
Abstract
Collision tumour of the thyroid is a rare entity for which surgical resection is the primary treatment. We present here a case of a collision thyroid tumour of oncocytic and papillary carcinoma with lung metastases occurring in a 62-year-old woman who initially presented with a rapidly enlarging cervical mass and dyspnoea. The patient had extensive venous tumour thrombosis in the internal jugular and subclavian veins. The patient received six cycles of combined chemotherapy with nedaplatin and paclitaxel which significantly reduced the size of the metastases in the lungs. Following discharge from the hospital, the patient was treated with oral anlotinib and at 14 months follow up she had not experienced any serious side effects and the metastases in her lung and thyroid surgery areas were well controlled.
Background
Collision tumours occur when two different histological types of tumours occur in the same organ or anatomical site.1,2 These tumours may be primary, metastatic, benign or malignant, and can occur in any combination. Although rare, collision tumours have been described in multiple locations, including the thyroid gland; 3 these account for <1% of all thyroid malignancies and co-occurring medullary carcinoma and papillary carcinoma are the most frequent neoplasms.3,4 Thyroid collision tumours containing oncocytic carcinoma (OC) and papillary carcinoma are extremely rare.5,6
The management of thyroid collision tumours is challenging because of differences between the tumours in biological aggressiveness, treatment options, and prognosis. 4 A review article recommended that treatment plan decisions, which may include surgical resection, radioactive iodine therapy, chemotherapy, external radiotherapy and other adjunctive treatments, should be individualized based on the highly invasive components of the tumours, which will ultimately determine the patient's prognosis. 7
Platinum-based drugs and paclitaxel are recommended for the treatment of head and neck malignancies, and clinical trials have shown that paclitaxel is effective in the treatment of differentiated and locally advanced thyroid cancer.8,9 We report here a case of a collision thyroid tumour composed of oncocytic and papillary carcinoma with lung metastases that occurred in a 62-year-old woman. In describing details of the pathology, histology, treatment, and prognosis, we hope to provide useful insights into the treatment of this type of tumour.
Case presentation
A 62-year-old woman who had developed a lump on the left side of her anterior neck three months previously, presented to our hospital with a 10-day history of a rapidly enlarging cervical mass and dyspnoea. The patient had been diagnosed with hypertension 10 years ago, and reported that she had no history of neck radiation or family history of thyroid cancer or any other malignant tumours. Physical examination showed a significant swelling on the left side of her neck and a mass approximately 8.0 × 6.0 × 5.0 cm in size was palpated in the left lobe of the thyroid gland and front of the trachea; it had a firm texture and moved up and down with swallowing. The lower border and trachea were not palpable. Several other hard masses with indistinct borders and poor mobility were also detected in level II-V of the left neck, the largest of which measured 4.0 × 2.0 cm in diameter. While metastatic lymph nodes were initially considered, subsequently, an internal jugular vein tumour thrombosis was confirmed. No obvious enlarged lymph nodes were palpated on the right side of the neck, and there was no presentation of superior vena cava (SVC) syndrome. Bilateral vocal fold function was normal on fibreoptic laryngoscopy.
Ultrasound of the neck showed an asymmetrical thyroid lobe with marked enlargement of the left lobe and rightward deviation of the trachea by compression. A mixed hypoechoic heterogeneous nodule was detected in the upper middle lobe of the left thyroid (Chinese thyroid imaging reports and data systems [C-TIRADS]-4C). 10 An intense hypoechoic nodule with an unclear boundary was observed in the lower part of the right lobe, (size approximately 1.3 × 1.0 cm); it was extremely hyperechoic, with a rear acoustic shadow, and was graded C-TIRADS 4C (Figure 1).

Results from ultrasonography. (a) Ultrasound showed heterogeneous hypoechoic filling in the left internal jugular vein. (b) Colour Doppler flow imaging (CDFI) detection of blood flow signal filling defect at low echo tamponade. (c) The left subclavian vein showed hypoechoic filling, and CDFI detected the filling defect of blood flow signal at the filling site. (d) Heterogeneous nodules, approximately 6.0 × 4.5 cm in size, shown in left lobe. (e) CDFI showed more abundant branched blood flow signals. (f) Heterogeneous nodule approximately 4.8 × 3.5 cm in size with an unclear boundary show in upper part of the left lobe. (g) The lower portion of the left lobe showed an intense hypoechoic nodule, approximately 3.3 × 3.0 cm in size, with an unclear boundary; aspect ratio >1. (h) Left neck level IV lymph node was enlarged, and CDFI showed a blood flow signal and (i) An intense hypoechoic nodule, size approximately 1.3 × 1.0 cm, with an unclear boundary, shown in the lower part of the right lobe; it was extremely hyperechoic with a rear acoustic shadow.
Minimal hypoechoic nodules with an aspect ratio were found in the lower part of both thyroid lobes. Several other solid, cystic nodules were detected in the right lobe of the thyroid gland, and heterogeneous solid occupancy was observed in the left level II and III. Cervical vascular ultrasound showed possible tumour thrombus formation in the left internal jugular vein, beginning segment of left subclavian vein, and intraluminal filling of the left vertebral vein.
A computed tomography (CT) scan of the neck showed a mass in the left lobe of the thyroid gland, which was considered malignant. Multiple enlarged lymph nodes were detected in the left neck level II-VI, and metastasis was considered. There were small nodules in the right lobe of the thyroid gland. Multiple soft tissue shadows were found in the SVC and its dependent branches, with the possibility of embolism formation (Figure 1). CT scan of the chest suggested bilateral nodular disease in the lungs. Multiple lymph node enlargement was found in the mediastinum, and emphysema and pulmonary bullae were observed in both lungs.
Laboratory test results showed normal serum levels of thyroid-stimulating hormone (TSH, 3.7 µIU/ml), calcitonin (2.6 pg/ml) and carcinoembryonic antigen (CEA, 1.1 ng/ml). However, serum levels of thyroglobulin were significantly elevated (1217 µg/l). Thyroid related autoantibodies were within normal levels which excluded thyroid autoimmune disease.
Histological evaluation of multiple sections from the left lobe of her thyroid gland showed OC (Figure 2). The OC cells showed sheet and nest distribution with large nuclei and obvious atypia, with capsule and vascular invasion. Immunohistochemical staining showed tissue from the left lobe of the thyroid was negative for the following biomarkers: CgA; thyroglobulin (TG); CK19; HBME1; BRAF. However, positive staining was obtained for the following biomarkers: thyroid transcription factor 1 (TTF-1), weak +; PAX-8, +; Syn, partial +; Galectin-3, focal +; CD56, +; thyroid peroxidase (TPO), +; Ki-67 40%, +. Following multidisciplinary consultation, a diagnosis of OC was confirmed; the tumour had a large diameter with extensive venous tumour thrombosis, and was compressing the trachea which resulted in dyspnoea on minimal exertion.
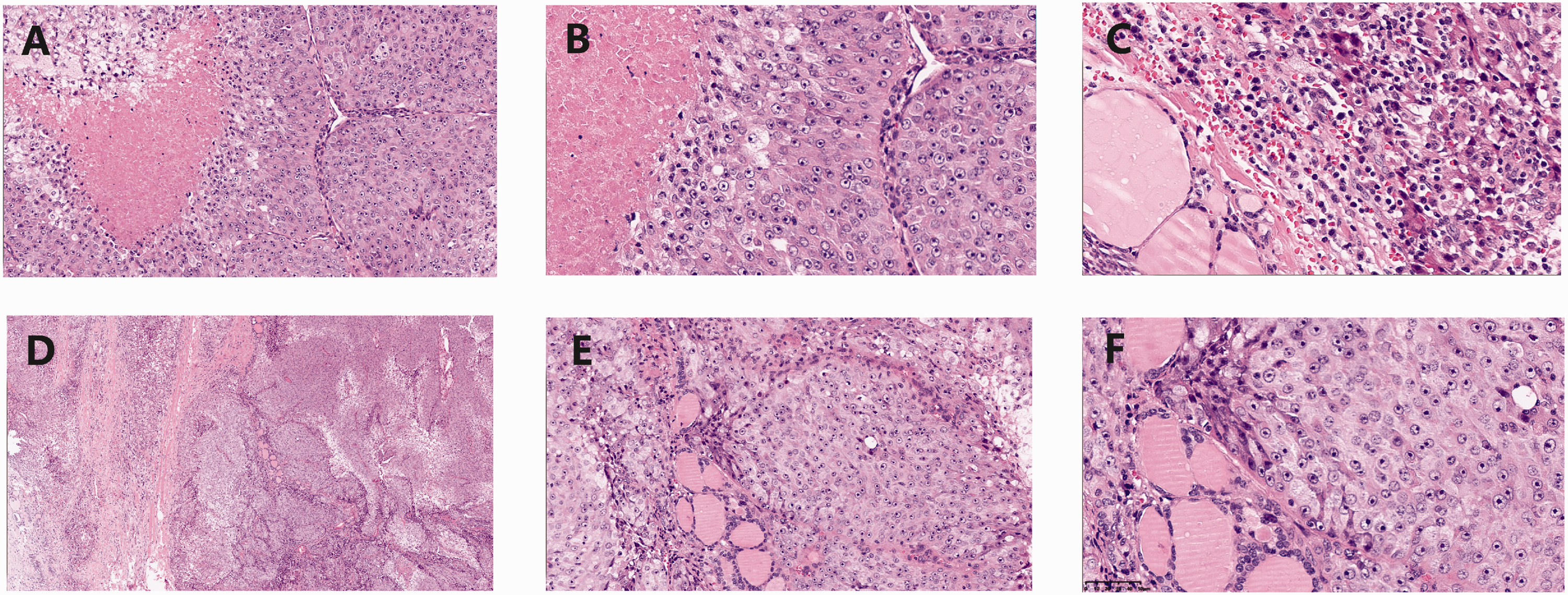
Histological findings. (a) Tumour cells were distributed in flakes and nests, with necrosis (haematoxylin and eosin staining; magnification ×20). (b) Oncocytic carcinoma (OC) characterized by tumour cells with abundant cytoplasm, eosinophilic staining, and obvious nucleoli (haematoxylin and eosin staining; magnification ×40). (c) Compared with normal follicle epithelium, OC cells are larger, the mesenchyme blood capillaries are dilated and congested (haematoxylin and eosin staining; magnification ×40). (d) In some regions, fibrous tissue proliferation around tumour cells was observed. (haematoxylin and eosin staining; magnification ×40). (e) In some regions, clear cytoplasm was observed (haematoxylin and eosin staining; magnification ×20) and (f) Tumour with large obvious nucleus, and mitoses is rare (haematoxylin and eosin staining; magnification ×40).
The patient underwent resection of right lobe and isthmus in the thyroid, palliative resection of the left lobe, and left central cervical lymph node dissection. Intraoperatively, the right lobe of the thyroid was seen to be normal in size and morphology, whereas the left lobe tumour was located in the posterior medial aspect of the gland with cystic infiltration and was closely adherent to the oesophagus, extending down to the posterior mediastinum. Postoperative pathology confirmed OC with cystic infiltration in the left lobe and papillary microcarcinoma in the right lobe (tumour diameter of approximately 0.60 cm; pT4bN2bM1). The OC component was in the left gland with lymph node metastasis, and the classic variant of papillary carcinoma was located in the right lobe without lymph node metastasis.
Compared with follicular thyroid carcinoma, oncocytic cells are less avid for radioiodine therapy, and so a whole-body scan following radioiodine therapy was not performed. Due to the extensive intravenous tumour thrombus, the vascular intervention team was unable to place a venous filter to prevent complications such as pulmonary embolism. Therefore, because the patient had multiple metastases in both lungs and mediastinal lymph node metastases, she was treated with six cycles of combination chemotherapy (i.e., nedaplatin 20 mg/m2 for three days and paclitaxel for injection (albumin bound) 260 mg/m2 for one day) with a 3-week interval between chemotherapy sessions.
Following two cycles of chemotherapy, the patient developed a right pulmonary pneumothorax, which resolved after administration of a closed chest drainage. The patient continued conventional chemotherapy until the end of the third cycle, and a CT scan showed a slight reduction in size of the nodule in the middle lobe of the right lung. A positron emission tomography/computed tomography (PET/CT) scan showed no new metastases. During the fifth cycle of chemotherapy, a pneumothorax developed in the left lung, which resolved after closed chest drainage. A CT scan at the end of the sixth cycle of chemotherapy showed that the metastatic nodules in both lungs had shrunk compared with the previous scans (Figure 3).

Nodules in the lungs. The arrows show the metastasized nodules. (a–d) Before chemotherapy; (e–h) Following three cycles of chemotherapy and (i–l) Following six cycles of chemotherapy.
Following discharge from hospital, the patient started oral treatment with anlotinib on a 21-day cycle (i.e., 10 mg/day for two weeks followed by one week of rest). As of the latest follow-up at 14 months, the patient has experienced no significant adverse effects and the metastases in the lung and thyroid surgery areas are well controlled.
The reporting of this study conforms to CARE guidelines. 11 Written informed consent was obtained from the patient to publish her anonymised data and the case report did not require ethics committee approval.
Discussion
Thyroid cancer is one of the most common endocrine malignancies, and accounts for approximately 3–4% of all malignancies. 12 Among thyroid malignancies, papillary carcinoma is the most common cell type, accounting for approximately 85% of cases. 12 Oncocytic cell carcinomas of the thyroid refer to invasive malignant neoplasms composed of >75% oncocytic cells, and account for approximately 5% of all thyroid cancers. 12 Compared with papillary carcinoma, OC is more prone to invade the thyroid capsule and surrounding blood vessels, and patients often present with local lymph node metastases or even distant metastases.13,14
Thyroid collision tumours composed of multiple histologic types are rare. 7 Collision tumours can be distinguished from mixed tumours by the presence of two separate components within the same tumour, both of which are primary and are often separated by normal glandular tissues. 15 Usually, only one tumour component in collision tumours can be diagnosed by preoperative fine-needle aspiration (FNA), while the second component is often an incidental finding by postoperative pathology. In our case, OC was found in the left side of the gland without other malignant components, and papillary cell carcinoma occurred in the right side of the gland. Although both originate from follicular epithelial cells, the two malignant components existed independently in the two lobes of the thyroid gland without areas of mutual fusion and therefore, were classified as collision tumours.
Most thyroid collision tumours have no specific clinical manifestations, and maybe diagnosed by physical examination or incidental palpation of a neck mass. While the course of thyroid collision tumours maybe long, when its infiltrative component predominates, it may manifest as a rapidly enlarging mass within a short period of time, which may be accompanied by symptoms such as pain, vocal cord dyskinesia, dyspnoea, and dysphagia. Moreover, the OC component of collision tumours can be aggressive and ultimately, can only be diagnosed in resected specimens. 16 Indeed, the diagnosis of OC requires one or more of the following features: tumour infiltration or penetration of the entire thyroid capsule; spreading to adjacent normal glandular tissue or penetration of the thyroid capsule into surrounding tissue; vascular infiltration; or local or distant metastasis.17,18 One report described a case of collision tumour formed by primary squamous cell carcinoma and papillary carcinoma, which presented as a rapidly growing right-sided neck mass accompanied by pain, localized dark red skin, and dysphagia. 19 Another study reported a case of collision tumour formed by anaplastic thyroid carcinoma and papillary carcinoma, which presented with hoarseness, inspiratory dyspnoea, and painless swelling of the left side of the neck, with the mass growing rapidly within four weeks. 13
In our case, the patient had a short course of disease and the mass in her neck grew rapidly within 10 days. Intraoperative exploration showed extensive invasion of the thyroid capsule and surrounding tissues, vascular invasion, and extensive tumour emboli, indicating the aggressive nature of the tumour. The incidence of thyroid cancer with tumour thrombosis is a rare occurrence and has been reported to have a prevalence of approximately 0.2–3.8% and is commonly seen in the advanced stages of differentiated thyroid cancer, indicating the strong aggressiveness of the tumor. 20 Our patient had a history of left heart failure. Due to her poor physical tolerance, we prioritized the resolution of the currently life-threatening respiratory distress and did not treat the tumour thrombosis, which at her last follow-up was stable.
There are limited reports related to the treatment of collision tumours, especially in cases involving OC with distant metastases. Therefore, it is difficult to determine whether standard treatment options, metastasis rates and prognosis for collision tumours are similar to those for single tumors.21,22 The consensus of opinion is that both entities in collision tumours should be considered as separate primary tumours, with different treatment options for different subtypes. For example, with respect to collision tumours with tissue components, such as OC, complete excision of the gland is required with simultaneous lymph node dissection if necessary. 3 One study reported that most patients with collision tumours had distant metastases by the time they presented to the hospital with symptoms. 7 Interestingly, the most common site of distant metastasis from thyroid cancer is the lung. 23
Because of their anti-proliferative and anti-angiogenic effects, tyrosine kinase inhibitors (TKI) have been used to treat radioiodine-refractory, locally advanced, or metastatic thyroid cancer. 24 Paclitaxel and platinum-based therapies have been shown to be effective in head and neck malignancies and in locally advanced differentiated thyroid cancer. 25 Anlotinib is a type of TKI, which inhibits tumour angiogenesis, and controls tumour growth by inhibiting related kinase activity. 26 In China, anlotinib has been approved and has been used as a novel therapeutic option in several cancers following chemotherapy. 27,28
In the case of our patient, we did not perform whole-body scan with radioiodine, or radioiodine therapy because she was considered allergic to iodine contrast agents. We surgically removed the thyroid gland to relieve her dyspnoea, and then treated the patient with a combination chemotherapy regimen of paclitaxel and nedaplatin. After a significant reduction in lung metastases, maintenance therapy with anlotinib was started. No recurrence or new distant metastases were observed at 14 months follow-up, demonstrating the favourable results of our treatment strategy. However, the patient developed pneumothorax twice during chemotherapy. Further studies are needed to confirm whether pneumothorax is associated with the administration of chemotherapy or lung metastasis of the tumour, and whether it is an indicator of poor prognosis.
In summary, in this case report we described a case of a thyroid collision tumour consisting of OC and papillary carcinoma with extensive tumour thrombosis and pulmonary metastasis, which was effectively controlled by chemotherapy with paclitaxel combined with nedaplatin and followed by targeted therapy with anlotinib. For tumours that progress rapidly in a short period of time, pathologists need to examine resection specimens carefully and be aware of the development of collision tumours, especially those containing poorly differentiated cancerous tissues, to avoid missing the relevant diagnosis.