
Abstract
Abstract
Background
Pediatric headache is a common cause of pediatric emergency department (ED) visits, and 8.8% of cases require imaging. Alarmingly, 12.5% of imaged cases have a pathologic cause. A pediatric patient with a complicated medical history presented to the pediatric ED with multiple cerebral abscesses. The possible causes and contributors to this rare cause of pediatric headache and a review of pediatric headache emergency management are presented.
Conclusion
Managing pediatric headache in emergency settings requires a robust history and physical examination. Cerebral abscesses are an infrequent but fatal cause of pediatric headache and therefore should be considered among the differential diagnoses.
Keywords
Introduction
Pediatric headache is a relatively common occurrence in the emergency department (ED), and imaging is performed for 8.8% of those visits. 1 Alarmingly, 12.5% of those imaged are found to have a pathologic cause. 1 Although cerebral abscesses comprise only a small proportion of these cases, their relatively high morbidity and mortality rates require consideration when evaluating pediatric headache patients. We present a case of a pediatric patient with a complicated medical history who was found to have multiple cerebral abscesses. This report concludes with a review of the literature regarding evaluation and treatment of pediatric headaches and cerebral abscesses. This case highlights the rare condition of perforating folliculitis so that management and disposition in the ED setting can be optimized.
Case presentation
A 12-year-old male patient with a complex medical and surgical history, including post-repair pulmonary valve stenosis, presented to the pediatric ED because of intractable and worsening left frontoparietal headache for 6 days, which was refractory to ibuprofen. The patient also reported associated symptoms of vomiting, neck stiffness, and photophobia but denied focal deficits.
The patient's medical and surgical history included neonatal pulmonary valve stenosis with repair, gut malrotation repaired via the Ladd procedure, and gastroesophageal reflux repaired via Nissen fundoplication. Upon arrival to the ED, the patient's vital signs were within normal limits, including an oral temperature of 36.6°C, pulse of 65 beats per minute, 20 respirations per minute, blood pressure of 106/70 mmHg, and oxygen saturation of 100% on room air. A physical examination revealed severe photophobia and restlessness secondary to severe head pain, with no other significant findings. The visual acuity examination score was 20/20, and no pupillary or gaze defects were found. The patient had a motor strength score of 5/5 in the bilateral upper and lower extremities with no sensory deficits throughout, intact cranial nerves, and normal memory and cerebellar examination results. A psychiatric evaluation demonstrated normal judgment and insight along with normal-for-age speech and orientation, and the patient was cooperative throughout the examination.
Because of the level of pain and chronicity of the headache, the patient underwent non-contrast computed tomography (CT) of the brain, which demonstrated two round, bilateral, parietal hypodense lesions with surrounding vasogenic edema. The larger lesion on the right side measured 2.5 cm. No midline shift, hemorrhage, or hydrocephalus was observed. Because of the lack of contrast, it was difficult to differentiate whether the lesions were of neoplastic or infectious origin (Figure 1a–e).
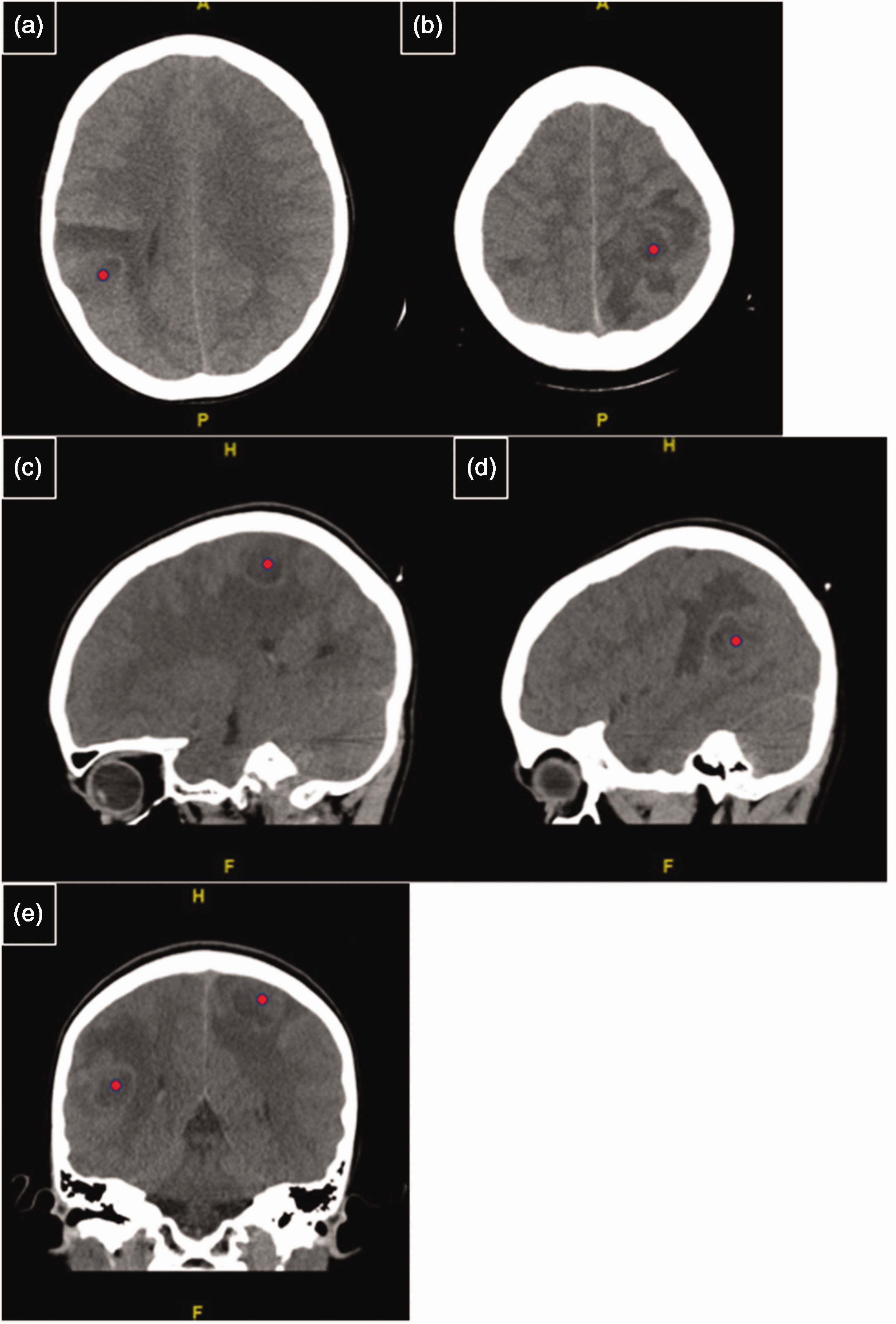
Brain computed tomography without contrast. (a, b) Right and left hemispheres with hypodense lesions (red dots) and surrounding vasogenic edema and (c, d) Sagittal images that also demonstrate the right and left hemisphere lesions (red dots), respectively. e: Both lesions (red dots) on a single coronal image.
The serum laboratory results showed a marginally elevated initial lactate level of 2.1 mmol/L, a normal white blood cell count of 12.9 × 103/µL, and marginal erythrocytosis with a hemoglobin level of 16.7 g/dL. The differential blood count, electrolytes, and C-reactive protein results were all normal, and viral polymerase chain reaction assays for coronavirus disease 2019 and influenza and blood culture results were all negative.
The ambiguity of the lesions necessitated transfer to a facility with pediatric neurosurgical capabilities, where the patient subsequently underwent magnetic resonance imaging (MRI) of the brain, with and without contrast. MRI demonstrated a right temporoparietal juncture mass measuring 3.2 cm and a left parietal lobe intra-axial mass of 3.6 cm. Both masses had a thick rim of enhancement and internal low T1/mildly high T2 signal centrally along with surrounding vasogenic edema. A third tiny nodular focus of enhancement was also found in the inferior right frontal lobe involving the gyrus rectus, measuring 2 mm with minimal adjacent edema. A questionable diffuse meningeal enhancement was also observed. While not definitive, the neuroradiology report favored an infectious etiology on the basis of the suspected diffuse leptomeningeal enhancement and restricted diffusion in the larger masses (Figures 2a–c, 3a–g, 4a–e).
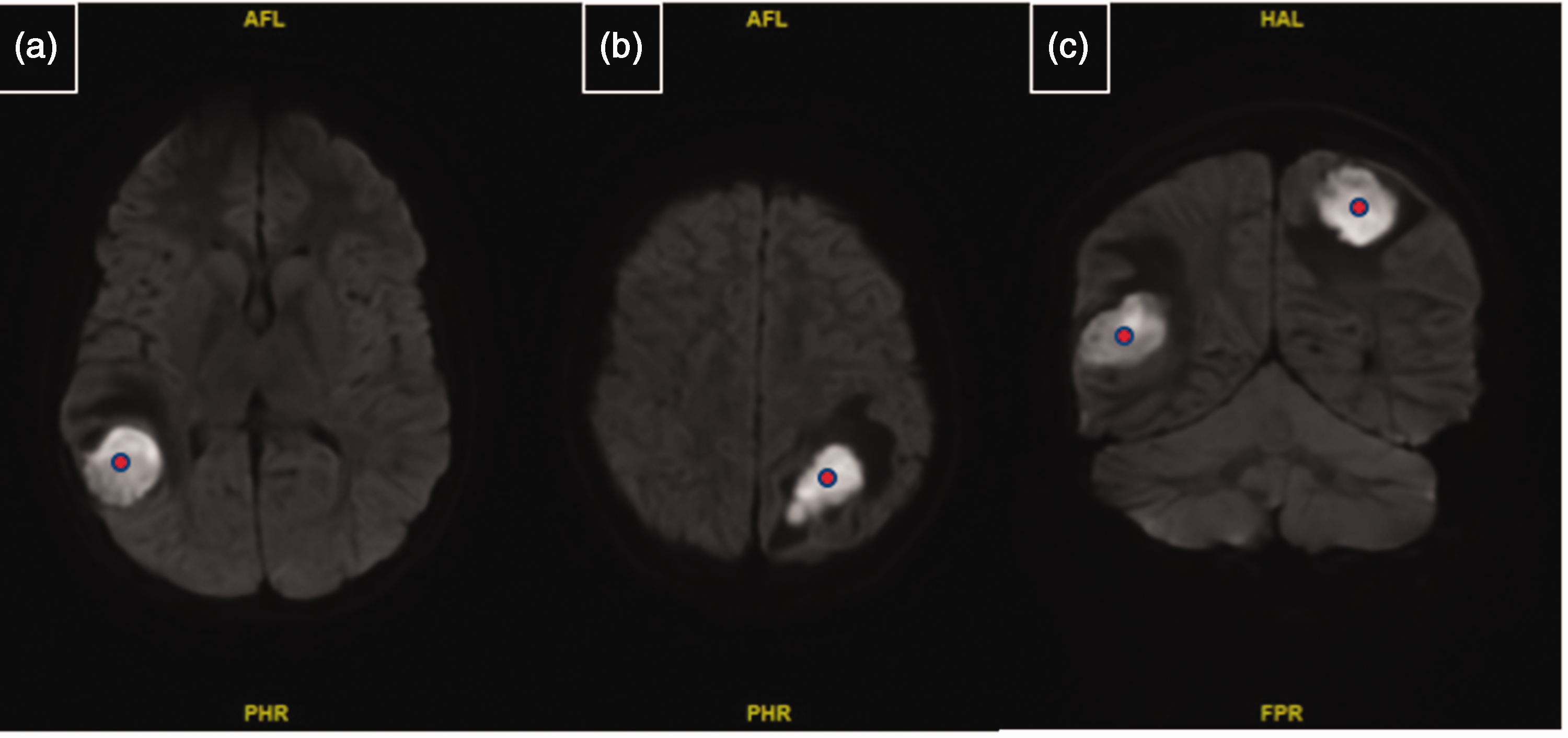
Diffusion-weighted imaging (DWI) of the brain with contrast showing restricted diffusion, leading to a high DWI signal in the lesion, likely caused by a fluid component. (a, b) Lesions (red dots) in the right temporoparietal juncture and left parietal lobe, respectively, with vasogenic edema and (c) Coronal view of both lesions (red dots) with vasogenic edema in one plane.
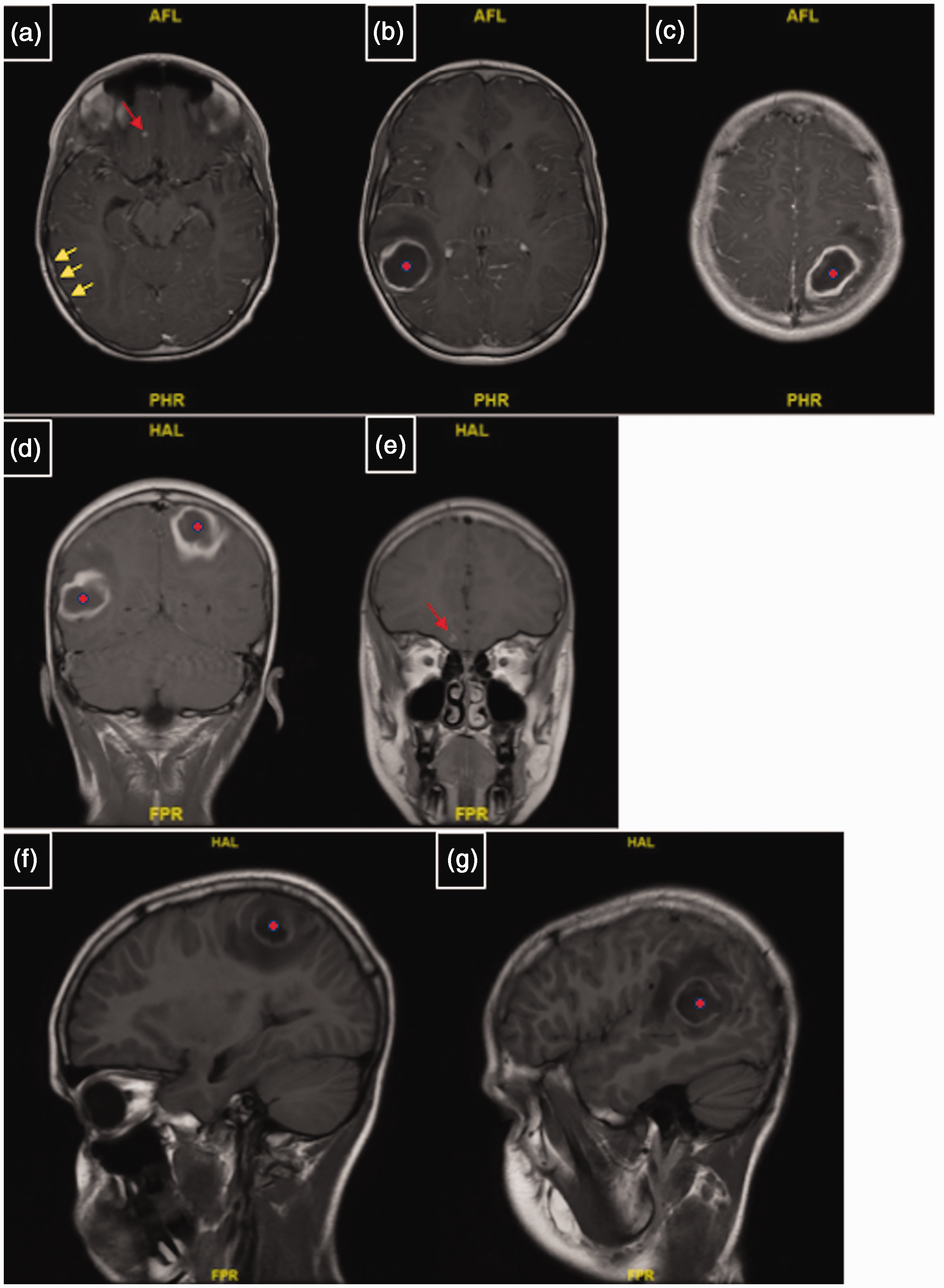
T1-weighted brain magnetic resonance imaging with contrast demonstrating peripheral enhancement of the lesions with low T1 signal. Leptomeningeal enhancement is present in all images (see panel a (yellow arrows) as an example). (a) Lesion in the right gyrus rectus (red arrow). (b, c) Lesions (red dots) in the right temporoparietal juncture and left parietal lobe, respectively, with a thick rim of enhancement and vasogenic edema. (d) Coronal view of both lesions (red dots). (e) Gyrus rectus lesion on coronal view (red arrow) and (f, g) Sagittal view of the lesions (red dots) in the left and right lobes, respectively, with surrounding vasogenic edema

T2-weighted brain magnetic resonance imaging with contrast demonstrating high T2 signal in the lesions with peripheral enhancement. (a) Lesion in the right gyrus rectus (red arrow). (b, c) Lesions (red dots) in the right temporoparietal juncture and left parietal lobe, respectively, with a thick rim of enhancement and vasogenic edema and (d, e) Sagittal view of the lesions (red dots) in the left and right lobes, respectively, with surrounding vasogenic edema.
While awaiting surgical exploration and possible drainage, the patient was treated with ketorolac and metoclopramide for symptom relief, as well as levetiracetam for seizure prophylaxis. Given the ambiguous nature of the lesions, the patient was not started on empiric antibiotic coverage in the initial ED visit but was given empiric ceftriaxone treatment at the receiving hospital. We did not attempt a lumbar puncture (LP), given the concern for a possible space-occupying lesion. Surgical exploration eventually revealed the lesions to be abscesses, which were successfully drained in the operating room. The abscesses were postulated to be related to the patient's pulmonary valve stenosis and repair; however, he did not undergo cardiology follow-up for confirmation. The patient made a full recovery and had complete resolution of symptoms without neurological compromise. The patient was lost to follow-up, and therefore, the causative bacterial species could not be determined. The reporting of this study conforms to the CARE guidelines. 2 The patient’s parents provided verbal and written consent for the publication of this report as well as consent for the treatment and transfer of the patient.
Discussion
Pediatric headaches
Primary headaches, defined as having an unidentifiable cause, comprise most headaches in the pediatric population and include migraine, tension-type, and cluster headaches. 3 Serious causes of secondary headaches include, but are not limited to, malignancy, elevated intracranial pressure because of acute obstructive hydrocephalus, carbon monoxide poisoning, intracranial infection, hemorrhage, or hypertensive crisis. Other less-severe causes of secondary headaches include temporomandibular joint dysfunction, idiopathic intracranial hypertension, and compromised vision.
Any child presenting to the ED with a headache should be screened for warning signs and comorbidities, which are outlined in Figure 5.1,4–10 If possible, the patient should undergo brain MRI or CT if MRI is not readily available. 11 Recent ED trends for headache examinations reflect this recommendation, with MRI rates increasing and CT rates declining. 12 Patients who lack warning signs, including signs of trauma, decreased neurologic function, and signs of increased intracranial pressure, do not require imaging because the rate of severe pathology in this population is less than 0.4%. 6 A patient with fever and meningeal signs without neurologic deficits should undergo LP. 13 Other patients who require LP include those with neuroimaging that failed to identify subarachnoid hemorrhage or those who are not within the time range to identify subarachnoid hemorrhage. 14 Oral analgesia such as acetaminophen or nonsteroidal anti-inflammatory drugs should be considered while awaiting test results in cases of primary headache. Refractory treatment includes a combination of intravenous fluids (20 mL/kg), ketorolac (0.5 mg/kg, maximum dose 15 mg), antiemetics such as metoclopramide (0.2 mg/kg, maximum dose 10 mg), and other medications such as magnesium or steroids, although these are typically reserved for explicit migraines.15,16

Pediatric headache algorithm. AMS, altered mental status; NF1, neurofibromatosis 1; MRI, magnetic resonance imaging; CT, computed tomography; NSAIDs, nonsteroidal anti-inflammatory drugs.
Regarding the order of operation for LP, antibiotics should be postponed until immediately after the LP. However, if imaging is required prior to the LP or the patient is unstable, antibiotics should be administered immediately (preferably after blood cultures have been obtained). 14 CT should be performed prior to LP if the patient is altered, is unstable, has papilledema, or has focal neurological findings. LP is contraindicated in patients with signs of elevated intracranial pressure, a space-occupying lesion with midline shift, or cerebral herniation. 17 Abnormal imaging findings should prompt an emergent neurosurgery consultation.
Pediatric cerebral abscess
The pediatric population has multiple predisposing factors for introduction of infection into the brain, as summarized in Table 1. 18 The most common causative organisms are Streptococcus pneumoniae and viridans streptococci, followed by Staphylococcus aureus, Staphylococcus epidermidis, and group B Streptococcus. 19 However, predisposing factors for the most likely causative organisms should also be considered (Table 1). 18 Another consideration is travel, particularly to areas endemic for neurocysticercosis caused by Taenia solium and other parasites such as Entamoeba histolytica, Schistosoma japonicum, and Paragonimus.18,20,21
Predisposing factors, causative agents, and management of cerebral abscess.

RIPE = Rifampin, Isoniazid, Pyrazinamide, Ethambutol. TMP-SMX = Trimethoprim Sulfamethoxazole.
Cerebral abscesses typically form over 10 to 14 days after the initial focal cerebritis. 22 Clinical symptoms typically include signs of elevated intracranial pressure such as headache, vomiting, and neck stiffness, as well as neurologic changes, fever, and seizures. The classic triad consists of unilateral headache, fever, and focal neurologic deficits. 18
Regarding the workup, LP is not recommended, even if meningitis is present, because of a theoretical risk of tonsillar herniation in patients with space-occupying lesions.13,19,23 MRI with contrast is the modality of choice and has a sensitivity and specificity of 95.2% and 100%, respectively, if used with diffusion-weighted imaging showing lesion hyperintensity. Other MRI findings include ring enhancement and internal capsule border thinning on T1-weighted imaging, a hypointense border with a hyperintense center on T2-weighted imaging, and hypointensity on apparent diffusion coefficient mapping. 24 However, CT is generally the initial imaging modality because of ease of access, despite its relatively low sensitivity for cerebral abscesses. 25 Additionally, CT scans may not detect early cerebritis. 25 Findings can include a dual rim sign (hypodensity on the outer rim representing granulation tissue and hyperdensity on the inner rim, which is better visualized by MRI) or a hyperintense ring, central pus manifesting as low attenuation, surrounding vasogenic edema (low density), and sometimes ventriculitis and obstructive hydrocephalus. 26 Serum laboratory testing of the white blood cell count is indicated but will not necessarily indicate or exclude disease. Serum blood cultures should be obtained, as cerebral abscesses often occur because of hematogenous spread. Most sources recommend routine and regular follow-up for at least 3 months post-abscess treatment because nearly 40% of cerebral abscesses will recur, and the vast majority of those will recur within 2 months. 27
Not all ring-enhancing lesions are cerebral abscesses, and the differential diagnoses are characterized by the popular MAGICAL DR mnemonic (Table 2). 28
MAGICAL DR mnemonic. This memory aide describes the differential diagnosis for a ring-enhancing lesion on brain magnetic resonance imaging.

Treatment of a pediatric cerebral abscess begins with prompt initiation of empiric antibiotics (Table 1) and will ultimately require neurosurgical consultation for drainage via stereotactic aspiration or craniotomy, although there is emerging evidence supporting more conservative management. 29
Conclusion
Given the ubiquitous and dynamic nature of non-traumatic pediatric headache ED visits, clinicians must use up-to-date guidelines to provide optimal care. The rate of pathologic etiologies of these headaches has been reported to be as high as 12.5%, but the majority of pediatric headache cases can be managed with empiric nonsteroidal anti-inflammatory drug intervention, as well as addressing the underlying causes. In the rare instance that imaging is needed, heavy preference should be given to brain MRI with and without contrast, although CT scanning is appropriate under certain circumstances, if it is more readily available. Cerebral abscesses are an infrequent but nonetheless fatal cause of pediatric headaches.
Footnotes
Author contributions
The authors accept direct responsibility for the manuscript. Each author made integral contributions to the report. Drs. Glenn Goodwin, Moshe Bengio, and Michelle Marin helped care for the patient during the initial visit, formulated the idea for publication, obtained verbal and written patient consent, and participated in follow-up interactions. Dr. Abhishek Roka formulated the pediatric headache flow chart, performed a literature review of cerebral abscess, and revised the manuscript. All of the authors participated in formulating and editing drafts of the manuscript and are listed in order of their contribution.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
The patient's parents provided verbal and written consent for publication of this report. Forms will be provided upon request. This case report was approved by the HCA Research Department Review Board (approval number: MS #2131 on 12 May 2023).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.