
Abstract
In patients with breast cancer, oncoplastic breast-conserving surgery can achieve a good aesthetic outcome without compromising oncological outcomes. However, tumors located in the upper inner quadrant (UIQ) are challenging for surgeons because treatment gives rise to visible scars, glandular deformities, and deviation of the nipple–areolar complex. The present study was performed to analyze a modification of the matrix rotation technique for UIQ tumors and address the main drawback of this technique, which is a visible scar on the commonly exposed part of the breast. A prospective database of seven patients who presented with UIQ tumors and underwent the new modification technique was utilized for the analysis. All patients preferred the modified technique over the standard technique because of the absence of a scar in the UIQ (visible breast line). The postoperative patient-reported outcomes regarding breast shape, breast symmetry, and scar location were also satisfactory. No surgical complications were reported. This modified surgical technique results in a scarless UIQ and is an aesthetically acceptable procedure that can be considered for UIQ tumors.
Keywords
Background
Breast cancer is the most common malignancy among women worldwide. 1 Oncoplastic breast-conserving surgery (O-BCS) has become the standard of care for surgical treatment of breast cancer because it provides a good aesthetic outcome while maintaining an equivalent oncological outcome to other techniques. The term “oncoplastic” was introduced in the literature in 1997 to expand the spectrum of the indications for BCS and improve the aesthetic outcomes following surgery. 2 This led to a higher quality of life by reducing the detrimental impacts of psychosocial maladjustment, poor body image, and sexual dysfunction caused by mastectomy. 3 However, tumors located in the upper inner quadrant (UIQ) still pose a challenge to surgeons, especially those located far from the nipple–areolar complex (NAC). Wide resection in the UIQ generally gives rise to scars along the visible breast line, glandular deformities due to insufficient tissue for reshaping, and deviation of the NAC. 4
Several surgical techniques have been described in the literature to address UIQ tumors. Each technique has its own advantages and disadvantages, and no single technique is considered the ideal. As a result, there is a need for innovative approaches that can overcome the drawbacks of existing techniques.
On this background, we herein describe the modified matrix rotation technique for UIQ tumors, which uses the “de-epithelialized dermoglandular flap-based matrix rotation technique.” We present our experience with the aesthetic and surgical outcomes of this modified matrix rotation technique in seven patients with UIQ tumors.
Methodology
This retrospective study involved all consecutive patients diagnosed with UIQ tumors at two tertiary care breast clinics in Sri Lanka. All patients with UIQ tumors were initially discussed at a multidisciplinary meeting. The suitability of the modified matrix rotation technique was determined by two surgeons specialized in breast surgery. All consecutive patients who underwent the modified matrix rotation technique for UIQ tumors from August 2022 to February 2023 were included in the study. Tumors invading the anterior skin were excluded from the study. The collected data included the patients’ demographics, clinicopathological details, perioperative details, surgical complications, and aesthetic assessments. All patients were followed up at 6 months.
Assessments
The following data were assessed:
Surgical outcomes: re-excision rate, resection margin, and complications, with surgical complications categorized according to the Clavien–Dindo classification Aesthetic outcomes: specific 6-month postoperative outcomes such as breast symmetry, breast volume, nipple position, and scar visibility using the previously described aesthetic items scale assessment tool,
5
which is a Likert scale questionnaire
The results were statistically analyzed using SPSS statistical software version 19 (IBM Corp., Armonk, NY, USA). The reporting of this study conforms to the CARE guidelines. 6
Surgical technique
Skin markings were drawn preoperatively with the patient in the standing position and the arms abducted and resting on the hips. The tumor location was marked with a 1-cm macroscopic clearance margin. A curved line with slight concavity was drawn from the mid-axillary line medially up to the 12-o’clock position of the breast. This curved line was placed 1 cm above the upper margin of the tumor. A triangle was drawn with the upper base at the medial corner of this line and the vertex oriented toward the NAC. The size of the triangle was dependent on the breast volume resected. A second small triangle was drawn at the lateral corner in the axillary region based on the Burow’s triangle principle, providing leverage for the rotational advancement flap. This also gave access to the area required for sentinel lymph node biopsy.
The surgical procedure was performed with the patient under general anesthesia. Initially, sentinel lymph node biopsy was performed through a lateral triangular incision. The large inverted triangular area was de-epithelialized to form a dermoglandular flap. An incision was made on the medial vertical limb of the triangle, and the skin flap was raised along the correct plane to perform wide local excision. This excision was extended up to the pectoralis major muscle posteriorly with adequate margins all around.
Next, the two triangles were joined along the skin incision, and the de-epithelialized dermoglandular flap was raised from the pectoralis major muscle just enough to allow its advancement medially to comfortably fill the defect. The tumor base was clipped, and hemostasis was achieved. The flap was positioned within the defect using anchoring stitches in the medial and superior pillars as required. The skin was approximated and sutured with absorbable stitches (Figures 1 and 3).

Schematic diagram depicting the surgical technique for an UIQ tumor at the 10- to 11-o’clock position, located far from the nipple–areolar complex. (a) Preoperative skin marking. (b) De-epithelialized inverted triangle at the level of the 12-o’clock position. (c) Wide local excision of the tumor, achieved by raising the flap through the medial vertical limb (black line). (d) Mobilization of flap into the defect by release from the pectoralis major muscle and (e) final outcome of the scar at the 12-o’clock position without breaching the UIQ. UIQ, upper inner quadrant.
Results
Our population sample comprised seven patients with a radiological and histological diagnosis of breast cancer in the UIQ. All patients were included in the study because all preferred the modified technique over the standard technique. The main reason for this preference as stated by the patients was the absence of a scar in the visible breast line with the modified technique. The patients’ mean age was 55.6 years (range, 42–72 years). All patients had T2 stage cancer according to the TNM classification. All patients underwent the operation by a single surgeon specialized in breast surgery. The mean length (horizontal limb) of the flap was 6.2 cm. No patients developed any surgical complications such as wound dehiscence or infection (Table 1).
Patients’ demographic and clinical characteristics.

*Wound dehiscence, surgical site infection, and fat necrosis of the flap.
NAC, nipple–areolar complex.
All patients were followed up at 6 months to assess the aesthetic outcomes based on the aesthetic item scale. 5 The patient-reported aesthetic outcome assessment demonstrated satisfactory results, with all four aspects scoring more than 9/10 (Table 2).
Patient-reported aesthetic outcome measurements at 6 months postoperatively.
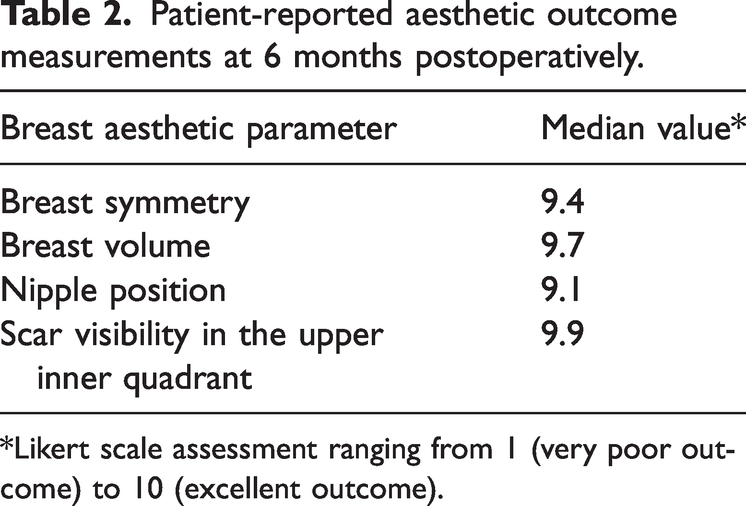
*Likert scale assessment ranging from 1 (very poor outcome) to 10 (excellent outcome).
Discussion
To our knowledge, this is the first study to analyze the modified de-epithelialized surgical technique to avoid a scar after treatment of breast tumors in the UIQ.
The UIQ has been described as “no man’s land” by Grisotti 7 because of the significant deformities and patient dissatisfaction caused by wide excision in this area. The surgical techniques described in the literature aim to address these issues as much as possible. However, no single technique is considered the standard or ideal.
The crescent mastopexy and round block techniques are good surgical options for tumors in the periareolar region and zone 1. The batwing approach is another method that has the advantage of avoiding an incision in the UIQ. However, the main disadvantages of these technique are that the NAC is invariably displaced upward and the technique is not suitable for tumors located far from the periareolar region. 8 Various mammoplastic techniques have also been described for UIQ tumors.9,10 These are more extensive surgeries that warrant contralateral symmetrization. 11 In the sociocultural background of Sri Lanka, patients are quite reluctant to undergo surgery in the normal breast, and this technique is not favored by many patients.
Another popular technique among breast surgeons is the matrix rotation technique using the Burow’s triangle. This technique is relatively simple and provides an adequate amount of glandular tissue to replace and reshape the breast, and it is suitable for UIQ tumors located far from the NAC. The main disadvantage of this technique is the need to excise the skin anterior to the tumor even when it is oncologically clear. This results in an unsightly scar crossing over the UIQ and appearing on the visible breast line4,12 (Figure 2).

Matrix rotation technique in a patient with a UIQ tumor with the scar extending to the UIQ (visible breast line). UIQ, upper inner quadrant.

Modified matrix rotation technique in a patient with a UIQ tumor. The scar does not encroach into the UIQ. (a) Skin marking. (b) De-epithelialized flap. (c) Wide local excision defect. (d) Mobilization of the flap to the defect and (e) postoperative result with no incision in the UIQ while retaining breast symmetry. UIQ, upper inner quadrant.
Because the UIQ is a cosmetically sensitive area for most patients, a minimum scar or deformity is the preferable outcome. We addressed this main drawback of the matrix rotation technique using the herein-described modified technique, avoiding an incision in the UIQ. The de-epithelialized flap is the key modification used to fill in the wide local excision defect. Neither the incision nor scar encroaches into the UIQ, which is the most visible part of the breast (Figures 2 and 4). In our study, the patients were given the choice between the standard and modified technique. All patients preferred the modified technique because of the absence of a scar in the UIQ. The postoperative patient-reported outcomes regarding breast shape, breast symmetry, and scar location were also satisfactory. The need for contralateral symmetrization was avoided because the breast shape and volume were almost equally restored. This technique is also well-suited and reliable for tumors located far from the NAC, as shown in our study sample; in our patients, the mean distance between the tumor and the NAC was 5.6 cm. Tumors located far from the NAC are the most challenging tumors in the UIQ for breast surgeons because of the limited options for scarless reconstruction. In the present study, the operative time was similar to that of standard wide local excision, and no complications were reported.

Modified matrix rotation technique in a patient with an UIQ tumor. The scar does not encroach into the UIQ. UIQ, upper inner quadrant.
The mean flap length in our study was 6.2 cm, and the mean tumor size was 2.9 cm. The flap length should be judiciously planned according to the defect size and the ability to fill the defect with dermoglandular rotation and advancement of the flap. A concern regarding this technique could be whether the de-epithelialized flap can maintain the blood supply to the fatty glandular tissue located away from the excised margin. In our study, the 6-month follow-up scans showed minimal fat necrosis of the flaps with good viability in all patients (Figure 5). A limitation of this study is the small number of patients, which probably occurred because breast cancer uncommonly presents in the UIQ. Therefore, further studies with larger sample sizes are required to improve our understanding of this technique and the maximum flap size that can be safely harvested for reconstruction.
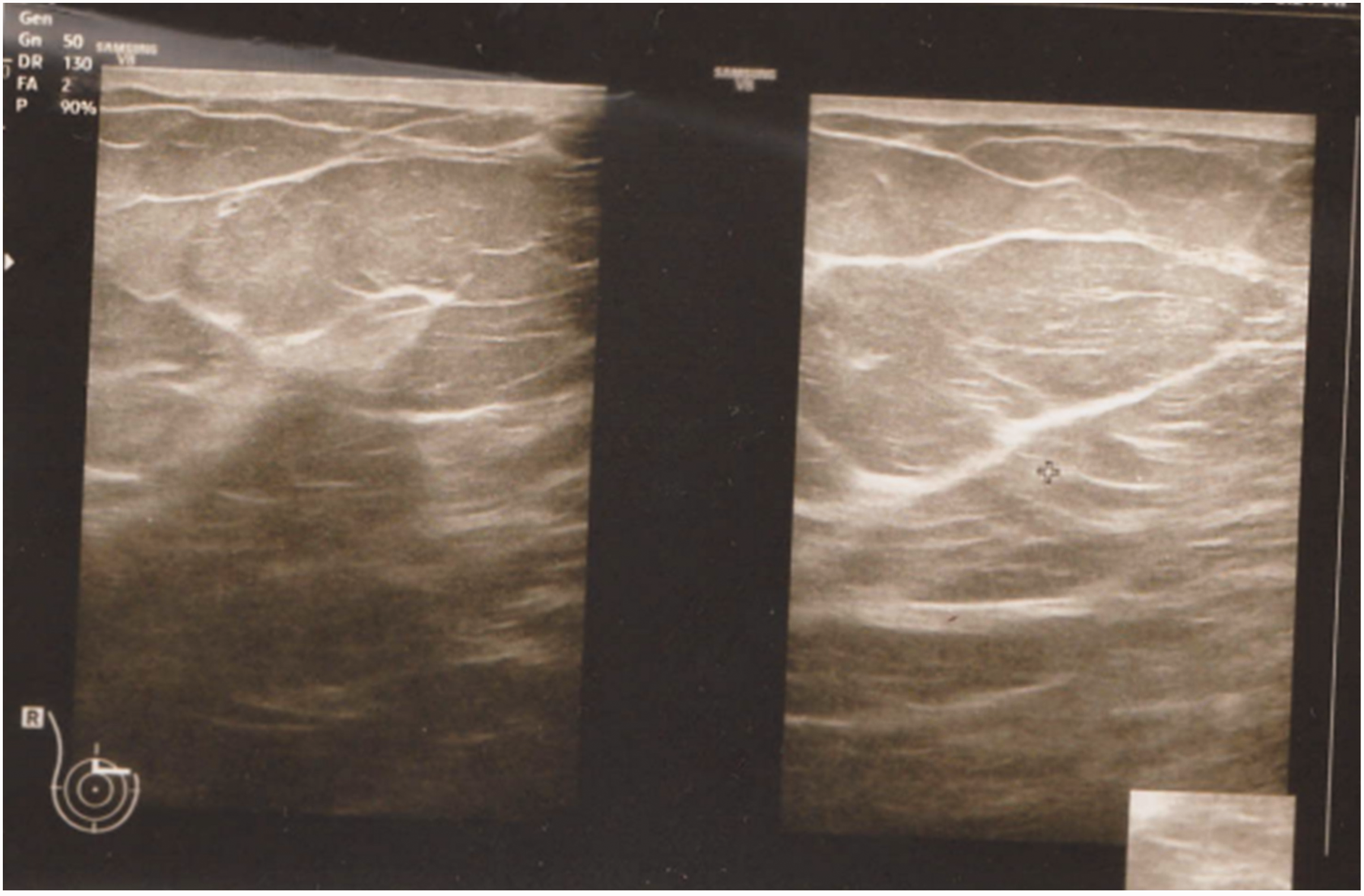
Six-month postoperative scan demonstrating a viable flap.
Conclusion
Tumors in the UIQ deserve surgeons’ close attention because a visible scar or deformity in this area can have a significant impact on overall patient satisfaction. The novel modification described in this report addresses the main drawback of the existing matrix rotation technique and results in a scarless UIQ. Our study demonstrates that the modified technique is aesthetically acceptable and addresses difficult-to-treat areas in patients with UIQ tumors.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241239852 - Supplemental material for Aesthetic and surgical outcomes of the modified matrix rotation technique for upper inner quadrant breast tumors: a case series
Supplemental material, sj-pdf-1-imr-10.1177_03000605241239852 for Aesthetic and surgical outcomes of the modified matrix rotation technique for upper inner quadrant breast tumors: a case series by Kanchana Wijesinghe, Umesh Jayarajah and Ajith De Silva in Journal of International Medical Research
Footnotes
Acknowledgement
We thank Mr. Bhanu Wijetilaka for his contribution to creation of the diagrams.
Author contributions
All authors contributed to the study conception and design. Material preparation and data collection and analysis were performed by all authors. The first draft of the manuscript was written by KW, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Consent
All patients provided written informed consent for participation in the study and publication of their anonymized images.
Data availability statement
All data are available in the article and data can be requested from the corresponding author.
Declaration of conflicting interest
All authors declare that there is no financial or non-financial conflict of interest.
Ethics
Our institution does not require ethical approval for reporting individual cases or case series. Nevertheless, approval was obtained for the publication of this article from the relevant institutional review board (Ethical Review Committee of the National Hospital of Sri Lanka, 21 April 2023; approval no. AAJ/ETH/COM/2023).
Funding
The authors declare that no funds, grants, or other forms of support were received during the preparation of this manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.