbon dioxide, and body temperature were monitored intraoperatively. In addition, the bispectral index (BIS) of the depth of anesthesia was recorded using a BIS monitoring system. The depth of anesthesia was maintained at a BIS of 40 to 60. Preoperative examination by fibrilloscopy had revealed a deep diverticulum with a weak wall, convex to the interior of the thoracic cavity. After surgery, the thoracoscopic image showed that the TD protruded into the inner trachea.

The bronchoscopic view showed the tracheal diverticulum (black arrow) on the middle aspect of the tracheal carina.
The whole operation procedure was smoothly performed. The surgery took 1.5 hours, with a bleeding volume of 20 mL, urine volume of 200 mL, crystallite infusion of 500 mL, and colloid infusion of 500 mL. Intraoperative pathology indicated either carcinoma in situ or adenoma, and mediastinal lymph node sampling was further performed. After 30 minutes of observation in the recovery room, the patient returned to the ward. Flurbiprofen and sufentanil were used for postoperative analgesia. During postoperative follow-up, the patient’s visual analog scale score was 1, and she developed no nausea, vomiting, fever, or any other complications. The patient was discharged from the hospital 4 days postoperatively. Further treatment, such as targeted therapy, radiation therapy, or chemotherapy, will be based on the final pathology.
Discussion
This is the first reported case in which single-lung ventilation was required in a patient with a large diverticulum at the tracheal carina. The site of the TD undoubtedly presents a challenge for bronchial intubation. With the particular location of the TD in this case, adequate preoperative preparation and intraoperative management to avoid breakage of the TD were crucial. Several considerations were important in the present case.
First, fiberoptic-guided intubation was performed because blind intubation may have resulted in accidental insertion of the tube into the TD. Second, because of the weak wall of the TD, accidental puncture by the double-lumen tube may have resulted in the tube entering the aorta or pulmonary artery, causing rupture and bleeding. This was also the most dangerous and noteworthy aspect of this case. Third, after double-lung ventilation, positive end-expiratory pressure was added to avoid rupture of the thin wall of the TD, development of a tracheal fistula, or reverse protrusion of the TD into the trachea, blocking the bronchial opening. Finally, after closing the pleural cavity, the residual gas in the pleural cavity resulted in positive pressure, and the thin wall of the TD protruded into the trachea and pulsated with the heartbeat. Therefore, suction and extubation were very gently performed to avoid damaging the thin wall of the TD. However, the effects of intraoperative single-lung ventilation, double-lung ventilation, heart rate fluctuations, lung inflation, and thoracoscopic pressure on the TD have not been fully studied.
TD, also known as a paratracheal air cyst, is a rare benign disease. It is commonly diagnosed as an incidental finding on thoracic CT or bronchoscopy. They can be classified as congenital (a cystic structure connected to the trachea through a narrow isthmus resulting from normal tissue growth and degeneration) or acquired (a weak spot with increased pressure on the tracheal wall resulting from mucosal protrusion and development). 7 Most patients with TDs are asymptomatic, and the TD is diagnosed incidentally by radiographic examination of the chest. A small percentage of patients present with cough, recurrent respiratory infections, hoarseness, or dyspnea.4,8,9 A TD is an uncommon anatomical abnormality that can cause serious complications during general anesthesia and tracheal intubation, such as difficulty intubating or ventilating. 10
We searched the literature for incidental findings of TDs in mechanically ventilated patients with associated adverse outcomes. All were case reports, and the clinical information of these reports is summarized in Table 1.11–17 In all cases, the TD was diagnosed by fiberoptic bronchoscopy or CT. Möller et al. 16 reported a case of postoperative mediastinal emphysema due to accidental perforation of a dilated trachea as a result of tracheal intubation. Mazul-Sunko et al. 15 experienced a case of mediastinal emphysema associated with a TD; however, the authors concluded that mediastinal emphysema was not likely associated with injury to the TD caused by the tracheal tube. Chakraborty et al. 12 reported a rare case of a ruptured TD by intubation leading to pneumothorax, pneumopericardium, pneumomediastinum, pneumoperitoneum, and pneumoretroperitoneum. The remaining cases of TD were associated with difficult intubation, ventilation, or lung isolation. Although TD is infrequent in clinical practice, its adverse consequences cannot be ignored.
Characteristics of the included studies.

NA, not available; ETT, endotracheal tube; DLT, double-lumen tube.
In previous studies, most of the patients with TDs were diagnosed incidentally; they had no clinical symptoms and lacked appropriate preoperative imaging examinations. This is undoubtedly a critical and urgent situation that can result in failed tracheal intubation, tracheal leakage, and other complications. Repeated respiratory infections, insufficient intubation, and ventilation without an identifiable cause require vigilance for TD. Reintubating the patient with a larger-diameter endotracheal tube and ensuring that the catheter covers the TD opening by fibrilloscopic examination is an alternative approach when difficult ventilation is associated with a TD. A case of an iatrogenic TD has also been reported and might have occurred by increased cuff pressure from improper endotracheal tube placement. 18 Preoperative CT scans are necessary to avoid accidental injury. Timely and accurate diagnosis of the TD is crucial, especially for patients requiring general anesthesia with tracheal intubation. Resection of the TD is an effective method for symptomatic patients. 19
There is a lack of clinical research in this field because TDs are uncommon and vary in shape, size, and location. The available literature is mainly based on case reports. Therefore, experience with perioperative management and anesthesia in these patients is limited. Close attention to the results of CT and fibrilloscopy is required. Timely diagnosis of TD is important to prevent perioperative adverse events. This case may increase the understanding of TD in future clinical work.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211032855 - Supplemental material for Anesthetic management of thoracoscopic pulmonary wedge resection with a giant tracheal diverticulum in the carina: a case report and review of the literature
Supplemental material, sj-pdf-1-imr-10.1177_03000605211032855 for Anesthetic management of thoracoscopic pulmonary wedge resection with a giant tracheal diverticulum in the carina: a case report and review of the literature by Xiao Huang, Yuan Sun, Dandan Lin, Changewi Wei, Anshi Wu and Chao Gao in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics
The requirement for ethics approval was waived because this was a case report and not a clinical trial. Written informed consent was obtained from the patient. We have de-identified the details such that the identity of the patient may not be ascertained in any way.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.