
Abstract
Impetigo herpetiformis is a rare variant of generalized pustular psoriasis that occurs during pregnancy or is triggered by pregnancy, often in association with hypocalcemia. This condition is associated with increased maternal and fetal morbidity and mortality. We report a 29-year-old pregnant woman who presented to hospital at the gestational age of 20 weeks with widespread erythema covered with pustules that coalesced to form lakes of pus. She did not respond to corticosteroids, immunosuppressants, or phototherapy. Finally, intra-amniotic injection of ethacridine lactate was administered to terminate the pregnancy, and the patient showed complete recovery in 3 months. Insight from this case report may facilitate optimal management of this relatively rare entity.
Introduction
Impetigo herpetiformis (IH) is a severe acute skin disorder that occurs during pregnancy. IH in pregnancy was first reported in 1966 and is an extremely rare condition. 1 Since 2000, only 350 cases of IH have been reported in the European and American literature. 2 We report a pregnant woman who presented at the gestational age of 20 weeks with widespread erythema covered with pustules that coalesced to form lakes of pus. The patient failed to respond to various treatments and showed rapid disease progression. Finally, intra-amniotic injection of ethacridine lactate was administered to terminate the pregnancy.
Case report
A 29-year-old pregnant woman (primipara; gestational age: 20 weeks) presented to hospital with a history of erythema, pustules, and itching since 1 month. The patient sought medical assistance at The First Hospital of Jilin University following 2 weeks of aggravation of symptoms. There was no family history of similar complaints. A physical examination showed widespread distribution of pin-sized pustules with erosions over an annular erythematic base over the torso and extremities (>40% of the body) (Figure 1). Laboratory parameters were as follows: leukocyte count, 14.17 × 109/L; neutrophils, 87%; erythrocyte sedimentation rate, 34 mm/hour (reference range, 0–20 mm/hour); serum C-reactive protein level, 117 mg/L (reference range, 0–3.5 mg/L); serum calcium level, 1.82 mmol/L (reference range, 2.11–2.52 mmol/L); total protein level, 49.0 g/L (reference range, 65.0–85.0 g/L); and albumin level, 23.1 g/L (reference range, 40.0–55.0 g/L). The patient was prescribed a once-daily regimen of dexamethasone 5 mg and gamma globulin 30 g, together with antibiotics to prevent infection. Moreover, we administered supplemental calcium to correct electrolyte abnormalities.

Photograph showing flaky erythematous lesions of different sizes symmetrically distributed over the surface of the body. A physical examination showed widespread distribution of pin-sized pustules with erosions over annular generalized pustules on an erythematous base. Some pustular lesions merged into pustular lakes.
Skin biopsy of the lesions showed spongiform pustules under the stratum corneum, acanthous hyperplasia and hypertrophy, spongy edema, and dilation of superficial dermal vessels. The perilesional areas showed moderate infiltration of lymphocytes and neutrophils (Figure 2). These findings were consistent with IH. All symptoms, except for pruritus, were alleviated with active treatment. Subsequent administration of topical agents and systemic UVB irradiation alleviated the itching. After 5 days, we replaced dexamethasone with methylprednisolone (60 mg once daily) because dexamethasone may have adverse effects on the fetus. Two days later, the patient developed pustules over the neck and under the breast folds. The lesions showed rapid exacerbation. Therefore, the dosage of methylprednisolone was increased to 80 mg once daily. However, the patient experienced recurrence of severe symptoms. Based on the patient’s condition, 150 mg cyclosporine was administered twice daily along with 100 mg thalidomide once daily. The patient and her family members were fully informed about the teratogenic effects of thalidomide before prescribing this drug. After detailed discussion, the patient and her family members consented to the use of this drug and signed the notification of drug use. The dosage of methylprednisolone was adjusted to 70 mg (administered intravenously). However, there was no significant improvement in symptoms. Itching and repeated appearance of new skin lesions was distressing for the patient. Ultrasound assessment of the fetus showed that the biparietal diameter was 5.5 cm, the femur length was 3.7 cm, cardiac activity was 148 times/minute; and gestational age was 22 weeks.

Results of a histopathological examination. Spongiform pustules were observed under the stratum corneum. Acanthous hyperplasia and hypertrophy, a spongy edema, and dilation of superficial dermal vessels surrounded by moderate infiltration of lymphocytes and neutrophils can be seen. The findings are consistent with impetigo herpetiformis. The arrow indicates pustules under the angular layer and epidermal edema (scale bar,×4; hematoxylin and eosin stain).
After detailed counseling, the patient and her family members voluntarily consented to termination of pregnancy. Subsequently, the dosage of cyclosporine was reduced to 125 mg twice daily, and avermectin A (Chongqing Huabang Pharmaceutical Co., Ltd., Chongqing, China.) (20 mg once daily) was prescribed. After 3 days, there was a new eruption of erythematosquamous plaques and herpetiform pustules, and the symptoms continued to persist. Despite various treatment regimens, the skin lesions were not fully alleviated and there was appearance of new skin lesions. Ultimately, ethacridine lactate was used for induction of labor. After using rivanol (Guangxi Hefeng Pharmaceutical Co., Ltd., Hechi City, China) for 44 hours, the patient gave birth to a dead female infant with a length of 26 cm and a weight of 420 g. The dead infant’s skin showed no erythema or herpetic lesions. Thereafter, intravenous methylprednisolone 40 mg was administered twice daily for 3 days. After the abortion, there was gradual alleviation of skin lesions with no new eruptions. The original lesions dried up and started falling off. There was flattening of papules with residual brownish pigmentation. Methylprednisolone was gradually tapered off and the patient was discharged 8 days after the procedure. However, the symptoms recurred 15 days post-discharge and the patient was readmitted. On re-initiation of treatment, the skin lesions subsided and the patient was subsequently discharged. One month after her delivery, her skin was normal, except for residual pigmentation. Her skin showed complete recovery 3 months postpartum.
Discussion
IH is a severe acute skin disorder that occurs during pregnancy. Owing to the similar clinical and histopathological features, IH is currently considered as a form of generalized pustular psoriasis. 3 This disease most commonly presents in the last trimester of pregnancy. IH may persist until delivery, but it rarely persists in the postpartum period. After delivery, the skin lesions tend to disappear after active medication. The survival rate of fetuses is higher in patients who develop IH in the third trimester. Additionally, neonates of patients tend to be healthy in such cases with no skin lesions after birth. The prognosis of the mother with IH and her child is good; however, there is a possibility of recurrence in subsequent pregnancies or during use of oral contraceptives. 4 Our patient presented in the second trimester of pregnancy and her symptoms were not alleviated, despite active treatment. Finally, IH was controlled by termination of pregnancy. Eruption of lesions characteristically develops symmetrically in the flexural and intertriginous areas and shows centrifugal extension. The lesions are erythematous patches with grouped sterile pustules at their margin. There may be post-inflammatory pigmentation after subsidence of plaques and pustules; however, there is no scar formation. IH is often accompanied by systemic complications, such as fever, tetany, an increase in leukocytes and neutrophils, a decrease in serum calcium levels, and hypoproteinemia. The disease course of IH is marked by periodic exacerbations. In severe cases, erosion of mucous membranes may occur over the tongue, oral cavity, and esophagus. 5 Timely diagnosis and treatment are imperative to achieve favorable outcomes owing to the recurrent disease course and the associated high risk of maternal and infant mortality. The clinical management of IH includes stopping progression of skin lesions and preventing potential complications. From the obstetric point of view, the main complications of IH are placental insufficiency and electrolyte imbalance.
There is a limited evidence base for treating IH. The main challenges are the critical condition of the mother and fetus and the possible teratogenicity of the drugs used for treatment of IH. The medical board of the National Psoriasis Foundation lists corticosteroids, cyclosporin, and infliximab as first-line treatments for IH. 6 Some case reports have documented rapid resolution of IH with biologics, most notably, infliximab, but also adalimumab, etanercept, and ustekinumab. However, the prohibitive cost of these drugs has limited our experience with these drugs. Financial constraints hampered the use of these drugs in our patient. A summary of IH systemic treatment is presented in Table 1.
Systemic treatment options for impetigo herpetiformis.
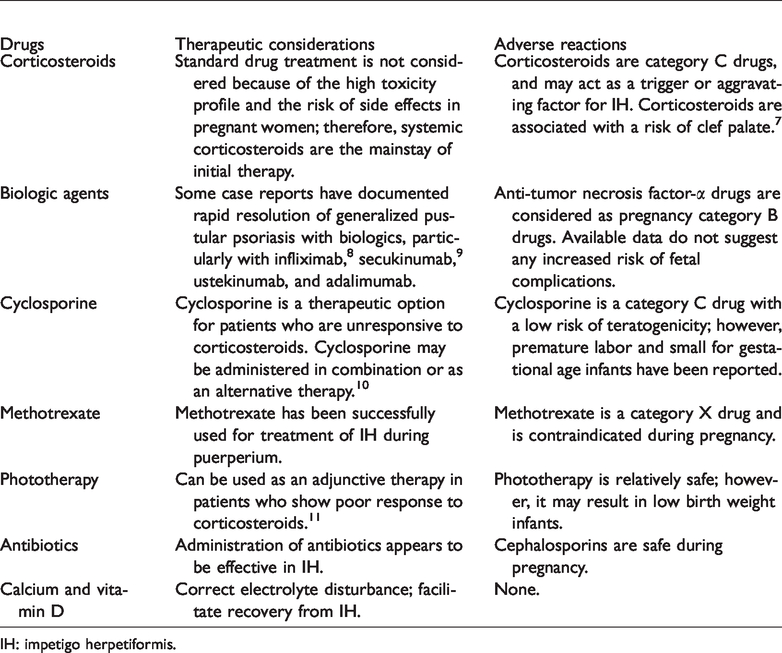
IH: impetigo herpetiformis.
Our patient’s condition did not respond to systemic treatment options. Because the patient was pregnant, medication use was restricted, with a consequent suboptimal therapeutic effect. The Chinese ethical standards allow for active induction of labor and termination of pregnancy if continuation of pregnancy is considered hazardous for the health of the pregnant woman because of some special reasons, and only termination of pregnancy and induction of labor can ensure the safety of the mother. The relapse in our patient 2 weeks after discharge was likely attributable to the excessive reduction in the dose of hormones and immunosuppressants. Therefore, following symptomatic improvement, the dosage must be decreased slowly under close monitoring to prevent exacerbation or recurrence of the disease.
The clinical diagnosis and treatment course of our patient may provide an important reference for clinicians managing IH in pregnancy. When pregnancy complicated by IH is clinically apparent and the symptoms are unabated, the pregnancy should be terminated as soon as possible. However, termination of pregnancy is not the ideal way to treat this disease. Therefore, development of more effective targeted drugs for the treatment of this disease is imperative.
Ethics
This report was approved by the ethics committee of the First Hospital of Jilin University. Written consent of the patient for publication of this case report was obtained in accordance with the principles of the Declaration of Helsinki.
Footnotes
Acknowledgements
We thank the Jilin Province Science and Technology Development Plan Project Fund for funding this report.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Jilin Province Science and Technology Development Plan Project Fund (20190304125YY).