
Abstract
Although selective coronary angiography is the gold standard diagnostic technique for coronary lesions, this method does not provide all information regarding pathophysiologic mechanisms. We herein describe a patient in their early 60s with a 3-month history of pronounced angina. Coronary angiography revealed a central line of illumination in the proximomedial segment of the right coronary artery, suggesting a chronic coronary dissection/recanalized thrombus, along with positive remodeling and TIMI grade 2 flow. Optical coherence tomography showed a recanalized thrombus and multiple lumens separated by thin septa. Because of the significantly reduced flow and signs of ischemia in the right coronary artery irrigation territory, we decided to perform percutaneous coronary intervention. Post-treatment optical coherence tomography indicated optimal apposition and expansion of the stents with positive remodeling of the blood vessel. We believe that decisions regarding treatment modalities should be guided by the presence or absence of ischemia. Lesions that are causing myocardial ischemia should be revascularized; otherwise, medical treatment can be utilized.
Keywords
Introduction
Coronary angiography is the gold standard diagnostic technique for coronary artery disease. 1 The most common coronary lesions are of atherosclerotic origin. By contrast, spontaneous coronary dissection, hematomas, and spontaneous recanalization of intracoronary thrombi are significantly less common. All of these lesions are associated with the same or similar clinical symptoms.2–4
The exact pathogenesis and epidemiological profile of non-atherosclerotic causes of coronary artery disease remain unclear, primarily because diagnosis is difficult. Although selective coronary angiography is the gold standard for the diagnosis of coronary lesions, this method does not provide all information about the pathophysiological mechanism underlying the formation of lesions of atherosclerotic and non-atherosclerotic origin. Additionally, non-atherosclerotic lesions are often unclear, which makes decisions regarding further treatment difficult.2,5,6
Identifying non-atherosclerotic lesions in the pathogenesis of ischemic heart disease is important. It enables early risk assessment of complications and acute coronary events, determination of the constituent components of the lesions, elucidation of the pathophysiological mechanism of their origin, and administration of adequate treatment.
We herein present a case of a honeycomb-like structure observed in a recanalizing thrombus confirmed by optical coherence tomography (OCT). Presentation of this case will provide useful information for interventional cardiologists regarding the diagnosis and treatment of angiographically unclear coronary lesions and will promote further research.
Case presentation
The patient described in this report provided written informed consent for both participation and treatment. We have de-identified the patient’s name and other details. Our institution does not require ethical approval for reports of individual cases. The reporting of this study conforms to the CARE guidelines. 7
A patient in their early 60s visited our hospital for elective coronary angiography because of a 3-month history of pronounced angina. The arterial pressure on admission was 130/80 mmHg, and the heart rate was 58 beats/minute. On 12-channel electrocardiography, the basic rhythm was sinus rhythm; rS formation was found in leads D3 and aVF, and shallow negative T waves were found in leads V2 to V6. The patient had been previously diagnosed with chronic heart failure with an ejection fraction of 29%. The patient’s new symptoms were characterized by typical anginal complaints, had lasted for 3 months, occurred even at rest, and stopped spontaneously. Two episodes of atrial fibrillation had been diagnosed 2 months previously, and the patient had since been on oral anticoagulant therapy (warfarin tablets). Echocardiography demonstrated a globally reduced ejection fraction (estimated at 29%) without segmental motion abnormality of the left ventricular wall; mild to borderline moderate mitral regurgitation was also present (estimated MR grade of 1+ to 2+). Because of the patient’s angina and absence of ischemia on echocardiography, a stress echocardiogram was performed. This revealed hypokinesis of the inferior wall during exertion. Coronary angiography revealed a central line of illumination in the proximomedial segment of the right coronary artery (RCA), suggesting a chronic coronary dissection/recanalized thrombus with positive remodeling and TIMI 2 flow. OCT was performed to evaluate the coronary angiography findings and to obtain detailed information about the lesion as well as the proximal and distal landing zones and the actual diameter of the RCA. This imaging examination revealed a recanalized thrombus and multiple lumens separated by thin septa; the thrombus had a diameter of 1.89 mm, whereas the diameter of the lumen proximal to the lesion was 3.13 mm. OCT also revealed a plaque with fibrotic components (diffuse thickening of the intima with high reflection and low attenuation), an organized thrombus of high intensity, and a central lumen divided by thin septa into multiple channels with a smooth interior. Because of the significantly reduced flow and signs of ischemia in the RCA irrigation territory on the positive stress echocardiogram, we decided to manage the lesion by percutaneous coronary intervention (PCI) revascularization. PCI was performed on the RCA with implantation of three drug-eluting stents measuring 3.5 × 13 mm, 3.5 × 28 mm, and 3.0 × 22 mm (Synsiro stents; BIOTRONIK, Bülach, Switzerland). Post-PCI OCT evaluation was then performed with an FD-OCT C7XR system (LightLab Imaging Inc., Westford, MA, USA) using a 6-Fr guide catheter-compatible Dragonfly DUO catheter (Abbott Vascular, Chicago, IL, USA) to optimize the PCI procedure in terms of adequate apposition, expansion, and confirmation of the absence of edge dissections. The OCT findings indicated optimal apposition and expansion of the stents, positive remodeling of the blood vessel, no edge dissection, and TIMI grade 3 flow (Figure 1).
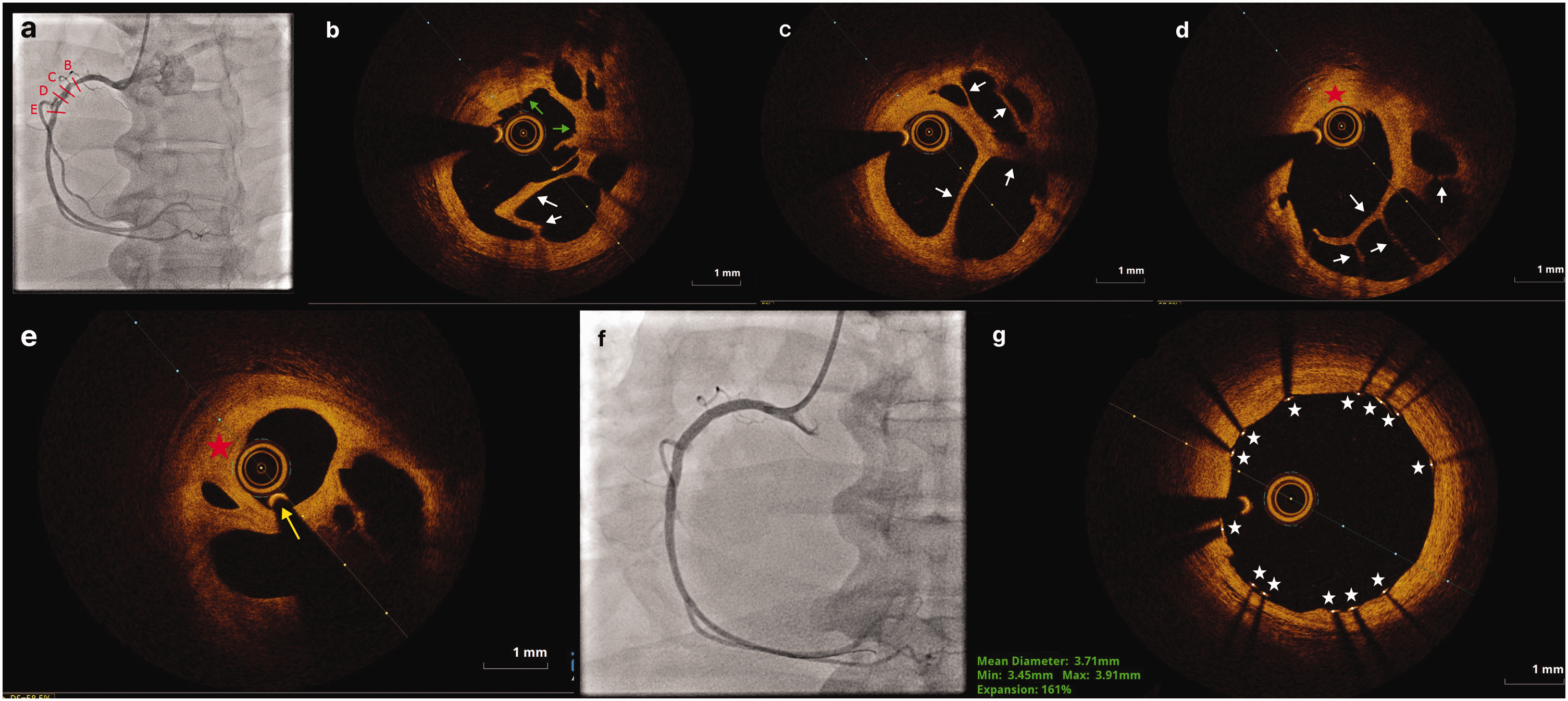
Findings of coronary angiography and optical coherence tomography (OCT). Coronary angiogram of the right coronary artery (RCA) in the (a) left anterior oblique view showed angiographic haziness and a central line of illumination in the proximomedial portion of the RCA (b, c, d, e). Representative cross-sectional OCT images of the RCA showed a honeycomb-like appearance and a recanalized thrombus with multiple microchannels. The red star indicates a diffuse heterogeneous plaque burden with fibrotic areas. The green arrows indicate an organized thrombus with high-intensity signal. The white arrows indicate the central lumen divided by thin septa into multiple channels. The yellow arrow indicates the guidewire within the central lumen. (f) The lesion was successfully treated with a sirolimus-eluting stent and (g) Postprocedural OCT demonstrated favorable expansion and apposition of the stent (white stars).
Discussion
The terms “honeycomb-like structures,” “Swiss cheese appearance,” and “lotus root-like appearance” in the literature refer to coronary arteries with multiple lumens interconnected by thin septa. These lumens converge proximally and distally into a single lumen, and individual walls containing all components are lacking.6,8,9 “Braid-like” or “woven” coronary arteries have a similar appearance; they are also characterized by multiple lumens, but the lumens are separated from each other by complete arterial walls with all three layers fully developed. 9 In both cases, most of the lumens are extremely small compared with the true lumen of the coronary artery proximal and distal to the site of the altered wall structure, and in many cases, they limit normal blood flow and require revascularization.6,8,10
The exact pathogenesis of honeycomb-like structures is unknown. There are hypotheses regarding dissection and inflammation as complications of atherosclerotic plaques as well as hypotheses regarding thrombus recanalization and neovascularization, tissue substitution after spontaneous dissection, and cardioembolic origin.2–4,11 The literature indicates that such structures occur more often in men than women, at an average age of approximately 50 years, and in active smokers with an average of >20 cigarettes per day; these data are consistent with our case report. Smoking is considered to be the main trigger for the formation of such lesions because smoking causes endothelial dysfunction and increased prothrombotic activity of platelets.10,12–14 The predominance of these lesions in men can be explained by the lower prevalence of risk factors for complications of atherosclerotic plaques in women (e.g., plaques rich in lipids, cholesterol crystals, and plaque rupture) and a higher prevalence of healed plaques with positive remodeling in women. 12 However, the representation of the two sexes in lesions of non-atherosclerotic origin cannot be adequately explained. The RCA is most often affected by these lesions, and the left circumflex artery is the least commonly affected. Cases in which such lesions exist simultaneously in two and all three coronary arteries have been described. 9 Reduction of coronary flow caused by the microchannels of these lesions can clinically present as stable ischemic heart disease, acute coronary syndrome, tachycardia, atrial fibrillation, ventricular tachycardia, absence of symptoms, and as an associated finding of the culprit lesion of acute coronary syndrome.8,10,15 The literature also contains a case of chronic total occlusion caused by a “honeycomb-like” structure 16 and a case of in-stent restenosis with a “honeycomb-like” appearance. 17
Accurate differentiation of unclear structures is impossible based only on the findings of coronary angiography. OCT examination helps to establish an accurate diagnosis because it can depict all components of arterial walls, differentiate atherosclerotic and non-atherosclerotic origins of lesions, detect vulnerable plaques according to the thickness of the fibrous cap and the degree of macrophage infiltration, and facilitate decision-making regarding adequate treatment of coronary lesions. The thin septa separating the lumens of “honeycomb-like structures” on OCT appear smooth, exhibiting strong reflections and weak attenuation. The septa are characteristically made of proteoglycans, which gives some parts of the septa a darker appearance. By identifying the markers of atherosclerosis (lipid infiltration, intimal thickening, hypervascularization, calcium nodules, and cholesterol crystals), OCT enables the exact pathogenesis of the structures to be defined. In the absence of atherosclerosis markers, lesions are considered to be of non-atherosclerotic origin. In such cases, the mechanism underlying their development can be explained by the hypotheses of spontaneous dissection and cardioembolization.2,4,9,18,19
In some studies, similar structures were interpreted as spontaneous dissections. 20 In our case, however, more microchannels developed to establish flow through the thrombus-occluded segment of the coronary artery. Research has shown predominance of women among patients with spontaneous dissection.21,22 We consider that the decisive factor in diagnosing a recanalized thrombus as the main cause of honeycomb-like structures is determined through the findings of OCT. These findings include the absence of microchannels penetrating the subintimal space, an intact intima, a fibrotic plaque, and an organized thrombus. Notably, a double-lumen structure on the initial coronary angiography examination may also indicate type I spontaneous coronary dissection. The presence of numerous small canals supports the diagnosis of a recanalized thrombus; this is in contrast to spontaneous dissection, which usually contains two or three lumens. Elements of chronic thrombosis indicative of thrombus recanalization have been histopathologically confirmed in cases of honeycomb-like structures.23,24
OCT also enables a precise assessment of the severity of the stenosis and length of the lesion, thus helping to determine the optimal treatment and material used for revascularization. 18 The tortuosity of blood vessels is considered to have a greater influence on the severity of stenosis in honeycomb-like structures than in other lesions, considering that the separated lumens already have reduced flow compared with the true lumen of the blood vessel. 25 PCI, cardiosurgical revascularization, implantation of bioresorbable scaffolds, balloon angioplasty, and conservative treatment of insignificant lesions have been described as treatment methods for such structures.4,6 Because these structures are rarely diagnosed, however, there are still no general recommendations for their treatment. The use of double-lumen catheters and parallel wire techniques have been described in the treatment of PCI lesions when the wire cannot pass through the multiple lumens. 26 Hydrophilic and polymer wires are most often used to pass these lesions. 10 Additionally, the effectiveness of using scoring and cutting balloons and the buddy wire technique to break through the microlumen septa has been described. 15 When such techniques are ineffective, the lesions can be treated with rotational atherectomy and intravascular lithotripsy.26,27 Although difficulties have been described in the passage of lesions with wires and the treatment of such lesions, an OCT catheter can easily pass these lesions, and no reports have described the impossibility of OCT imaging of these lesions. 26 The presence of reduced coronary lesions is often associated with a higher risk of triggering ventricular fibrillation when a large amount of contrast is injected during interventions. 10 Regardless of the method of treatment, these lesions have a good early and late prognosis. 28 Nevertheless, they are associated with a higher rate of compromised flow through the side branches during stenting, precisely because of the existence of multiple septa; compromised flow can be avoided by protection of the side branch.10,25,29 Using OCT in PCI lesions avoids suboptimal treatment results such as malposition, dissection, insufficient stent expansion, and later consequences related to major adverse cardiac and cerebrovascular events.2,30
Conclusion
“Honeycomb-like” structures are rarely encountered in clinical practice because of the difficulty of diagnosis based on coronary angiography findings and the nonspecific clinical symptoms and signs. Coronary angiography is insufficient for recognition of these structures because the true canaliculi are often not recognized and unclear filling defects are often mistaken for dissections. Establishing the correct diagnosis is very important for determining further treatment. OCT greatly facilitates the diagnosis and treatment of such lesions and reduces the complications of the procedure itself. OCT also provides information about the origin and mechanism of the formation of such lesions. We believe that decisions regarding the treatment modality should be guided by the presence or absence of ischemia. If the lesion has caused myocardial ischemia, it should be revascularized. When ischemia is absent, the lesion can be treated medically.
Data availability statement
According to our institutional policy, it is not possible to share data.
Supplemental Material
sj-mp4-1-imr-10.1177_03000605231213753 - Supplemental material for Diagnosis and treatment of angiographically unclear coronary lesions
Supplemental material, sj-mp4-1-imr-10.1177_03000605231213753 for Diagnosis and treatment of angiographically unclear coronary lesions by Bojan Maričić, Zoran Perišić, Tomislav Kostić, Nenad Božinović, Svetlana Apostolović, Sonja Šalinger, Tijana Maričić, Vladimir Vasilev, Stefan Juričić, Sonja Dakić, Jelena Perišić and Jelena Milošević in Journal of International Medical Research
Supplemental Material
sj-avi-2-imr-10.1177_03000605231213753 - Supplemental material for Diagnosis and treatment of angiographically unclear coronary lesions
Supplemental material, sj-avi-2-imr-10.1177_03000605231213753 for Diagnosis and treatment of angiographically unclear coronary lesions by Bojan Maričić, Zoran Perišić, Tomislav Kostić, Nenad Božinović, Svetlana Apostolović, Sonja Šalinger, Tijana Maričić, Vladimir Vasilev, Stefan Juričić, Sonja Dakić, Jelena Perišić and Jelena Milošević in Journal of International Medical Research
Supplemental Material
sj-mp4-3-imr-10.1177_03000605231213753 - Supplemental material for Diagnosis and treatment of angiographically unclear coronary lesions
Supplemental material, sj-mp4-3-imr-10.1177_03000605231213753 for Diagnosis and treatment of angiographically unclear coronary lesions by Bojan Maričić, Zoran Perišić, Tomislav Kostić, Nenad Božinović, Svetlana Apostolović, Sonja Šalinger, Tijana Maričić, Vladimir Vasilev, Stefan Juričić, Sonja Dakić, Jelena Perišić and Jelena Milošević in Journal of International Medical Research
Footnotes
Author contributions
B Maričić: Project development, Data analysis and review, Manuscript writing and editing. Z Perišić, T Kostić, N Božinović, S Apostolović, S Šalinger, T Maričić, V Vasilev, S Juričić, S Dakić, J Perišić, J Milošević: Data analysis and review, Manuscript writing and editing.
Declaration of conflicting interests
The authors declare no conflict of interest in preparing this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.