
Abstract
Objective
To develop and compare four predictive models for intraoperative acquired pressure injury (IAPI) in surgical patients.
Methods
One hundred patients undergoing various surgeries (hepatobiliary, pancreas, spleen, gastrointestinal, and cardiac surgeries) at Ruijin Hospital from November 2021 to September 2022 were included in this prospective cohort study. Four pressure injury risk assessment scales were used to measure the pressure injury risk: the Braden scale, Munro Pressure Injury Risk Assessment Scale, Scott Triggers tool, and CORN Intraoperative Acquired Pressure Injury Risk Assessment Scale. The patients were divided into the IAPI group and non-IAPI group.
Results
In total, 37% of patients (37/100) developed class I/stage pressure injury (erythema) after surgery, which resolved within 2 hours after surgery in 86.49% of cases and further progressed to class II/stage or higher pressure injury within 6 days in 15.63% of cases. The application effects of the four commonly used risk assessment tools were compared with the sensitivity, specificity, and area under the receiver operating characteristic curve. The Munro Scale showed the best sensitivity and area under the receiver operating characteristic curve among the four tools for postoperative assessment, but its specificity was only 20.63.
Conclusions
More appropriate assessment tools are required for IAPI risk evaluation.
Keywords
Background
A pressure injury (PI) is a local skin and/or soft tissue lesion at a bony prominence or at the site of contact with a medical instrument. 1 PIs are associated with increased morbidity rates, hospital stays, and health care costs. 2 Such injuries are adverse events that can affect surgical patients. 3 A 2016 study showed that 3.5% of major surgical patients developed hospital-acquired PIs and that these PIs added $8200 to the cost of a surgical stay after adjusting for comorbidities, patient characteristics, procedures, and hospital characteristics. These ulcers increased hospital costs by 44% per hospital stay.4,5
Patients who undergo prolonged surgery also easily develop PIs, which are called intraoperative acquired PIs (IAPIs). 6 A systematic review showed that the incidence of IAPI ranged from 0.3% to 57.4%.7,8 Moreover, the occurrence rate of PI is two to three times higher in surgical patients (8.1%–54.8%)9,10 than in all admitted patients (3.3%–14.7%).11,12
It is generally agreed upon that the key to reducing the incidence of IAPI is to find an objective, noninvasive, automatic, and consistent scientific method for predicting IAPI. 13 Although several risk assessment scales for PI are available, the Braden scale is the most commonly used measure in China and abroad. However, some studies have indicated that this scale has a limited ability to predict the risk of ulcers in different populations and clinical environments. 14 The Munro Pressure Injury Risk Assessment Scale is the first PI scale to be specifically developed for surgical patients. However, its use is relatively cumbersome because of the large number of assessment items and the need for some items to be evaluated with the assistance of anesthesiologists. As a result, the Munro Pressure Injury Risk Assessment Scale is not widely used in the clinical setting. 15 The Scott Triggers tool includes four items, namely age, serum albumin level, estimated surgery time, and American Society of Anesthesiologists (ASA) score, 16 which can reduce the workload of clinical nurses; however, its efficacy needs to be further studied. Finally, the CORN Intraoperative Acquired Pressure Injury Risk Assessment Scale was developed by the Operating Room Nursing Committee of the Chinese Nursing Association in recent years to assess the risk of IAPI during the perioperative period. The effect of its application needs to be further studied. Therefore, selection of the most appropriate assessment tool is an important clinical problem for perioperative nurses.
Aims
The incidence of surgery-acquired PI is an important indicator of the quality of nursing in the operating room and has received significant attention from operating room managers. 17 Risk screening and assessment are essential methods for reducing the incidence of IAPI. Four main risk assessment scales are currently used in perioperative PI risk assessment: the Braden scale, Munro scale, Scott Triggers tool, and CORN Intraoperative Acquired Pressure Injury Risk Assessment Scale. This study was performed to compare the effectiveness of these four risk assessment scales in predicting the incidence of IAPI in adult patients undergoing surgery under general anesthesia. The overall aim was to provide a reference for screening patients at high risk of IAPI.
Methods
Sample
A prospective study was conducted in Ruijin Hospital from November 2021 to September 2022 and included 100 patients undergoing hepatobiliary, pancreas, spleen, gastrointestinal, and cardiac surgery. No participants had any PIs upon admission, and all underwent surgery with an operation time of ≥3 hours during their hospital stays. The occurrence of PI was considered when such injuries appeared within 3 days after surgery. Patients who developed postoperative erythema that resolved within 2 hours were also included. All patients were required to provide written informed consent and volunteer to participate in the study. Patients who underwent repeated surgery were excluded.
Data collection
A preoperative assessment was conducted by uniformly trained researchers using the four risk assessment tools upon patient entry into the operating room. After the surgery, the researchers completed a postoperative evaluation based on the actual procedure and examined the skin condition at the compression site. The patients were categorized into the IAPI group if they presented with erythema or more severe PIs at the compression site, and patients with no skin damage were categorized into the non-IAPI group. Based on the scores obtained from the different risk assessment scales before, during, and after the operation, the patients were divided into the low-risk group and the medium- to high-risk group. Regardless of their risk of developing IAPI, the patients’ body position and skin protection were managed according to the operating room nursing guide, while preventive measures were implemented to manage any potential IAPIs. All patient details have been de-identified. The reporting of this study conforms to the STROBE guidelines. 18
Instruments
Four scales were used to measure the risk of PI in this study: the Braden scale, Munro Pressure Injury Risk Assessment Scale, Scott Triggers tool, and CORN Intraoperative Acquired Pressure Injury Risk Assessment Scale.
The Braden scale consists of six assessment categories: sensory perception, mobility, nutrition status, activity level, moisture exposure, and friction/shear force. Patients receive a score of 6 to 23, with lower scores indicating a higher risk of developing PI. A cutoff score of 16 is used to categorize patients into two risk groups. A score of ≤16 indicates a significant risk for PI development, while a score of ≥17 indicates a lower risk. 17
The Munro scale is used to assess patients during the preoperative, intraoperative, and postoperative phases, and it contains a summary section that calculates the total score based on the variables assessed. 19 The risk factor assessment and scores are cumulative, with each assessment phase yielding a low-, medium-, or high-risk score. The total perioperative risk score is obtained by adding up the scores from each assessment phase. The preoperative risk assessment includes six factors: mobility, preoperative fasting, BMI, history of weight loss, age, and comorbidities. Each variable is assigned a score of 1, 2, or 3 with corresponding cutoffs and reference intervals. The total score determines the risk level, which is classified as low (score of 5 or 6), moderate (score of 7 to 14), or high (score of ≥15). The intraoperative assessment includes the physical status/ASA score, anesthesia type, changes in body temperature, episodes of hypotension, skin moisture levels, surface/motion variables, and patient position, with each variable receiving a score of 1, 2, or 3. The sum of the intraoperative scores (ranging from 7 to 21) is added to the preoperative score, resulting in a low (score of 13), moderate (score of 14 to 24), or high (score of ≥25) risk classification. The postoperative assessment includes the perioperative duration and blood loss, which are scored using a 3-point descriptive rating scale. The sum of both postoperative and intraoperative scores yields the total Munro risk score, grouped as low (score of 15), moderate (score of 16 to 28), or high (score of ≥29). 20
Finally, the Scott Triggers tool uses four items: age of ≥62 years, serum albumin level of <3.5 g/dL, ASA score of ≥3, and surgery time of >3 hours. These items predict the risk of developing IAPI in surgical patients, with a score of ≥2 indicating high risk.
The CORN risk factor assessment scale for IAPI includes 2 dimensions, 12 risk factors, and 37 items. The two dimensions are a preoperative PI risk factor assessment and dynamic intraoperative PI risk factor assessment. The 12 risk factors are the anesthesia grade, body mass index (BMI), compression site, skin status, preoperative physical activity, estimated operation time, diabetes mellitus, decrease in body temperature, operative blood loss, intraoperative pressure, shear force change, and operation time. Patients with preoperative evaluation scores of >14 were classified as high-risk, those with scores of 9 to 14 were classified as medium-risk, and those with scores of <9 were classified as low-risk. Patients with intraoperative evaluation scores of >12 were classified as high-risk, those with scores of 8 to 12 were classified as medium-risk, and those with scores of <8 were classified as low-risk.
Statistical methods
The data were analyzed using SPSS 22.0 software (IBM Corp., Armonk, NY, USA). The chi‐square test, Fisher’s exact probability method, and t-tests were used to compare the basic characteristics and risk scores of the 100 patients between the IAPI and non-IAPI groups. The predictive performance of each assessment tool was measured using the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and area under the receiver operating characteristic (ROC) curve (AUC). Sensitivity refers to the probability of the model classifying a patient as at risk of IAPI development given that they have IAPI. Specificity represents the probability of the model classifying a patient as not at risk of IAPI development given that they do not have IAPI. The PPV is the proportion of patients classified at risk who actually develop IAPI, while the NPV is the proportion of patients classified as not at risk who do not have IAPI. The ROC curve illustrates the trade-off between sensitivity and specificity for various test scores. Sensitivity is plotted on the vertical axis against (1 − specificity) on the horizontal axis over a range of potential cut-off scores. The AUC is a measure of how well the model can differentiate between the two groups. 21 A P-value of <0.05 was considered statistically significant.
Ethical principles
This study was reviewed and approved by the Institutional Review Board of Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine (IRB No. 2021-410). Informed consent forms were signed by either the patients or their legal guardian. Verbal informed consent was obtained from the patients.
Results
This study involved 100 patients who underwent elective surgery at the study site from November 2021 to September 2022, including 61 (61%) men and 39 (39%) women. The patients’ mean age was 62.19 ± 12.21 years, and their mean operation time was 244.60 ± 73.12 minutes. Sixty-four (64%) patients underwent cardiovascular surgery, 22 (22%) underwent pancreatic surgery, and 14 (14%) underwent gastrointestinal surgery.
Of the 100 patients, 37 (37%) developed class I/stage PI (erythema) after surgery. Among these 37 patients, the erythema in 32 (86.49%) resolved within 2 hours after surgery, whereas that in 5 (15.63%) progressed to class II/stage or higher PI within 6 days after surgery. The patients were subsequently divided into two groups, the IAPI group (37 patients) and the non-IAPI group (63 patients), based on the presence or absence of erythema. Table 1 presents a comparison of the general characteristics between the two groups, revealing no differences in age, weight, BMI, or sex. However, patients with IAPI had significantly longer operation times than those without IAPI (P < 0.05).
Baseline characteristics of patients with and without IAPI.
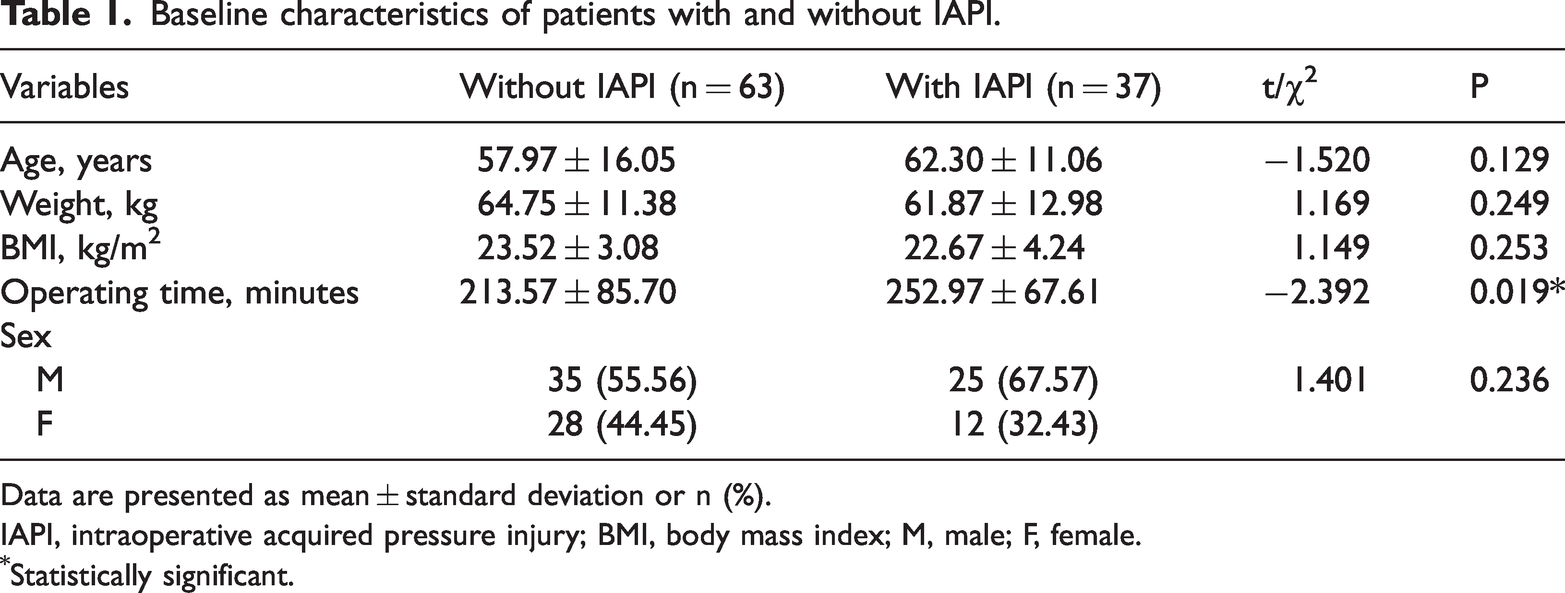
Data are presented as mean ± standard deviation or n (%).
IAPI, intraoperative acquired pressure injury; BMI, body mass index; M, male; F, female.
Statistically significant.
The four above-described risk assessment scales were used to assess the perioperative risk of PI, and the scores were compared between the IAPI and non-IAPI groups. The intraoperative Braden score showed no significant differences between the two groups. However, the mean scores of the other three risk assessment scales were significantly different between the groups (P < 0.01). These findings are shown in Table 2.
Comparison of perioperative risk assessment scale scores in patients with and without IAPI.

Data are presented as mean ± standard deviation.
IAPI, intraoperative acquired pressure injury.
Statistically significant.
We also compared the incidence of IAPI among various groups using the scores obtained from the four distinct risk assessment tools. The patients were categorized into either a no-risk group or high-risk group based on the results of their Braden scale assessments before and after their procedures. The rates of IAPI in each group were examined and compared, and no significant differences were found between the two. Details are shown in Table 3.
Comparison of incidence of IAPI in different groups with preoperative and intraoperative Braden score.

Data are presented as n (%).
IAPI, intraoperative acquired pressure injury.
The patients were divided into low-risk and medium- to high-risk groups based on their CORN perioperative risk assessment scale results before and after their operations. A statistical analysis was performed to evaluate the incidence of IAPI in each group, and the results showed significant differences between the two groups (P < 0.01). Details are shown in Table 4.
Comparison of incidence of IAPI in different groups with preoperative and intraoperative CORN score.

Data are presented as n (%).
IAPI, intraoperative acquired pressure injury,
Statistically significant.
Based on the results of the Scott Triggers risk assessment scale, the patients were categorized into either the no-risk group or the risk group. A statistically significant difference was found in the incidence of IAPI between the groups (P < 0.01). Details are provided in Table 5.
Comparison of incidence of IAPI in different groups with Scott Triggers scores.

Data are presented as n (%).
IAPI, intraoperative acquired pressure injury.
Statistically significant.
The Munro perioperative risk assessment scale was used to categorize the patients into low-risk and medium- to high-risk groups before, during, and after their operations. A comparison of the IAPI incidence between these groups was then conducted. We found no significant differences between the two groups either during or before the operation. After the operation, however, the incidence of IAPI differed significantly between the two groups (P < 0.01). Further details are provided in Table 6.
Comparison of incidence of IAPI in different groups of patients with Munro perioperative risk assessment scale scores.

Data are presented as n (%).
IAPI, intraoperative acquired pressure injury.
Statistically significant.
We established the occurrence of IAPI as the standard for diagnosis and used this measure to compare the efficacy of the four different assessment tools for predicting the IAPI risk. Our analysis was based on a range of measures, including sensitivity, specificity, PPV, NPV, and AUC. Based on these criteria, the Munro postoperative score produced the highest AUC, rendering it the most effective of the four tools evaluated in predicting the incidence of IAPI. The results are presented in detail in Table 7 and Figure 1. The Hosmer–Lemeshow test was used to assess the goodness of fit of the four assessment tools. The observed and predicted incidences were compared by the chi-square (χ2) goodness-of-fit test for calibration power. The results are presented in detail in Table 8.
Application effect of different assessment tools in IAPI risk prediction.

PPV, positive predictive value; NPV, negative predictive value; AUC, area under the receiver operating characteristic curve; IAPI, intraoperative acquired pressure injury.

Receiver operating characteristic curve comparison of different assessment tools for prediction of intraoperative acquired pressure injury.
Model calibration test results for the four tools.

Results analysis
The use of perioperative risk assessment is critical to effectively reduce the incidence of IAPI. In this study, we compared four commonly used risk assessment tools and categorized patients by IAPI occurrence (including erythema). Our analysis compared the risk scores and IAPI incidence of the four different assessment tools in the two groups of patients. The Braden scale was the only tool used to predict the risk of IAPI during surgery, and there was no significant difference between the two groups. Conversely, there were significant differences in the risk assessment scores for the other assessment tools at different time points. These findings suggest that the Braden scale may not be suitable for assessing perioperative stress injuries.
The Braden scale is commonly used in hospitals, nursing homes, communities, and other institutions, and previous research has shown good reliability and validity.22–25 Braden’s conceptual model of stress injury etiology forms the basis of later research in this field. 26 This model introduced the concept of tissue tolerance and identified the joint action of stress and tissue tolerance as the causes of stress injury. 27 PI occurs when the skin is exposed to high levels of stress over an extended period of time, reducing the patients’ range of motion, mobility, and perception and leading to sustained, high levels of stress effects. Reduced tissue tolerance can result in a shorter duration of lower-intensity stress leading to PI, which is affected by internal and external factors. External factors include increased moisture, friction, and shear force, while internal factors include inadequate nutrition, older age, reduced microarterial pressure, or related factors such as mood and smoking (Figure 2).

Conceptual schema for the study of the etiology of pressure sores, accounting for the relative contributions of the duration and intensity of pressure and the tissue tolerance for pressure.
During the operation, the patient’s mobility and perception are impaired by general anesthesia, yielding a score of 0 in the evaluation process. Thus, these items of the Braden scale are not ideal for IAPI risk assessment. However, this finding also explains why surgical patients are at high risk for the development of hospital-acquired stress injuries. While the Braden scale may not prove to be an effective assessment tool in predicting the risk of IAPI, these results are consistent with the findings of other related studies.28,29
Different studies have yielded varying results regarding the efficacy of the four risk assessment tools for assessment of the stress injury risk. The Munro scale has been translated into multiple languages, widely popularized, and applied in recent years. Several studies have shown that the Munro scale is effective for the risk assessment of stress injury in surgical patients.13,20,30 In our study, we used the Munro scale to assess the risk of patients before, during, and after surgery. The results indicated that the evaluation effect of the Munro scale continued to improve with the continuous progress of the surgical process. The AUC of the Munro scale before, during, and after surgery was 0.552, 0.732, and 0.790, respectively. However, the preoperative predictive effect of the Munro scale was inadequate. Early identification of patients at high risk of IAPI before surgery and prompt intervention are crucial in preventing IAPI. Some dressings have proven effective in IAPI prevention in recent years, but their high cost has prevented their widespread use in major medical institutions. Therefore, the development of an accurate preoperative IAPI risk assessment tool is essential, and it could also be used to rationally allocate and utilize limited medical resources, control costs, and reduce the economic burden on patients.
The CORN scale is a relatively authoritative IAPI risk assessment tool in China in recent years, and it is characterized by simpler assessment items, easier data access, and a shorter evaluation time. However, this scale has not been widely popularized, and few studies exist on its application effect. Our study showed that the CORN scale score and the incidence of IAPI were statistically different between the two groups (P < 0.05). However, its AUC was not as ideal as that of the Munro scale, and its sensitivity did not include all patients with IAPI among the high-risk groups screened. The failure of the scale to identify all risk factors, or to inaccurately select cut-off values, may be responsible for these findings.
Among the four assessment tools, the Scott Triggers tool is notable for having the simplest assessment items and is evaluated only before surgery, making it the most convenient and time-efficient option for the operating room nursing staff to master. In our study, its evaluation effect was suboptimal compared with the Munro scale and CORN scale in terms of the AUC, but its preoperative prediction accuracy was better than that of the Munro scale and CORN scale. These results indicate that age, BMI, ASA score, operation time, and nutritional status are key factors for preoperative prediction of IAPI and important critical indicators for risk screening of IAPI. 31 However, the sensitivity of the Scott Triggers tool was only 72.97, and high sensitivity is crucial for accurately identifying all high-risk groups. Although some studies have acknowledged the Scott Triggers tool as the most appropriate IAPI risk assessment tool, further verification of its application effect is necessary.
In addition to the four assessment tools in this study, artificial neural networks 32 and machine learning algorithm models 33 have also been used for risk assessment of IAPI. However, both studies that evaluated these techniques focused on patients undergoing cardiovascular surgery, whereas the four assessment tools in the present study are applicable to all surgical patients. Although the application effects of these two tools are better than those of the four tools compared in this study according to these previous studies,32,33 these two tools are highly specialized and have limitations in clinical promotion, and they are not suitable for the evaluation of all surgical patients. We look forward to applying these two methods to the risk assessment of IAPI in all surgical patients, which may represent the next direction of our follow-up research.
Some studies have also shown that the surgical time 34 and use of perioperative hormones 35 are key factors affecting the occurrence of IAPI. Among the four tools in this study, all except the Braden scale involved analysis of the duration of surgery. However, hormone use did not appear in the evaluation items. This may be a key evaluation factor especially for patients undergoing cardiovascular surgery, and it is an area where existing evaluation tools need to be improved.
Strengths and limitations
This study compared the effectiveness of four risk assessment tools in predicting patients at high risk of IAPI and evaluated the performance of each tool at different time points using ROC curves. This comparison provides important insight for perioperative nursing staff in selecting the most appropriate assessment tool. However, the study has some limitations, including the small sample size and the lack of inclusion of various caregivers and nursing interventions, which may affect the reliability of the results. Further studies should consider these factors and expand the sample size and research institutions to improve the quality of the research.
Conclusions
This study compared the application effects of four risk assessment tools in predicting patients at high risk of IAPI through analysis of the tools’ sensitivity, specificity, and AUC. The results indicate that all assessment tools except the Braden scale can effectively identify individuals at high risk for IAPI. However, each tool has its own strengths and limitations. Moving forward, it will be important to identify more appropriate assessment tools that can accurately screen for high-risk patients and reduce the workload of operating room nurses. This may lead to effective intervention measures and a reduction in the incidence of IAPI.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231207530 - Supplemental material for Comparison of four risk assessment scales in predicting the risk of intraoperative acquired pressure injury in adult surgical patients: a prospective study
Supplemental material, sj-pdf-1-imr-10.1177_03000605231207530 for Comparison of four risk assessment scales in predicting the risk of intraoperative acquired pressure injury in adult surgical patients: a prospective study by Yuan Chen, Wei Wang, QianJian Qian and BeiWen Wu in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231207530 - Supplemental material for Comparison of four risk assessment scales in predicting the risk of intraoperative acquired pressure injury in adult surgical patients: a prospective study
Supplemental material, sj-pdf-2-imr-10.1177_03000605231207530 for Comparison of four risk assessment scales in predicting the risk of intraoperative acquired pressure injury in adult surgical patients: a prospective study by Yuan Chen, Wei Wang, QianJian Qian and BeiWen Wu in Journal of International Medical Research
Footnotes
Acknowledgements
We thank all participants for their contributions to this study.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Funding
This research was supported by the Nursing Research Fund of Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine (RJHK-2022-11).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.