
Abstract
Treatment of multiple benign breast nodules is sometimes challenging with respect to establishing a surgical plan that achieves both therapeutic and cosmetic goals. Successful application of oncoplastic techniques has been reported in selected cases of benign breast lesions. In this case report, we present the surgical treatment and outcome of a patient with multiple fibroadenomas in ptotic and voluminous breasts. A combined procedure of extensive glandular resection and reduction mammoplasty using a modified vertical pedicle technique was performed on this patient, who desired complete lesion removal, volume reduction, and mastopexy. The cosmetic result was satisfactory at both the short- and mid-term follow-up. In addition, different techniques applied in the treatment of breast fibroadenoma are herein reviewed and discussed.
Keywords
Introduction
Fibroadenoma is a commonly encountered benign breast nodule in breast surgery departments.1,2 Simple lumpectomy is the first-choice treatment for isolated nodules with satisfactory outcomes. Among previous reports, more complicated cases have involved a single lesion of either large size or pathological rarity. However, in patients with multiple small- to medium-sized unilateral or bilateral nodules, the clinical outcome and patient satisfaction are impeded by the need for multiple incisions and repeated surgeries to treat diffusely located nodules or recurrent diseases. 3
Reduction mammoplasty and mastopexy are classical surgical techniques usually applied in patients with macromastia and/or mastoptosis. 4 These plastic surgery techniques have been gradually accepted by breast surgeons and applied in selected patients with breast cancer, resulting in acceptable oncological and cosmetic outcomes. However, few clinical reports have described combined volume reduction and mastopexy for multiple benign breast nodules.5–7
We herein report a case of bilateral multiple breast fibroadenomas treated by gland resection with volume reduction and simultaneous mammoplasty. A satisfactory clinical outcome was obtained. The reporting of this study conforms to the CARE guidelines. 8
Case presentation
A woman in her late 40s with a body mass index of >25 kg/m2 and bra cup size of 36E presented with multiple palpable, sharply demarcated nodules diffusely located in all quadrants of both breasts, including the sub-areolar region. There was no evidence of overlying skin or nipple areola complex (NAC) involvement, such as the peau d’orange sign or nipple asymmetry, retraction, or hemorrhage. Preoperative breast evaluation revealed pendulous breasts with grade 2 ptosis and a bilateral base width of 15 cm. The patient had no relevant diseases, was taking no medication, and had no family history or medical history. Preoperative ultrasonography (US) and mammography (MMG) showed bilateral multiple nodules of BI-RADs category 3 or 4a ranging from 0.6 to 3.5 cm in diameter (Figures 1 and 2). Fine needle aspiration cytology performed on suspected category 4 lesions showed no signs of malignancy. Routine laboratory testing showed that the levels of sex hormones were within the reference ranges. The patient and her husband desired removal of all breast lesions with adjustment of the shape and volume of the bilateral mammary glands. After discussion with the patient and her husband, they provided informed consent for treatment comprising bilateral gland resection with volume reduction and simultaneous mammoplasty.

Ultrasonography images showed similar hypoechoic lesions with sharp demarcation and partial calcification.

Mammography images showed diffuse high-density lesions with sharp demarcation in the bilateral breasts.
Surgical procedure
Preoperative skin markings were made with the patient in a standing position. These markings included a newly positioned areola and a lower pedicle measuring approximately 4 cm in width, with arms extending both medially and laterally from the bottom. The midline, inframammary fold, and axial line passing through the volumetric center of each breast were also marked (Figure 3). After induction of general anesthesia, the patient was placed in the supine position with both arms prepared and draped. A circumareolar incision was made extending down to the dermis, and another parallel circular incision was made 15 mm from the original areola. Another incision was made along the lower pedicle and inframammary fold. The inferior pedicle, which was approximately 4 cm in width, was de-epithelialized and prepared bilaterally. Extensive gland resection started at the inframammary incision, extended medially and laterally from the lower pedicle, and proceeded upward. A complete thick layer of adipose tissue and a thin layer of normal underlying breast tissue were preserved. For nodules located under the areola, the dissection level was adjusted accordingly to maximally protect the blood supply of the NAC. All detectable nodules were removed en bloc with few surrounding glands. More glandular tissue was removed from the breast with fewer nodules to balance the final volumes of both sides. After removal of sufficient glandular tissue, the wound cavity was irrigated with normal saline and a drainage tube was placed on both sides. The upper pedicle was folded to lift the NAC. After relocating the NAC to its new position, the lateral flaps were placed to cover the inferior pedicle. Simultaneously, the adipodermal glandular bridge of the inferior pedicle was folded and attached to the pectoral fascia to achieve a hemispherical appearance of the lower part of the breast. Closure was performed in an inverted T pattern without difficulty. The final resected volume (including nodules) was 380 mL on each side (Figure 4).

Preoperative photograph showed pendulous breasts with a low level of the bilateral nipples and preoperative mapping with the new areolar positions marked.

Operative incision diagram. The thick lines represent the incisions during our operation. The oblique line areas were de-epithelialized, while the area below the nipple–areolar complex (cross-lined area) was de-epithelialized and then folded and attached over the pectoral fascia.
Gross findings
Sixteen nodules were identified in the left breast, ranging in size from 0.5 × 0.5 ×0.5 cm to 3.5 × 3.0 × 2.8 cm. Eight nodules were identified in the right breast, ranging in size from 0.5 × 0.3 × 0.3 cm to 3.2 ×3.0 × 2.5 cm. These nodules were round or elliptical with intact fibrous capsules, and the cut sections of the nodules were grayish-white with a partly gelatinous and partly calcified texture (Figure 5).

Display of all of excised fibroadenomas by size in the bilateral mammary glands.
Pathological diagnosis
The histomorphological features of all of the lesions in the bilateral mammary glands were diagnostic for fibroadenoma combined with adenosis, exhibiting glass-like degeneration and calcification as well as usual ductal hyperplasia (Figure 6).

Representative histologic sections from the fibroadenomas (hematoxylin and eosin, ×100).
Clinical outcome
The patient’s recovery was uneventful. The sutures were removed on postoperative day 10. Clinical photographs were taken during routine clinical follow-up visits. The vascularity and sensation of the NACs as well as the appearance and symmetry of the breasts were satisfactory. The cosmetic outcome was also evaluated by two breast surgeons, who judged the result as good at 3 months postoperatively according to the Harvard scale 9 (Figure 7).
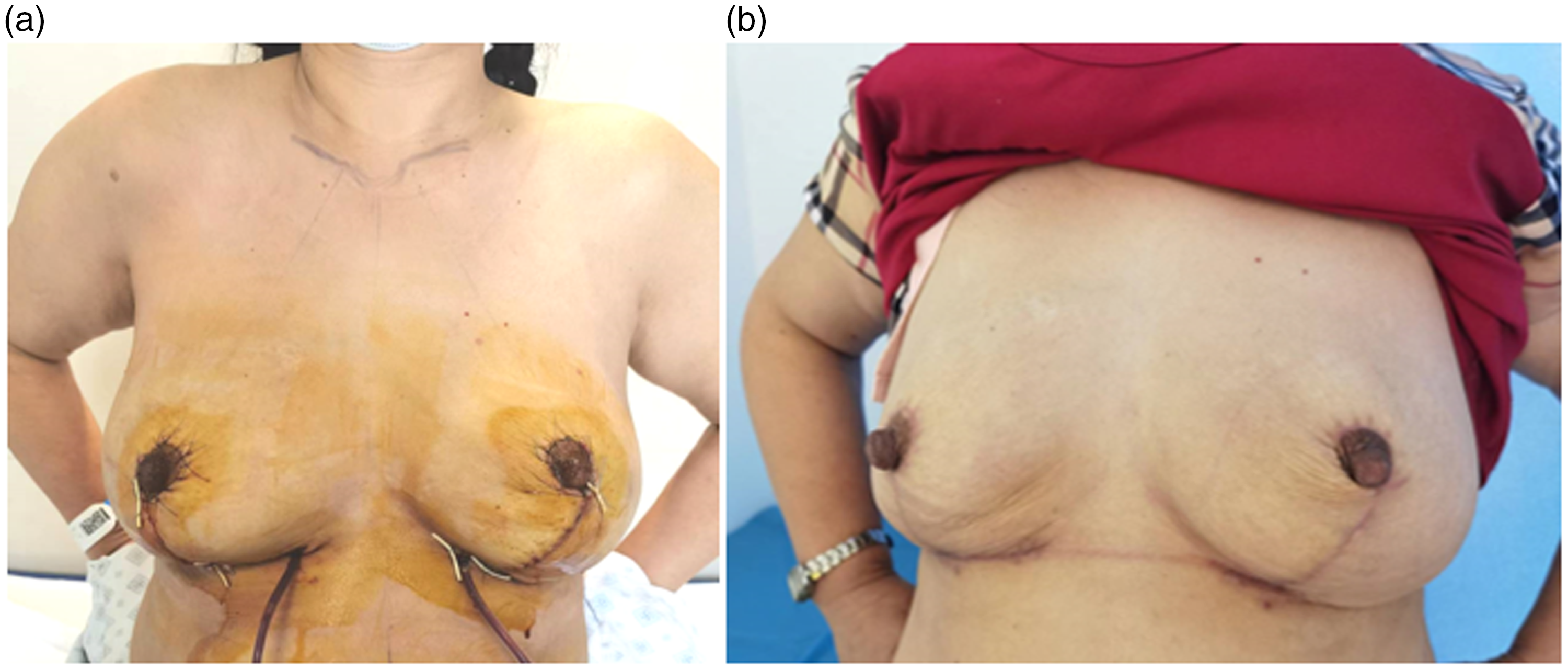
(a) Postoperative view at the 7-day follow-up and (b) Postoperative view at the 3-month follow-up with well-maintained contour of the bilateral breasts.
Discussion
Fibroadenoma is a common fibroepithelial lesion arising from the terminal duct lobular unit and adjacent tissue of the breast. For a single fibroadenoma of moderate size, simple lumpectomy is an adequate treatment.1,2 More complicated cases have also been reported, including resection of an exceptionally large lesion with or without special plastic surgery techniques.3,5–7
Benign breast lesions are common, but they do not cause high concern among surgeons. Reports to date have mainly focused on benign lesions of either exceptionable size or uncommon pathological types.5,6 For single or a few scattered small to medium nodules, conventional lumpectomy with an incision designed according to the nodule location and size is preferred. For multiple nodules, the conventional surgery strategy is creation of more incisions to remove large nodules. However, increased reoperation rates have been seen in patients with multiple nodules, such as patients with adenosis or fibroadenomas. Repeating an operation not only increases medical costs but also impacts the cosmetic outcome and patient’s mental state. 2
Breast reduction and mastopexy are traditional plastic surgeries that are sometimes applied in combination with mastectomy and breast reconstruction for breast cancer. For unilateral tumors in an oversized and ptotic breast, tumor treatment, achievement of bilateral symmetry, and contour correction can be achieved simultaneously.10,11 By using skin flaps and adjustment of remnant gland tissue, the impact of tissue volume resection on the breast shape can be minimized in select cases.12–15 Normally, the breast volume or the resected-to-total breast volume ratio should be within a certain range. In addition, combining plastic surgery procedures in the treatment of breast cancer reportedly has no negative impact on tumor-related survival.15,16 In some patients, integration of these plastic surgery techniques into an onco-surgical procedure is being embraced by increasingly more breast surgeons in China because it meets the demands of both tumor resection and cosmetics.
Because of the nature of localized benign breast lesions, surgical procedures are similar, typically involving complete resection or lumpectomy. Indications for surgery are consistent and include a large size (>2 cm in most cases), growth pattern suggestive of malignancy, characteristic imaging findings (US, MMG, or MRI), and inconclusive results from cytology or core needle biopsy.
Previous reports of plastic surgery techniques for treatment of breast diseases mainly involve a malignancy or single large nodule.10–16 We have herein reported the application of plastic surgery in a special case. This case had several aspects that were advantageous for surgical planning. First, the patient had benign disease, eliminating concerns about resection margins. Second, diffusely located lesions often raise cosmetic concerns because multiple incisions are often used to remove the nodules with surgical indications, but not all the nodules. Our technique alleviated this concern. Third, the voluminous and ptotic breast allowed for extensive gland resection, facilitating removal of all lesions and reducing the risk of recurrence. Fourth, the patient was 48 years old and had no further expectations to breastfeed, thus eliminating the concern regarding how breastfeeding might be impacted by the breast reduction surgery. The patient requested removal of all lesions within one procedure and wished to maintain the shape and symmetry of the breasts. Cases involving the combination of all the above-mentioned features are quite uncommon. At the time of this writing, our patient was continuing to undergo routine follow-up, including monitoring for recurrence and any changes in the shape of the breasts.
Few reports have described the use of plastic surgery to treat bilateral multiple fibroadenomas. Such surgical techniques include circumareolar incision–subdermal tunneling dissection with the so-called “round block” technique or the inferior glandular dermo-lipo flap technique, mainly applied in Germany.17–20 In this case, we applied a modified lower pedicle technique. Instead of maintaining the NAC blood supply by a single vertical flap alone, we preserved the blood supply from both the superior and inferior directions through a bipedicle structure. This was achieved by dissection of the glands from the medial and lateral sides of the pedicle. In this way, all the lesions including those located underneath the lower pedicle were removed completely, leaving a vertical dermoglandular tissue bridge that reliably ensured the vascularity of the NAC. Moreover, the relatively slack lower part of the pedicle that was present after lifting the NAC could be folded and fixed to the chest wall to create a satisfactory hemisphere shape of the breast. Finally, the bipedicle maneuver was beneficial in terms of preserving NAC sensation and nutrition through the subdermal plexus. Follow-up evaluation confirmed NAC viability and sensation as well as satisfactory breast symmetry and shape.
In patients with multiple complex benign nodules, achieving both therapeutic and cosmetic goals is sometimes difficult. The major challenges are the significant size, numerous lesions, and associated risk of recurrence. In general, complete resection of lesions with a capsule or a thin layer of adjacent glandular tissue is acceptable for benign lesions, such as a fibroadenoma or fibroadenomatous hyperplasia. The margin requirement in benign lesions is less demanding than that in breast-conserving surgery for breast cancer. In large medical institutes, surgeries for benign lesions are usually performed by residents or less experienced young doctors. Therefore, the motivation to improve operative techniques in surgery for benign lesions is not as strong as in oncologic surgery.
At present, technical innovations and research on benign breast lesions are mainly being performed in the field of minimal invasive surgery. In the vacuum-assisted resection or Mammotome (MMT) procedure, the nodule is removed in pieces under the guidance of US, MMG, or MRI. The resection is performed through a 5-mm skin incision, causing debating about whether the MMT procedure is indeed minimally invasive or is instead a minimal-incision procedure. A clear advantage of the MMT is that it enables accurate and complete resection of deeply located nodules. However, the procedure also has notable disadvantages. 21 First, the size of the mass than can be resected is limited by the instrument, which generally does not exceed 2.0 to 2.5 cm in diameter. Second, in patients with multiple nodules (e.g., more than five), the risks of device fatigue and failure to achieve complete resection increase. Third, use of the MMT is not suitable for benign to borderline tumors, such as phyllodes tumors, which have an increased risk of recurrence. Therefore, the MMT procedure is mainly suitable for a limited number of small breast nodules of specific size, particularly in cases where a benign diagnosis is presumed, there is diagnostic uncertainty, or recurrence has developed after a previous biopsy. Importantly, the decision to excise a fibroadenoma is often individualized and should be made in consultation with a healthcare provider who can consider the specific characteristics of the tumor and the patient’s medical history and preferences. The diagnostic application of the MMT in biopsy of suspicious malignancies with difficult localization or in the neoadjuvant therapy setting is not discussed in this article.
Laparoscopy or a laparoscopy-assisted technique removes breast nodules via an areolar or axillary approach. 22 This technique is commonly applied for benign lesion such as gynecomastia. 23 For multiple, scattered, or deeply located masses, intraoperative image-guided resection is feasible. However, most patients and surgeons are still accustomed to local incisional resection over the surface of the mass unless the procedure is being performed for research purposes.
Another objective is to minimize the alteration of the breast contour after resection of a considerable volume of tissue compared with the original breast size. Oncoplastic techniques and skin flap techniques are applied for medium to large nodules. Appropriate adjustment of glands and skin flaps or the use of autologous or prosthetic reconstruction has been reported to satisfactorily maintain the symmetry of the breast.15,16
In addition to the primary goal of lesion removal, addressing concerns related to the risk of recurrence (largely influenced by the pathological characteristics of the nodule) and minimizing the impact on the appearance of the breast (often contingent on the size and location of the mass) are also important concerns among patients. To meet these challenging requirements, breast surgeons must not only master basic general surgical techniques and principles but also have a refined aesthetic sensibility. Knowledge of relevant basic plastic surgery concepts and technologies is essential, along with the ability to attentively address patients’ concerns. The surgeons’ goal must be to achieve an optimal balance between effective treatment and aesthetic outcomes in all aspects of care.
The uniqueness of our case lies in its distinctive clinicopathological and anatomical conditions. The outcome was characterized by the complete preservation and even improvement of the original breast appearance through the application of breast reduction and mastoplastic techniques. By learning and applying relatively simple plastic surgery techniques such as breast reduction or augmentation, breast surgeons can achieve both effective tumor resection and aesthetic outcomes. Publication of similar data is expected in the future, which will help to deepen the understanding and evaluation of plastic surgery in the treatment of complex breast lesions. More data on the application of plastic surgery techniques in special cases of benign breast lesions will help to achieve optimal therapeutic and cosmetic outcomes.
The main limitation of the surgical technique described in our case is that it is unsuitable for young women with plans to breastfeed.
Footnotes
Author contributions
L.Z. and Q.Y. contributed to the conception of the report. All authors participated in all aspects of the patient’s treatment. L.Z. wrote the first draft of the manuscript, and L.Y. reviewed the manuscript for clarity and English use. L.Z. and Q.Y. were the guarantors of the entire manuscript. All authors read and approved the final manuscript.
Data availability statement
Any further inquiries about the data of the report beyond the information provided in the article can be directed to the corresponding author.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
This case report was authorized for publication by the ethics committee of Tongji Hospital of Tongji Medical College of Huazhong University of Science and Technology (ethics approval number: TJ-IRB20230237). Written consent to publish the case report was obtained from the patient, and we have de-identified the details of the patient to the greatest extent possible.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.