
Abstract
Objective
We performed a systematic review to analyze the benefits of and risk factors associated with granulocyte colony stimulating factor (GCSF) in patients with liver cirrhosis.
Methods
PubMed, Scopus, and Embase were searched for randomized controlled trials and case–control studies that compared the use of GCSF with another treatment or control group. The Jadad and Newcastle–Ottawa scales were used to assess the risk of bias in the included studies. The primary outcome studied was mortality; and the secondary outcomes were the disease severity score, liver transplantation criteria, complications, CD34+ cell count, adverse events, and health-related quality of life (HRQOL). PROSPERO registration number CRD42023416014.
Results
The initial search yielded 2,235 studies, of which seven studies of 670 patients with liver cirrhosis were included. Multiple cycles of GCSF significantly improved the survival rate, disease severity score, CD34+ cell count, and HRQOL; and significantly reduced the incidences of liver transplantation, ascites, infection, and hepatic encephalopathy. Fatigue and backache were the most commonly reported adverse events.
Conclusion
GCSF significantly improves the survival rate and disease severity scores, and reduces the incidence of complications in patients with liver cirrhosis. The administration of GCSF is likely to be effective in patients awaiting liver transplantation.
Keywords
Introduction
Liver cirrhosis is a leading cause of morbidity globally. Cirrhosis is defined as the development of nodules, surrounded by fibrous bands, in response to repetitive chronic liver injury, and it ultimately leads to portal hypertension and end-stage liver disease.1,2 In addition, cirrhosis of the liver is associated with a higher risk of liver cancer. 3 Liver transplantation is currently the definitive treatment for liver cirrhosis. However, recent advances in the management of liver cirrhosis have improved treatment outcomes and health-related quality of life (HRQOL). 4 A few recent studies have shown that bone marrow-derived cells, including multipotent stem cells, are capable of self-renewal and differentiation into various adult cell types, including hepatocytes.5–7 In addition, one study has demonstrated a positive effect of bone marrow cells in vitro in models of acute and chronic liver damage, and that they can populate the liver and contribute to hepatic regeneration. 8 Granulocyte colony stimulating factor (GCSF) administration has been shown to be an effective, well-tolerated, and non-invasive means of mobilizing bone marrow cells.9,10 Most human tissues can secrete GCSF in response to stimulation by interleukin-1, lipopolysaccharide, or tumor necrosis factor-alpha, which are produced by macrophages, endothelial cells, fibroblasts, and other mesenchymal cells.11–13 GCSF receptor is expressed by neutrophils and their precursors, and signals through the janus kinase-signal transducer and activator of transcription pathway or through the phosphorylation of Lyn, activating the phosphoinositol 3-kinase/AKT pathway, which is involved in the development of liver fibrosis. GCSF also plays a role through the activation of the Ras-mitogen-activated protein kinase (MAPK) pathway via the tyrosine kinases Lyn and Hck.14,15
The Ras-MAPK pathway has been implicated in the development and progression of hepatocellular carcinoma in patients with liver cirrhosis.16,17 Ordelheide et al. reported that GCSF promotes free fatty acid-induced insulin resistance; and patients with liver cirrhosis who have co-morbidities such as obesity, metabolic syndrome, and insulin resistance, and are being administered GCSF, are at higher risk of disease progression. 18 Furthermore, Stroncel et al. reported a mean 20% increase in splenic size in patients administered GCSF at 10 μg/kg/day for 5 days. 19 Larger spleens receive greater blood flow, which is associated with portal hypertension, a condition that can cause the progression of liver cirrhosis-related complications. The effects of GCSF to improve liver function and ameliorate fibrosis have been identified through the study of CD34+ bone marrow-derived cell mobilization. Recent studies have shown beneficial effects of the administration of GCSF to patients with acute-on-chronic liver failure (ACLF) 20 or alcoholic hepatitis. 21 However, studies regarding the effects of GCSF when administered to patients with liver cirrhosis, with respect to safety profile, quality of life, long-term outcomes, and the optimal dose and duration of administration, have been few in number to date. Therefore, in the present study, we aimed to evaluate the effects of GCSF in patients with liver cirrhosis by conducting a systematic review of randomized controlled trials and case–control studies of the use of this substance.
Because the study was a systematic review, the requirements for ethics approval and the informed consent of the participants were waived.
Methods
Literature search
An extensive literature search was performed using PubMed, Scopus, and Embase. In the first phase of the search, we used “granulocyte-colony stimulating factor”, “GCSF”, “G-CSF”, “lenograstim”, “filgrastim”, “pegfilgrastim”, and “lipegfilgrastim” as search terms; and in the second phase we used “liver cirrhosis”, “decompensated cirrhosis”, and “cirrhosis”. The results of the first and second search phases were combined, and citations were imported into Zotero v.5.0 (Corporation for Digital Scholarship, Vienna, VA, USA). Two authors (SR and PBM) independently screened the eligible studies, and a third author (BM) helped settle any disagreement regarding the application of the inclusion and exclusion criteria (Figure 1).

Preferred reporting items for systematic reviews and meta-analyses flow diagram.
Inclusion and exclusion criteria
We selected all the randomized controlled trials and case–control studies conducted between May 2013 and August 2022 that concerned liver cirrhosis and GCSF and involved a comparison with standard medical therapy and/or placebo. The primary outcome was mortality or survival rate; and the secondary outcomes of the changes in the model for end-stage liver disease (MELD)/MELD-Na and Child–Turcotte–Pugh (CTP) scores, the improvement in liver cirrhosis and related complications, hospitalization, spontaneous bacterial peritonitis, variceal hemorrhage, the requirement for liver transplantation, adverse events, and quality of life. Only publications in English were considered; and review articles, case reports, case series, editorials, and studies with insufficient or incomplete data were excluded. In cases of duplicate publication, the data from the most recent publication were included.
Data extraction
Two authors (SR and PBM) independently assessed the eligible studies for the following information: (i) study description, including author name, year of publication, study location, target population, study design and size, treatment used, and the nature of the control group; (ii) liver cirrhosis-related findings, including CTP score, MELD or MELD-Na score, ascites, spontaneous bacterial peritonitis, sepsis, acute kidney injury, variceal hemorrhage, hepatic encephalopathy, mortality or survival rate, liver function, the requirement for liver transplantation, HRQOL, and adverse events.
Quality assessment
Two independent reviewers (SR and PBM) evaluated the risk of bias associated with, and the quality of, each study using the Newcastle–Ottawa Scale (NOS) 22 and Jadad 23 scales. The NOS is used to evaluate the selection of cases and controls, their comparability, and outcome assessments. The Jadad score consists of three parameters: randomization, masking, and the accounting for all the participants, including withdrawals. The first five questions were scored as one each if the answer is yes, and minus one if the method of randomization or blinding was inappropriate. The overall score varies from 0 (very poor) to 5 (rigorous).
Data synthesis and analysis
We tabulated the results or outcomes from each study in detail to more readily identify patterns within the data. We performed a narrative data synthesis because we considered that the data were unsuitable for a formal quantitative meta-analysis owing to the considerable variation in study design, reported outcomes, and outcome metrics. The study was performed according to the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines. 24
Registration
We did not prospectively register this trial, but it was registered retrospectively with PROSPERO, with registration number CRD42023416014.
Results
Search results and included studies
The initial search yielded 2235 records (PubMed, 646; Scopus, 686; and Embase, 929). After screening of the titles and for duplicates, 583 records were analyzed, of which 572 did not meet the inclusion criteria. Of the remaining 11, 4 more studies were excluded because two were review articles and two were original studies comparing the use of a GCSF-erythropoietin combination with placebo. The remaining seven studies met the inclusion criteria and were included in the systematic review (Figure 1).
Study characteristics
Of the seven selected studies,25–31 five were randomized controlled trials25,28–31 and two were case–control studies26,27 with a control group. Five studies were conducted in India,25,26,28–30 one in Italy, 27 and one in the UK. 31 All the included studies involved the administration of GCSF to the treatment group and the use of standard medical therapy in both the treatment and control groups. Newsome et al. 30 and Verma et al. 31 presented additional data regarding the use of a stem cell infusion and growth hormone, respectively. Collectively, the studies presented data for 670 patients with liver cirrhosis (n; = 377 in the treatment group and n; = 293 in the control group). In all the included studies, CTP, MELD, CD34+ cells, liver function, and liver cirrhosis-related complications and adverse events were assessed. In one study, a historical control group was used for patient matching, 25 HRQOL was assessed in two studies,26,29 and the relationship between splenic diameter and CD34+ cell count was assessed in one study 27 (Tables 1 and 2).
Characteristics of the included case–control studies and randomized controlled trials.

ACS, acute coronary syndrome; AKI, acute kidney injury; AVB, acute variceal bleeding; BD, twice a day; CFU-GM, colony-forming unit-granulocyte–macrophage; CTP, Child–Turcotte–Pugh; HE, hepatic encephalopathy; HRQOL, health-related quality of life; HRS, hepatorenal syndrome; ICU, intensive care unit; LSM, liver stiffness measurement; MELD, model for end-stage liver disease; OD, once a day; SBP, spontaneous bacterial peritonitis; SC, subcutaneous; SMT, standard medical therapy, DLC, decompensated liver cirrhosis.
Characteristics of the included randomized controlled trials.
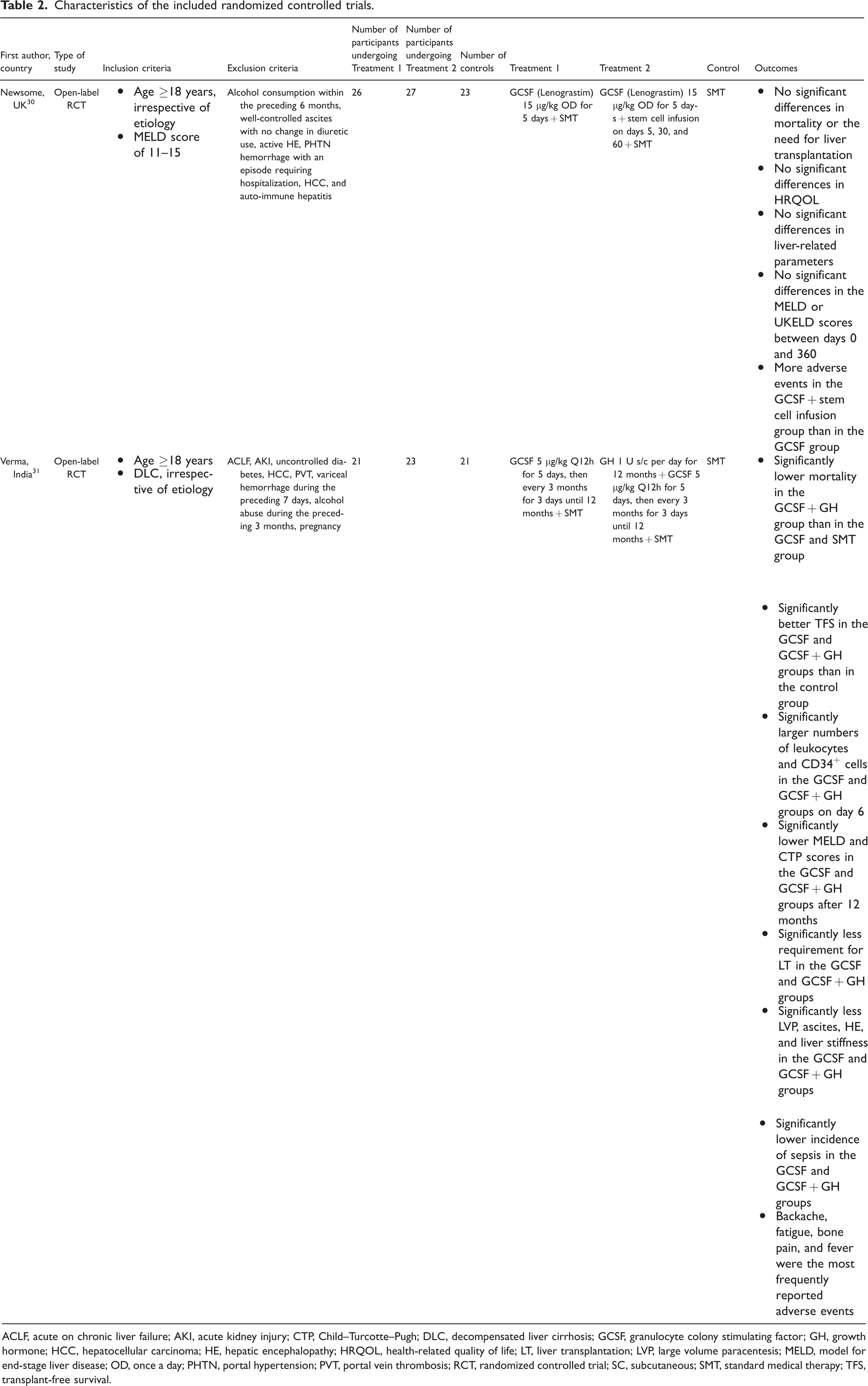
ACLF, acute on chronic liver failure; AKI, acute kidney injury; CTP, Child–Turcotte–Pugh; DLC, decompensated liver cirrhosis; GCSF, granulocyte colony stimulating factor; GH, growth hormone; HCC, hepatocellular carcinoma; HE, hepatic encephalopathy; HRQOL, health-related quality of life; LT, liver transplantation; LVP, large volume paracentesis; MELD, model for end-stage liver disease; OD, once a day; PHTN, portal hypertension; PVT, portal vein thrombosis; RCT, randomized controlled trial; SC, subcutaneous; SMT, standard medical therapy; TFS, transplant-free survival.
Risk of bias and quality assessment
The evaluation method and the inclusion and exclusion criteria were explained prior to the enrolment of the participants in all the included studies. In addition, the same diagnostic tests were performed for both the treatment and control groups over similar periods of time. None of the studies were excluded on the basis of the results of the risk of bias assessment (Table 3).
Results of the quality assessment of the included studies

Outcomes
Mortality
Three of the seven studies25,28,31 showed significantly lower mortality in the GCSF group. However, Philips et al. 26 reported an increase in mortality after 12 months of GCSF treatment, and Newsome et al. 30 reported no difference in mortality between the GCSF and control groups. Venkitaramen et al. 29 reported less mortality in the GCSF group, although the difference from the control group was not significant. De et al., 25 Prajapati et al., 28 and Venkitaraman et al. 29 reported that the majority of their participants died because of sepsis and multi-organ failure (Tables 1 and 2).
Disease severity score
Six of the studies showed improvements in CTP score from baseline.25–29,31 In addition, the MELD score was reported as an outcome in six of the studies,25–27,29–31 three of which25,28,31 showed significant improvements in the MELD score. Gaia et al., 27 Venkitaraman et al., 29 and Newsome et al. 30 reported no change in the MELD score from baseline (Tables 1 and 2).
Liver transplantation
Two of the studies25,31 showed that significantly fewer participants in the GCSF group fulfilled the criteria for liver transplantation (Tables 1 and 2). In addition, Newsome et al. 30 reported a non-significant difference in the requirement for liver transplantation in the GCSF and GCSF-plus-stem cell infusion groups vs. the control group.
Complications
Liver cirrhosis-related complications were reported in four of the studies.25,26,29,31 Significantly less ascites,25,26,29 less frequent infections,25,29 a lower incidence of spontaneous bacterial peritonitis (SBP), 29 a lower incidence of hospitalization, 26 less frequent hepatic encephalopathy,26,31 and less acute kidney injury 26 were reported. However, Philips et al. 26 reported non-significantly higher incidence of acute variceal hemorrhage and significantly higher incidences of acute kidney injury and sepsis after 3 months of treatment (Tables 1 and 2).
Change in CD34+ count
Outcomes related to CD34+ cell count were reported in five studies.25,27–29,31 All five studies showed significantly higher peripheral CD34+ cell count in the treatment group. However, Gaia et al. 27 reported a significant inverse relationship between splenic size and CD34+ cell mobilization. In addition, the authors reported comparable or higher CD34+ cell count in the peritoneal ascitic fluid of the participants on the peak day of mobilization (Tables 1 and 2).
Adverse events
Adverse events were reported in five of the studies,25,27–29,31 but none were severe or life-threatening. Fatigue, bone pain, back pain, nausea, and vomiting were the most commonly reported adverse events (Tables 1 and 2).
Health-related quality of life
HRQOL was reported in two of the studies. De et al. 25 and Venkitaraman et al. 29 reported significantly and non-significantly higher HRQOL, respectively, in the treatment group (Table 1).
Discussion
Liver cirrhosis progresses through several clinical phases, and culminates in death or liver transplantation. The effects of GCSF in patients with liver cirrhosis have varied in previous studies. Therefore, we performed a systematic review and quantitative analysis of five randomized controlled trials and two case–control studies to better understand its effects. These studies were published between 2013 and 2022, and included a total of 377 participants who received GCSF therapy.
Most importantly, we noted a positive effect of GCSF on the survival of patients with liver cirrhosis. In addition, the included studies showed superior CTP scores, but no significant difference in the MELD scores, in the participants in the GCSF group. The movement of bone marrow cells to the liver is the most likely mechanism for GCSF-induced liver regeneration. Consistent with this, the meta-analysis conducted by Marot et al. 21 showed that the use of GCSF is associated with a reduction in mortality of > 70% after 3 months in patients with acute hepatitis vs. controls. However, we cannot be certain whether this survival benefit may be the result of a non-significant reduction in mortality rate, and the precise mechanism whereby GCSF has clinical benefits remains unclear.
The mode of action of GCSF may involve the direct stimulation of liver regeneration by hepatic progenitor cell proliferation or an increase the mobilization of bone marrow stem cells (CD34+), which differentiate and proliferate into mature hepatocytes.32,33 The success of the treatment can be attributed to an improvement in immune cell function and fewer infectious complications, as well as the larger numbers of CD34+ stem cells in the liver, which may facilitate its recovery from injury. A comparable improvement in survival was shown in further studies of patients with acute alcoholic hepatitis or decompensated cirrhosis who were treated with GCSF. 34 In the present review, we found that the administration of GCSF significantly increased the CD34+ stem cell count, which is noteworthy, because studies that have demonstrated the mobilization of CD34+ showed superior outcomes. Similar results regarding CD34+ cells have been obtained in four previous studies of patients with ACLF 6 days following GCSF administration, compared with controls.25,35–37
There were no notable findings regarding liver transplantation-related outcomes in GCSF-treated patients in the present review. However, we also investigated whether there is a relationship between GCSF administration and the complications related to liver cirrhosis. Previously, significant improvements in ascites,25,26,29 infection,25,29 SBP, 29 hospitalization, 26 hepatic encephalopathy,26,31 and acute kidney injury 26 have been identified in GCSF-treated patients. There is evidence that the stimulation of CD34+ cells following their mobilization by GCSF treatment ameliorates the features of cirrhosis: it reduces the volume of ascites fluid and improves albumin and bilirubin synthesis. 38 A meta-analysis conducted by Huang et al. 39 showed that there are lower incidences of hepatic encephalopathy, sepsis, and hepatorenal syndrome in GCSF-treated patients. The prevalence of infection in patients that were treated with GCSF or not was 25% and 32%, respectively.
Regarding adverse events, in the present review, we identified such events in the GCSF group, but none were categorized as being severe or life-threatening. The most commonly reported adverse events were fatigue, bone pain, back pain, nausea, and vomiting, as documented in Tables 1 and 2. In a multi-center randomized trial (the GRAFT study) conducted by Engelmann et al., 20 adverse events were also recorded in the GCSF group, and the systematic review and meta-analysis by Chavez-Tapia et al. 40 documented mild adverse effects, such as fever, rash, herpes zoster infection, headache, and nausea.
The quantification of HRQOL is essential as part of the assessment of the status of patients with liver cirrhosis, but in only two of the included studies25,29 the values of this metric were compared between the groups.
We have revealed superior outcomes relating to certain aspects of cirrhosis in patients treated with GCSF, but it is important to note that the magnitude of the differences may not be particularly biologically significant. Therefore, its overall impact on patients with liver cirrhosis may not be substantial. However, to optimize the therapeutic and safety profile, more high-quality research is necessary to better characterize the role of GCSF in liver cirrhosis therapy.
We acknowledge that the present review has several limitations. First, only seven studies were included, the majority of which generated heterogeneous data and lacked qualitative and quantitative results. Second, five of the studies showed promising results of using GCSF in patients with liver cirrhosis, which introduces social desirability bias into the present study. Finally, the number of participants enrolled and analyzed in the studies differed, which weakens the reliability of the findings.
In conclusion, the role of GCSF in the treatment of liver cirrhosis remains controversial. However, it may be useful in patients with liver cirrhosis who are awaiting liver transplantation. The majority of the studies of its use have shown significantly lower mortality and liver cirrhosis-related complications, but because most lacked sufficient quantitative and qualitative data, we recommend that further randomized controlled trials are performed to assess the effects of GCSF in patients with liver cirrhosis more comprehensively.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231207064 - Supplemental material for Role of granulocyte colony stimulating factor in the treatment of cirrhosis of liver: a systematic review
Supplemental material, sj-pdf-1-imr-10.1177_03000605231207064 for Role of granulocyte colony stimulating factor in the treatment of cirrhosis of liver: a systematic review by Siddheesh Rajpurohit, Balaji Musunuri, Pooja Basthi Mohan, Ganesh Bhat and Shiran Shetty in Journal of International Medical Research
Footnotes
Author contributions
SR: Conceptualization, methodology, resources, writing - original draft, writing - review and editing.
BM: Conceptualization, writing - review and editing, supervision.
PBM: writing - original draft, writing - review and editing.
GB: writing - review and editing, supervision.
SS: writing - review and editing, supervision.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.