
Abstract
Objective: To determine the relationship between coagulation system markers and hyperbilirubinaemia in full-term neonates.
Methods: This retrospective case–control study enrolled full-term neonates with hyperbilirubinaemia and healthy control full-term neonates. Prothrombin time (PT), thrombin time (TT), fibrinogen (Fbg), activated partial thromboplastin time (APTT) and international normalized ratio (INR) were recorded. The correlation between INR and total bilirubin and between INR and indirect bilirubin was analysed by linear regression analysis. Receiver operating characteristic curve analysis was used to assess the efficacy of INR to identify neonates with hyperbilirubinaemia.
Results: This study enrolled 40 full-term neonates with hyperbilirubinaemia and 30 healthy controls. PT, INR and APTT were significantly higher in the neonates with hyperbilirubinaemia compared with the healthy controls. There was a significant positive correlation between INR and the level of total bilirubin in neonates with hyperbilirubinaemia (R = 0.3327). There was also a significant positive correlation between INR and the level of indirect bilirubin in neonates with hyperbilirubinaemia (R = 0.3406). INR in neonates with hyperbilirubinaemia significantly achieved an area under the curve of 0.800 (95% confidence interval, 0.6288, 0.9712; cut-off value, 1.060; specificity, 71.43%; sensitivity, 80.00%).
Conclusion: These findings suggest that INR is a novel biomarker for the diagnosis of neonatal hyperbilirubinaemia in full-term neonates.
Introduction
Neonatal hyperbilirubinaemia is a common phenomenon during the neonatal period. 1 Hyperbilirubinaema is a major risk factor for brain damage caused by bilirubin-induced neurological dysfunction. 2 Hyperbilirubinaema manifests as a yellowish colour of the skin and mucous membranes. 3
Neonatal jaundice induces blood incompatibility. 4 Some studies have shown a correlation between neonatal hyperbilirubinemia and glucose-6-phosphate dehydrogenase deficiency, serum vitamin D levels and anti-streptolysin O haemolytic disease.5,6 Hyperbilirubinaemia can be caused by erythrocyte membrane defects and red blood cell enzyme deficiencies.7,8 With regard to the coagulation system, the interaction of coagulation factors has been found to go beyond their traditional effects and to affect some diseases.9,10 Therefore, there could be a correlation between the occurrence of hyperbilirubinaemia and changes in coagulation variables.
The present study measured the relationship between prothrombin time (PT), thrombin time (TT), fibrinogen (Fbg), activated partial thromboplastin time (APTT) and hyperbilirubinaemia in full-term neonates.
Patients and methods
Study design and population
This retrospective case–control study enrolled consecutive full-term neonates with hyperbilirubinaemia and consecutive healthy neonates born in the newborn wards of Chengdu Second People’s Hospital, Chengdu, Sichuan Province, China between October 2019 and September 2020. The inclusion criteria were as follows: (i) full-term of either sex; (ii) no significant illness; (iii) no major congenital malformation; (iv) no prior use of other complementary treatments, such as medicinal or herbal treatments, in addition to phototherapy. The exclusion criteria were as follows: (i) conditions that could aggravate hyperbilirubinaemia, including sepsis, respiratory distress syndrome, asphyxia, mothers with diabetes mellitus or intrauterine growth retardation.
The study was approved by the Ethics Committee of Chengdu Fifth People’s Hospital, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan Province, China (no. 20210216) and conducted according to the principles of the Declaration of Helsinki. Written informed consent was obtained from all of the parents of the neonates before any procedures were performed. All patient details have been de-identified.
Laboratory methods
Whole blood samples (3 ml) were collected from each full-term neonate. Blood was allowed to clot, centrifuged at 3000 g for 10 min at 4 °C in a centrifuge (KDC-3000R; Zonkia Scientific Instruments, Hefei, China), and the resulting serum was stored at –70 °C. Hyperbilirubinaemia was determined by measuring the serum total bilirubin level and observing the clinical manifestations on the second day after birth before they were discharged from the hospital. A total bilirubin level > 34 µmol/l was considered to indicate hyperbilirubinaemia. Serum total bilirubin levels were measured by using a LABOSPECT 008 α Hitachi Automatic Analyzer (Hitachi Medical Corporation, Tokyo, Japan) according to the manufacturer's instructions. Venous blood samples were collected and sent for PT, TT, Fbg and APTT analyses. The international normalized ratio (INR) was calculated.
Statistical analyses
All statistical analyses were performed using GraphPad Prism 8 (Graphpad Software Inc., San Diego, CA, USA). Data are presented as mean ± SD. An unpaired t-test was used to compare the two groups and linear regression analysis was used compare the correlations as measured by Pearson’s Correlation Coefficient. A P-value < 0.05 was considered statistically significant.
Results
This retrospective case–control study enrolled 40 full-term neonates with hyperbilirubinaemia and 30 healthy control full-term neonates. No asphyxia or inflammation occurred in any of the 70 neonates. Baseline clinical characteristics were similar in the two groups (Table 1), but there were significant differences in white blood cell count, platelet count and haemoglobin levels (P < 0.0001 for each comparison).
Clinical and demographic characteristics of full-term neonates with hyperbilirubinaemia (n = 40) and full-term healthy control neonates (n = 30) that were included in a study to determine the relationship between the coagulation system and hyperbilirubinaemia.

Data presented as mean ± SD or n of patients.
Unpaired t-test; NS, no significant difference (P ≥ 0.05).
A comparison of the two groups in terms of coagulation variables demonstrated that PT, INR and APTT were significantly higher in the neonates with hyperbilirubinaemia compared with the healthy controls (Table 2) (P ≤ 0.0001 for each comparison).
Comparison of various coagulation characteristics of full-term neonates with hyperbilirubinaemia (n = 40) and full-term healthy control neonates (n = 30) that were included in a study to determine the relationship between the coagulation system and hyperbilirubinaemia.
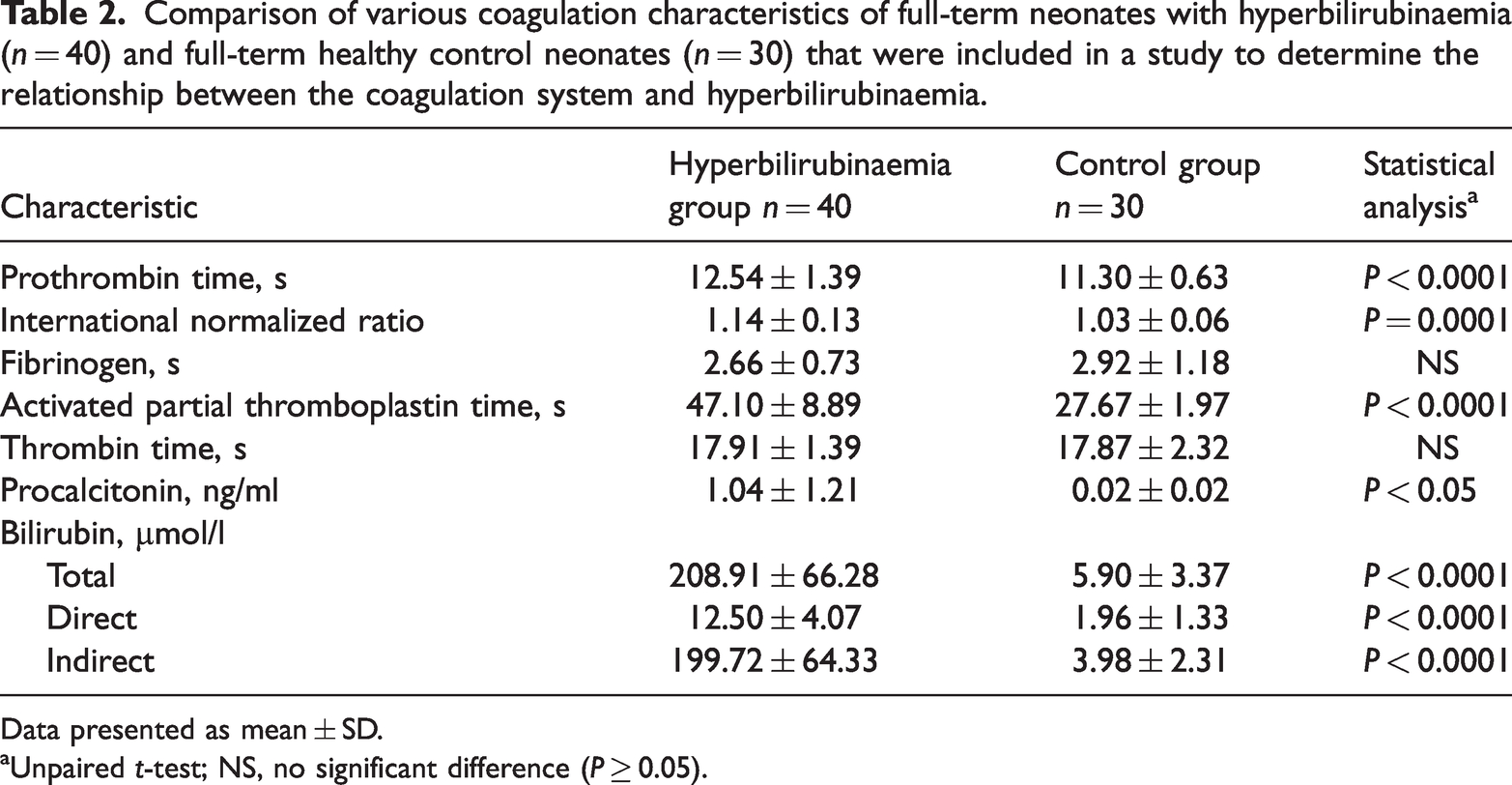
Data presented as mean ± SD.
Unpaired t-test; NS, no significant difference (P ≥ 0.05).
There was a significant positive correlation between INR and the level of total bilirubin in neonates with hyperbilirubinaemia (R = 0.3327; P < 0.0001) (Figure 1). There was also a significant positive correlation between INR and the level of indirect bilirubin in neonates with hyperbilirubinaemia (R = 0.3406; P < 0.0001) (Figure 2). Receiver operating characteristic curve analysis was used to assess the efficacy of INR to identify neonates with hyperbilirubinaemia. INR in neonates with hyperbilirubinaemia significantly achieved an area under the curve of 0.800 (95% confidence interval, 0.6288, 0.9712; cut-off value, 1.060; specificity, 71.43%; sensitivity, 80.00%) (Figure 3).

Linear regression analysis between international normalized ratio (INR) and total bilirubin levels (R = 0.3327; P < 0.0001) in full-term neonates with hyperbilirubinaemia (n = 40) that were included in a study to determine the relationship between the coagulation system and hyperbilirubinaemia.

Linear regression analysis between international normalized ratio (INR) and indirect bilirubin levels (R = 0.3406; P < 0.0001) in full-term neonates with hyperbilirubinaemia (n = 40) that were included in a study to determine the relationship between the coagulation system and hyperbilirubinaemia.

Receiver operating characteristic curve analysis for international normalized ratio (INR) in full-term neonates with hyperbilirubinaemia (n = 40) that were included in a study to determine the relationship between the coagulation system and hyperbilirubinaemia. AUC, area under the curve.
Discussion
This retrospective case–control study found relationships between several coagulation tests and hyperbilirubinaemia in full-term neonates. The mean PT and APTT were significantly higher in the neonates with hyperbilirubinaemia compared with the healthy control neonates. The mean serum procalcitonin level was also significantly higher in the neonates with hyperbilirubinaemia compared with the healthy control neonates. In this current study, white blood cell count, platelet count and haemoglobin levels were significantly higher in the neonates with hyperbilirubinaemia compared with the healthy control neonates. This current study also demonstrated significant positive correlations between INR and total bilirubin (R = 0.3327; P < 0.0001) and between INR and indirect bilirubin (R = 0.3406; P < 0.0001).
Hyperbilirubinaemia often occurs in infants without any apparent reason. 11 The aetiology of and the effective prevention strategies for hyperbilirubinaemia have been described in clinical guidelines. 12 There has been extensive research and progress on the main causes of neonatal hyperbilirubinaemia. 13 Compared with another study, 14 this current study used INR to evaluate the correlation between hyperbilirubinaemia and coagulation. The coagulation system is easily activated by inflammation and severe disease in humans. 15 Therefore, this current study evaluated PT and APTT in neonates with hyperbilirubinaemia compared with healthy controls; both coagulation variables were significantly prolonged in the neonates with hyperbilirubinaemia. Receiver operating characteristic curve analysis was used to assess the efficacy of INR to identify neonates with hyperbilirubinaemia; and it achieved an area under the curve of 0.800 (95% confidence interval, 0.6288, 0.9712; cut-off value, 1.060; specificity, 71.43%; sensitivity, 80.00%).
In conclusion, the findings of this current study suggest that hyperbilirubinaemia in neonates might induce changes in the coagulation system. Alternatively, a change in the coagulation system might cause early hyperbilirubinaemia. It appears that these changes could potentially be pathogenic in neonates because a high platelet count could be problematic. In our opinion, the coagulation system should also be considered when hyperbilirubinaemia is observed in neonates. These current findings suggest that the INR is a novel biomarker for the diagnosis of neonatal hyperbilirubinaemia in full-term neonates.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231207531 - Supplemental material for Coagulation profile of neonates with hyperbilirubinaemia in full-term newborns
Supplemental material, sj-pdf-1-imr-10.1177_03000605231207531 for Coagulation profile of neonates with hyperbilirubinaemia in full-term newborns by Fangye Zhou, Min Huang and Guangjie Zhang in Journal of International Medical Research
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.