
Abstract
Objective
To develop and confirm an individualized predictive model to ascertain the probability of deep venous thrombosis in patients with acute poisoning after undergoing hemoperfusion.
Methods
Three hundred eleven patients with acute poisoning who were admitted to a hospital in China between October 2017 and February 2019 were included in the development group. Eighty patients with acute poisoning who were admitted between February and May 2019 were included in the validation group. The independent risk factors for deep venous thrombosis were examined. An individualized predictive model was developed using regression coefficients.
Results
The number of catheter indwelling days, having a catheter while being transported, elevated serum homocysteine concentrations, and dyslipidemia were independent risk factors for deep venous thrombosis following hemoperfusion in patients with acute poisoning. The areas under the receiver operating characteristic curve of the development and validation groups were 0.713 and 0.702, respectively, which suggested that the prediction model had good discrimination capacity. The calibration belts of the two groups were ideal.
Conclusions
Our prediction model has a moderate predictive effect for the occurrence of deep venous thrombosis in patients with acute poisoning. In clinical practice, this model could be combined with a common thrombosis risk assessment model.
Introduction
Deep venous thrombosis (DVT) refers to an abnormal coagulation of blood in deep venous blood vessels. This coagulation blocks the lumen and leads to venous reflux disorder, which occurs in the lower extremities. Pulmonary thromboembolism (PE) is a disorder of the pulmonary circulation caused by a thrombus that clots the pulmonary artery or the branches on the right side of the heart. DVT and PE are collectively referred to as venous thromboembolism (VTE) and are different stages of this disease. One in four people worldwide are estimated to die from thromboembolism, making it an internationally leading cause of death.1–2 Therefore, VTE has become a global public health problem.2–3 Additionally, VTE is the third most common cardiovascular disease after ischemic heart disease and stroke.2,4 VTE is also one of the most common complications that occur in major surgical patients and in those with severe medical conditions.
Vascular wall damage, blood flow stasis, and abnormal coagulation have been proposed as the three major factors affecting the development of thrombosis. 5 At present, the most researched populations internationally primarily include patients with orthopedic major surgery, those with tumors, critical patients, and those who are pregnant or in childbirth.6–11 Because these populations are different, the risk factors affecting them are varied. Among patients with acute poisoning, especially paraquat poisoning and other patients with poisoning without specific antidotes, receiving hemoperfusion as early as possible is the most timely and effective treatment available.12–13 However, hemoperfusion requires indwelling of a central venous catheter. A femoral venous catheter is widely used in clinical practice because of its simple operation, ease of application, and relatively low risk. The use of a catheter is important for the rescue and treatment of critically ill patients. However, the incidence of catheter-related infections and thrombosis is relatively high. 14 A femoral venous catheter can cause many complications among patients, including local tissue injury, vascular wall injury, catheter-related bloodstream infections, and catheter-related thrombosis. Patients with acute poisoning are often in a critical condition, and using venipuncture to treat them can cause further damage to their blood vessel walls. In these patients, plasma D-dimer concentrations and coagulation function of the body are changed. Therefore, the patient’s blood enters a state of high coagulation, thereby increasing their risk of developing DVT.
The prevention of DVT is more important than treatment for this condition, and improving the prevention level of DVT is an important step in effectively reducing thrombosis-related events. To achieve effective prevention, accurate assessment of at-risk patients is the necessary first step. In addition to the above-mentioned three risk factors for thrombosis, whether there are other risk factors affecting patients with acute poisoning needs to be investigated. Moreover, the establishment of a risk prediction model could be helpful for more accurate screening for high-risk patients, enable the implementation of early prevention strategies, and reduce the occurrence of DVT in patients with acute poisoning. Therefore, this study aimed to develop a method for the early identification and screening of high-risk patients with DVT in those who are diagnosed with acute poisoning followed by hemoperfusion.
Methods
Patient selection
We retrospectively analyzed the clinical data of patients with acute poisoning who were admitted to our hospital from October 2017 to February 2019. In addition, 80 patients, who were admitted from February to May 2019, were enrolled in the validation cohort, including 55 patients with DVT and 25 without DVT.
The inclusion criteria were patients who had acute poisoning, and those who had undergone temporary femoral venous catheter insertion and hemoperfusion therapy. Patients who were enrolled in this study were continuously included, and treated with a uniform hemoperfusion regimen and heparinization regimen (including the configuration of prefilled fluid and the amount of heparin in tube sealing fluid). The duration of the hemoperfusion was 2 hours each time. The catheter types of femoral venous catheterization were consistent. Basic precautions were taken in all patients during treatment, including no fasting and water restriction (except contraindications), no restriction of movement if the condition permitted, and active or motionless movement of the lower limbs during catheterization. After deep venous catheterization was removed, DVT was determined according to venous ultrasound results of the lower limbs. GE LOGIQ E9 Doppler ultrasound equipment (GE Healthcare, Chicago, IL, USA) was used in a lower limb ultrasound examination, and the results were obtained by the hospital's qualified technicians.
The exclusion criteria were as follows: (1) taking any drugs and poisons (e.g., aspirin, warfarin, and anticoagulant rat poison poisoning) that affect the function of blood coagulation; (2) having any basic diseases (e.g., primary diseases of the blood system and platelet-related diseases) that affect coagulation or the fibrinolytic system; and (3) incomplete medical records.
Ethics statement
This study was approved (approval number: KYLL-2018-163) by the ethics committee of Qilu Hospital of Shandong University. All participants provided informed oral consent to voluntarily participate in this study. We have de-identified all patients’ details, and the clinical data were kept confidential.
Risk factors
General information, including each patient’s age, sex, height, weight, previous medical history, and associated diseases, whether a femoral venous catheter was present while being transported, the number of days of catheter indwelling, and the type of poisoning experienced, was collected. The patients needed to stay in bed during the indwelling of deep venous catheterization. Therefore, the bed time was consistent with the indwelling time of the catheter.
The results of laboratory tests, which measured the prothrombin time, activated partial thrombin time, white blood cell count, red blood cell count, and platelet count, and concentrations of plasma D-dimer, serum homocysteine blood glucose, and blood lipids, were recorded.
Statistical analysis
A descriptive statistical analysis was carried out between the general data and current survey results, including the rate, percentage, mean, and standard deviation. A risk factor analysis was performed using univariate and multivariate logistic regression analyses. The univariate analysis comprised the independent sample t-test, Mann–Whitney U test, and χ2 test. These tests were used to analyze the differences in general demographic data, toxic-related data, femoral venous catheter-related data, and laboratory test results between the thrombus and non-thrombus groups. Variables showing significance in the univariate analysis were also included in the multivariate logistic regression analysis to examine the main predictive factors of lower extremity DVT in patients with acute poisoning.
According to the results of the logistic regression analyses, the variable with the smallest regression coefficient was found. Other variables were then compared with the variable with the smallest regression coefficient to obtain the corresponding multiple (i.e., the weight value of each variable in the model was calculated to establish a high-risk prediction model). The prediction model was evaluated for its discrimination and calibration.15–16 SPSS version 22.0 (IBM Corp, Armonk, NY, USA) was used to draw the receiver operating characteristic (ROC) curves of the prediction model. We used MedCalc software (MedCalc Software Ltd., Ostend, Belgium) to calculate and compare the area under the ROC curve, sensitivity, and specificity of the model to evaluate its differentiation. Additionally, the calibration belt, which was drawn using R software (www.r-project.org), was used to evaluate the calibration of the prediction model.
The reporting of this study conforms to the TRIPOD guidelines.17–18
Results
Patients’ demographics
In this study, 311 patients with acute poisoning were enrolled who were aged 10 to 83 years (34.73 ± 15.93), including 147 men and 164 women. Twenty-one patients had hypertension, eight had diabetes, four had coronary heart disease, and five had cerebrovascular disease (Table 1). Among the 311 patients with acute poisoning, 184 (59.2%) had DVT. Of these 184 patients, 158 had the central type of lower extremity DVT, including total femoral vein thrombosis and iliac vein thrombosis, with 12 cases of intermuscular vein thrombosis of the lower leg. There were also 14 cases of mixed DVT. Most of the patients did not have any obvious symptoms. In 181 of the patients, only 3 showed any obvious symptoms, including 2 with lower limb swelling and pain, and 1 with PE. The thrombosis and non-thrombosis groups showed significant differences in their body mass index (BMI), number of catheter indwelling days, whether they had a femoral venous catheter during transport, plasma D-dimer concentrations, serum homocysteine concentrations, and dyslipidemia (Table 2) (all P < 0.05). However, there were no significant differences in the patients’ age, sex, hemoperfusion time, high-risk diseases, prothrombin time, activated partial thromboplastin time, white blood cell count, red blood cell count, platelet count, or blood glucose concentrations between the two groups (Table 2).
Baseline characteristics of the development group and the validation group.
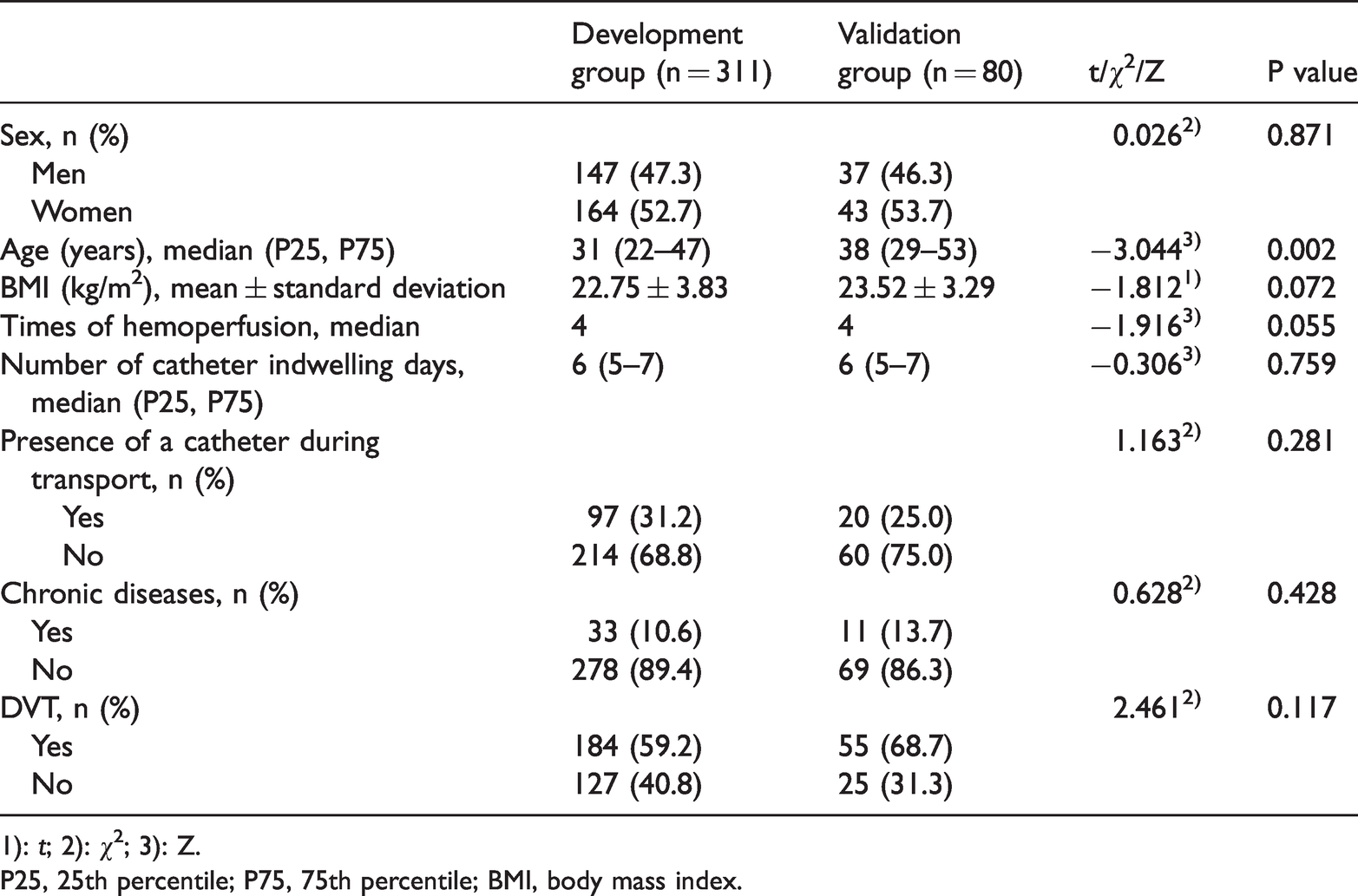
1): t; 2): χ2; 3): Z.
P25, 25th percentile; P75, 75th percentile; BMI, body mass index.
Comparison of the thrombus group and the non-thrombus group.

1): t; 2): χ2; 3): Z.
P25, 25th percentile; P75, 75th percentile; BMI, body mass index; CHD, coronary heart disease; PT, prothrombin time; APTT, activated partial thrombin time; WBC, white blood cell; RBC, red blood cell; PLT, platelet.
Development of the prediction model
Variables that showed significance in the univariate analysis were then analyzed using multivariate logistic regression. We found that the number of catheter indwelling days, having a femoral venous catheter during transport, elevated serum homocysteine concentrations, and dyslipidemia were independent risk factors for DVT following hemoperfusion in patients with acute poisoning (all P < 0.05, Table 3).
Logistic regression analysis of risk factors for DVT following hemoperfusion in patients with acute poisoning.

SE, standard error; OR, odds ratio; CI, confidence interval; BMI body mass index.
According to the results of the multivariate logistic regression analysis, in patients with acute poisoning, the regression coefficients of having a catheter during transport, dyslipidemia, number of catheter indwelling days, and serum homocysteine concentrations were 0.844, 0.682, 0.159, and 0.049, respectively. We used the minimum regression coefficient (0.049) of serum homocysteine as the cardinality to calculate the multiples of the other variables as a weighted value for each risk factor (Table 4).
Description of risk factor assignment.

On the basis of the above-mentioned risk factors, a high-risk scoring model of DVT in patients with acute poisoning was established as follows: Y = 17 × whether patients had a catheter during transport (yes = 1; no = 0) + 14 × whether dyslipidemia is present (yes = 1; no = 0) + 3 × number of catheter indwelling days +serum homocysteine concentrations.
Validation of the prediction model
Area and related parameters under the ROC curve of the prediction model
SPSS version 22.0 (IBM Corp, Armonk, NY, USA) was used to draw the ROC curve of the high-risk prediction model for DVT in patients with acute poisoning and to calculate the area under the ROC curve. We found that the AUC value of this high-risk prediction model was 0.713. Because this value was between 0.7 and 0.9, this indicated that the prediction effect of the model was at a medium level (Figure 1).
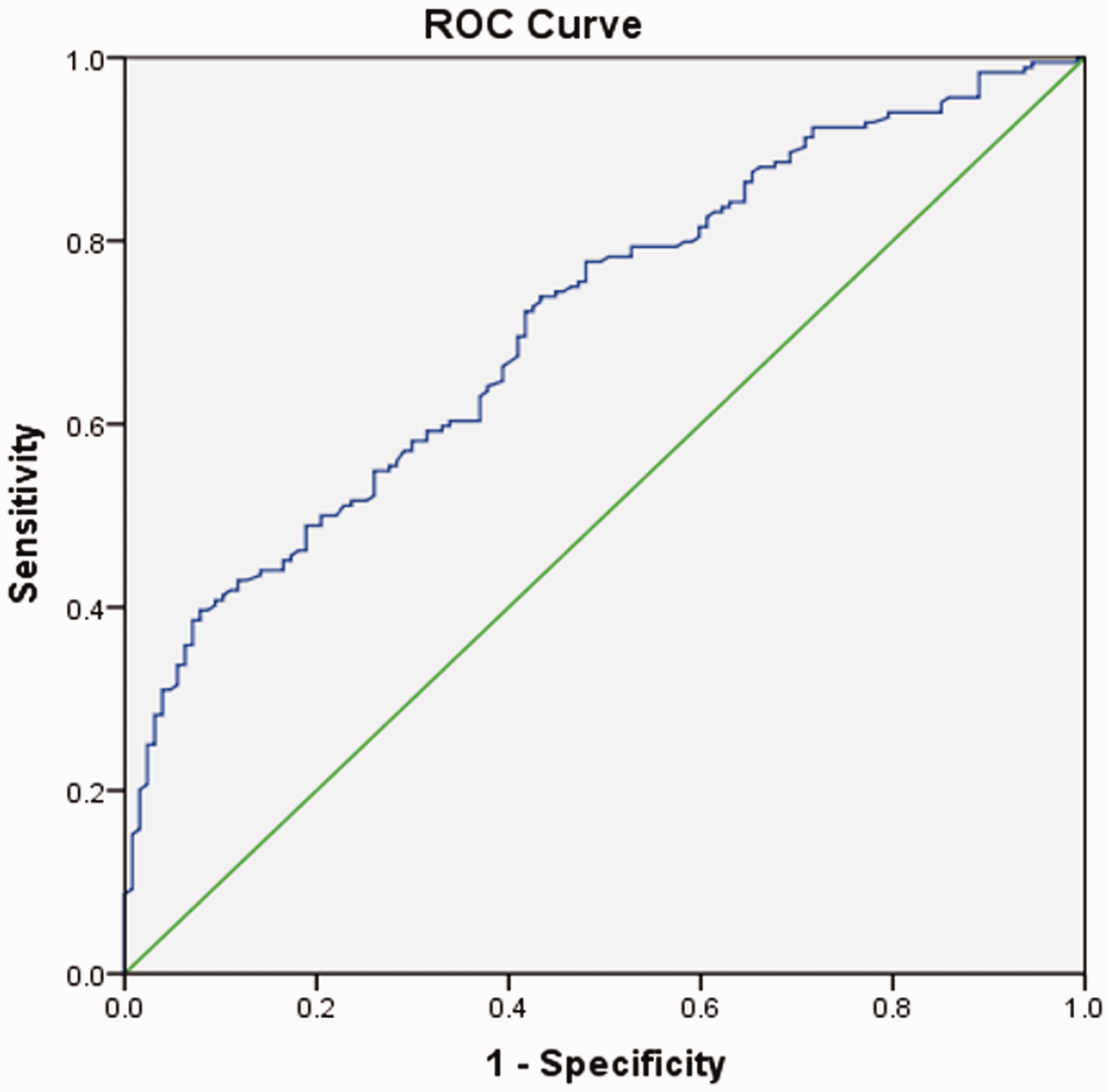
ROC curve of the prediction model.
MedCalc software was used to analyze the ROC curve of the prediction model. The optimal critical value of the model was 58.9, its sensitivity was 39.7%, and its specificity was 92.1% (Table 5).
Optimal critical value and related parameters of the prediction model.

ROC, receiver operating characteristic; CI, confidence interval.
External validation of the prediction model
The prediction model was checked for external validation by analyzing 80 patients with acute poisoning who visited the hospital between February and May 2019. We found that the area under the ROC curve was 0.702 (Figure 2 and Table 6).

ROC curve of the external validation data.
Comparison of external validation data with development of the prediction model.

AUC, area under the curve.
Calibration test of the prediction model in the development and validation groups
The calibration plots of the prediction model in this study suggested that there was strong concordance between the actual probability and predicted probability, and the calibration of this model was perfect in the development and validation groups (Figure 3).

Calibration plots of the prediction model in the development group and the validation group.
Discussion
The symptoms of DVT are insidious and often occur without warning. Once a patient experiences thrombotic symptoms, this indicates that either DVT or PE has occurred, which can be easily misdiagnosed or missed completely. The suddenness and lethality of DVT seriously endanger a patient’s life, affect their overall quality of life, and increase their experienced economic burden. DVT is also an important factor that causes various doctor–patient disputes. Therefore, effective risk assessment and the prevention of DVT are crucial processes that need to be further developed. A national, multicenter, cross-sectional study 19 showed that 36.6% of inpatients in China were at a high risk of VTE. A total of 53.4% of these patients were at a high risk of requiring surgery, while the prevention rates of medical and surgical DVT were 6.0% and 11.8%, respectively. These previous findings indicate that although a large proportion of hospitalized patients are at risk of DVT, prevention of VTE is insufficient. Therefore, medical workers need to have greater awareness and available actions to tackle the growing burden of VTE.
The incidence of DVT was 59.2% following hemoperfusion in patients with acute poisoning in this study. Additionally, most of them experienced asymptomatic DVT. Only 1.6% (n = 3) of the patients had symptoms and one patient developed PE. This finding should be a cause of serious concern among medical personnel. Therefore, the risk assessment and prevention methods in the treatment process of patients with acute poisoning need to be improved. Moreover, venous Doppler ultrasonography of the lower extremities should be regarded as a routine examination following the removal of a femoral venous catheter in patients with acute poisoning. This examination could effectively detect the occurrence of DVT at an early stage, enabling treatment as soon as possible to avoid the occurrence of more serious PE.
In this study, there were significant differences in BMI, whether the patients had a femoral venous catheter during transport, the number of catheter indwelling days, plasma D-dimer concentrations, serum homocysteine concentrations, and dyslipidemia between the thrombosis and non-thrombosis groups. A binary logistic regression analysis showed that the presence of a femoral venous catheter during transport, the number of catheter indwelling days, elevated serum homocysteine concentrations, and dyslipidemia were independent risk factors for DVT after patients with acute poisoning underwent hemoperfusion.
In this study, BMI in the thrombus group was significantly higher than that in the non-thrombus group. A previous study showed that the incidence of DVT was 75.4% in patients with obesity (BMI ≥25 kg/m2) 20 and 54.5% in patients without obesity (BMI <25 kg/m2). Therefore, patients with obesity are more likely to develop DVT than those who are not obese. This finding is consistent with the results of other studies.21,22 High body fat content in patients with obesity can lead to dyslipidaemia, 23 which leads to hypercoagulability 24 in their blood, thus increasing their risk of developing DVT. Therefore, medical personnel need to pay attention to patients with obesity. Furthermore, medical personnel need to consider the effect of this risk factor, be aware of the patients’ hemoperfusion, and the diagnosis and treatment process of anticoagulation standards to improve the implementation of preventive measures and clinical symptom observation.
The incidence of DVT in patients with femoral venous catheters during transport was 2.325 times higher than that in other patients. This is related to the large lumen diameter of the femoral venous catheter in patients. Additionally, the friction between the central venous catheter and the vascular wall increases during the patient’s transport, which further increases the resulting damage to the vascular wall. During transport, the patient is also either in a sitting or lying position for a long time within a narrow space. Therefore, achieving any level of mobility is inconvenient, which in turn means that the patient’s lower limb vein blood flow is slow. During transport, because of the inconvenience of urination, blood viscosity may increase owing to a reduced intake of food and water, resulting in high blood coagulation. Therefore, femoral venous catheters should be avoided in patients who need to undergo transport, especially for those needing to travel long-distances. If transport is unavoidable owing to special circumstances, appropriate preventive measures should be taken, with active fluid replenishment being performed throughout. Furthermore, active and passive activities of the patients’ lower extremities should be facilitated to increase blood reflux within their lower limbs.
This study also showed that the indwelling time of the femoral venous catheter in patients with acute poisoning had a considerable effect on the occurrence of DVT. We found that the number of catheter indwelling days in patients in the thrombosis group was longer than that in those in the non-thrombosis group. With the extension of the indwelling time of the femoral venous catheter, the incidence of DVT increased. Therefore, following the cessation of the hemoperfusion protocol, the duration of the femoral venous catheter should be shortened as much as possible to reduce the incidence of DVT, while still ensuring that it achieves its therapeutic purpose.
Among the relevant laboratory test indicators, elevated serum homocysteine concentrations and dyslipidemia were important predictive factors for DVT following hemoperfusion in patients with acute poisoning. The normal range of serum homocysteine concentrations is <15 µmol/L. Elevated serum homocysteine concentrations potentially disrupt the balance between the coagulation and anticoagulation mechanisms in the human body, forcing the blood into a hypercoagulable state. Previous studies 25 have also shown that elevated serum homocysteine concentrations are a risk factor for DVT. In a meta-analysis, 26 serum homocysteine concentrations were significantly higher in patients with cerebrovascular disease than in controls. In this study, the incidence of DVT in patients with dyslipidemia was 1.978 times higher than that in those with a normal lipid profile. Therefore, these two indices should be observed and evaluated in the treatment of patients with acute poisoning, with appropriate intervention measures being implemented as soon as possible to reduce the patient’s serum homocysteine concentrations and actively control their blood lipids.
In this study, independent risk factors in a logistic regression analysis were used to establish a high-risk prediction model of DVT in patients with acute poisoning. The area under the ROC curve was 0.713. The accuracy of this model in predicting DVT in patients with acute poisoning was at a medium level. Additionally, the optimal critical value of the prediction model was 58.9. When the score of patients using the prediction model was >58.9, the likelihood of an incidence of DVT was predicted to be 71.3%. Furthermore, the sensitivity, specificity, and Youden index of the model were 39.7%, 92.1%, and 0.318, respectively. In summary, in clinical nursing work, this study’s prediction model may be combined with the scoring results of a commonly used risk assessment model. This combination could be used to comprehensively evaluate the risk of DVT development in patients with acute poisoning and accurately and effectively screen for those who have a high risk. Basic preventive measures should be taken for low-risk patients, while physical and drug prevention should be undertaken for those who have a high risk of DVT. The risk factors screened in this study should also be actively avoided or reduced.
Limitations
There are some limitations to this study. We only investigated patients with acute poisoning in a single center. Therefore, the sample size was limited. In our follow-up research, we will expand our sample size and the observation indices to conduct a more in-depth assessment and validation of this prediction model. Additionally, the sensitivity of the prediction model established in this study was 39.7%, which is low. Therefore, in clinical work, the routine application of the Caprini thrombosis risk assessment model is required to assess the risk of thrombosis in patients and to implement prevention strategies at an early stage.
Conclusion
In this study, we established an individualized prediction model for the occurrence of DVT in patients with acute poisoning, and it had an accuracy at a medium level. In practical work, this prediction model may be combined with a commonly used thrombosis risk assessment model to comprehensively evaluate the risk of DVT occurring in patients with acute poisoning. Corresponding preventive measures can then be implemented.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221089779 - Supplemental material for Development and validation of a prediction model of deep venous thrombosis for patients with acute poisoning following hemoperfusion: a retrospective analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605221089779 for Development and validation of a prediction model of deep venous thrombosis for patients with acute poisoning following hemoperfusion: a retrospective analysis by Xiuqin Li, Jing Liu, Siqi Cui, Tianzi Jian, Shuang Ma, Longke Shi, Ying Lin, Juan Zhang, Yingying Zheng, Yanxia Zhang, Xiangdong Jian, Xiaorong Luan and Baotian Kan in Journal of International Medical Research
Footnotes
Author contributions
Conception and design: XL, SM, XL, and BK
Analysis and interpretation: XL and SM
Data collection: XL, YL, JZ, YZ, CL, and YZ
Writing the article: XL and SM
Critical revision of the article: XL, BK, and XJ
Final approval of the article: XL, BK, and XJ
Statistical analysis: XL and SM
Overall responsibility: BK, XL, and XJ.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.