
Abstract
Objective
To compare the effects on feto-maternal outcomes of expectant versus active management for premature rupture of membranes (PROM) at term.
Methods
This was a prospective randomized (1:1) controlled study involving 86 pregnant-women who received either expectant management (n = 43) or active management with misoprostol (n = 43) for PROM at term. Primary outcome was route of delivery. Secondary outcomes were: PROM to presentation interval; latency period; PROM to delivery interval; recruitment to delivery interval; labour and delivery complications.
Results
Baseline-characteristics were similar between groups. There was no significant difference between active and expectant groups in mean PROM to presentation/admission, or PROM to delivery. However, mean latency period (11.1 ± 7.3 hours vs 8.8 ± 5.5 hours) and mean recruitment to delivery intervals after PROM (14.7 ± 5.2 hours vs 11.8 ± 5.0 hours) were significantly shorter for the active group compared with the expectant group. Although the rate of caesarean section was less in expectant management group (21%) compared with the active management group (30%), the difference was not statistically significant. There were no significant differences between groups in delivery or perinatal complications.
Conclusion
Active and expectant management for PROM at term gave comparable outcomes in terms of methods of delivery and complications. However, active management significantly shortened the latency period and induction to delivery intervals compared with expectant management.
Keywords
Introduction
Premature, or prelabour, rupture of the foetal membranes (PROM) is defined as rupture of the integrity of the foetal membranes before onset of labour resulting in leakage of amniotic fluid.1,2 PROM can affect both term and pre-term gestations. 2
Multiple pathophysiological processes are involved in the events happening before the onset of parturition. 3 For example, uterine overdistention, neutrophil infiltration and alterations in the contents and composition of the matrix substances of the cervix and foetal membranes all contribute to the weakness and eventual rupture of the membranes, as well as initiation of labour at term. 4 Increased amniotic concentration of matrix metalloproteinase-1 (MMP-1) has been found in cases of chorioamnonitis.4,5 Other processes involved in the initiation of membrane rupture at term include, increased DNA variants of genes involved in extracellular matrix metabolism 6 and over expression of vascular endothelial growth factor (VEGF) in foetal membranes. 7 Multiple infections, 8 antepartum haemorrhage, 9 low amniotic fluid concentration of soluble vascular endothelial factor receptor-1 (VEGFR -1), 10 have been reported to be other causes of PROM. In addition, inherited connective tissue disorders such as Ehlers-Danlos syndrome and Marfan syndrome, have been reported to be associated with preterm delivery.11,12 Risk factors for PROM include: history of previous PROM; infection; incompetent cervix; preterm labour; uterine overdistention; trauma; amniocentesis; prior cervical surgery; low socioeconomic status; poor nutrition; labour; connective tissue disorders.13,14
Diagnosis of PROM requires a thorough medical history, physical examination, and selected laboratory tests. Importantly, it is associated with 10–20% false negative results. 15 Ancillary investigations are often used when clinical diagnosis is in doubt; these include, nitrazine paper test and the fern test. False positive results can also occur, and may arise because of blood, semen and/or vaginal discharge contamination. 16 Studies using biochemical agents that are present in high concentration in the amniotic fluid, absent in cervico-vaginal discharge and have low concentration in the body fluids, have found they are useful in the diagnosis of PROM. 17 For example, placental alpha microglobulin-1 (PAMG -1) and insulin-like growth factor binding protein -1 (ILGFBP-1) have high sensitivity and specificity for detection and diagnosis of PROM.16,18
The management of PROM at term remains controversial. The two main management strategies are either, wait for spontaneous onset of labour (expectant) or, induce labour with prostaglandins/oxytocin (active). Many studies, conducted in different parts of the world, have investigated differences in the outcome of these two strategies and have obtained mixed results. For example, a systematic review and meta-analysis of 23 studies involving 8615 women and their babies, achieved inconclusive results because the evidence was of low quality. 19 The aim of this present study was to compare the effects on feto-maternal-outcomes of expectant versus active management (with misoprostol) for PROM at term.
Methods
Study population
Pregnant women with PROM at term who attended Enugu State University of Science and Technology (ESUT) teaching hospital, Parklane, Enugu, Nigeria, from June 2022 to September 2022 were eligible for this prospective, randomized study. Inclusion criteria were as follows: aged 20–34 years; gestational age 37–41 weeks plus 2 days; singleton pregnancy with cephalic presentation; spontaneous PROM confirmed by clinical, laboratory and/or imaging tests; adequate pelvis; cervical dilatation <4 cm; normal cardiotocography (CTG) readings and ultrasound findings. Exclusion criteria were as follows: multiple pregnancy; features of chorioamnionitis; medical or obstetric complications; previous caesarean delivery; meconium-stained liquor; cephalopelvic disproportion; foetal malpresentation; intrauterine foetal death; prolonged PROM; in vitro fertilization pregnancy; multiple vaginal examinations prior to presentation; cervical incompetence.
Study procedures
At presentation in the labour ward, a detailed medical history, general and systemic examination were performed. Diagnosis of PROM was confirmed based on clinical history, speculum examination for evidence of vaginal pooling, and, nitrazine and fern test of vaginal fluid. PROM was confirmed when at least two out of the three parameters (i.e., vaginal pooling, nitrazine, or fern test) were positive. Following diagnosis of PROM at term, the women underwent an ultrasound scan and basal cardiotocography (CTG) to evaluate foetal wellbeing.
All women were given IV antibiotics (1g ceftriaxone every 24 hours), and 500 mg metronidazole every 8 hours until delivery. Maternal vital signs (i.e., pulse rate, temperature, blood pressure), and uterine contractions were monitored. Foetal heart rate, and colour of liquor were carefully observed. Unnecessary vaginal examinations were avoided. Vaginal examinations were only performed if uterine contractions were adequate or, to gauge the progress of labour (maximum three vaginal examinations in 12 hours). Most women were expected to go into spontaneous labour within 24 hours. Women were randomly allocated to Group A (expectant or conservative management) or Group B (active management with induction of labour).
Following endocervical swabbing for microscopy culture and sensitivity, participants in Group A (expectant management) were kept for observation with a sterile vulval pad for 24 hours from the time of PROM to await spontaneous onset of labour whereas, participants in Group B (active management) were induced, with 25 µg misoprostol (PGE1), repeated every 4 hours until labour. Women in Group B who failed to achieve birth within 24-hours of a cumulative dose of 150 μg misoprostol, received IV infusion of oxytocin at doses usually administered for the induction of labour. Patients in Group A who had no uterine contractions or onset of labour after 24 hours, and Bishop score <5, were given sublingual misoprostol as in Group B, or induced with oxytocin. Emergency caesarean sections were performed on obstetric indications as required. All labour and delivery events were documented.
Primary outcome measure was route of delivery. Secondary outcome measures were: PROM to presentation/admission interval; latency period (i.e., interval between rupture of membranes to onset of labour); PROM to delivery interval; recruitment to delivery interval (i.e., time between being recruited into the study at the hospital to delivery of the baby); labour and/or delivery complications (i.e., maternal fever; contractility patterns; augmentation of labour; instrumental delivery; postpartum haemorrhage; endocervical swab growth); foetal and perinatal outcomes (as exemplified by APGAR scores as a measure of presumed perinatal asphyxia); neonatal intensive care unit (NICU) admission; reason for NICU admission
The study adhered to CONSORT guidelines. 20 The study protocol was approved by the ESUT Ethics Review Committee (with approval number; ESUTHP/C-MAC/RA/034/Vol.11/57). Written informed consent was obtained from each participant prior to the study.
Statistical methods
Sample size calculations were based on results from a previous study. 21 Using a mean time of 21.5 (±9.8) hours for expectant management and a minimum detectable desired difference between groups of 6 hours, type I error at 5% and power at 80%, the total sample population for the study was estimated to be 86 (43 in each arm). Randomization was achieved using a computer-generated random number sequence (blocks of four in ratio of 1:1).
Statistical analysis was performed using SPSS software (version 26.0 for Windows®; IBM Corp, Armonk, NY, USA). A P-value <0.05 was considered to indicate statistical significance. Socio-demographic variables were used to categorize the data. Categorical variables were compared using χ2 test and continuous variables were expressed as mean ± SD and differences were analysed using Student's t-test.
Results
Of the 94 women assessed for eligibility, eight were excluded from the study (Figure 1). The remaining 86 women were randomized into the study, 43 women in each of the two groups. Baseline socio demographic and clinical characteristics were similar in both groups. (Table 1). While not statistically significant, by chance, in Group A, more women lived in a rural than an urban location (61% vs 40%) whereas in Group B, more women lived in an urban than a rural location (63% vs 37%).

Flow chart of the participants in the study.
Baseline characteristics.

Data are expressed as, n, n (%) or mean ± standard deviation.
ns, not statistically significant.
Overall, 64 (74%) participants had a vaginal delivery while 22 (26%) had a caesarean section. There was no significant difference between groups in the rate of caesarean section (Table 2). Of the 22 women that had a caesarean delivery, 9 (21%) were in Group A (expectant) and 13 (30%) in Group B (active).
Primary outcome measure (route of delivery).

Data are expressed as, n, or n (%).
ns, not statistically significant.
Mean (±SD) time to presentation/admission after PROM was 9.7 ± 8.6 hours and 6.5 ± 6.0 hours for the expectant and active groups, respectively. More women presented late (≥19 hours) after PROM in the expectant group (23%) than in the active group (7%). However, the difference between groups was not statistically significant (Table 3).
Secondary outcome measures.

Data are expressed as, n, n (%) or mean ± standard deviation.
Interval between rupture of foetal membranes to onset of labour.
Time between being recruited into the study at the hospital to delivery of the baby.
PROM = Premature Rupture of Foetal Membranes; ns, not statistically significant.
While there was no statistically significant difference between groups in the mean (±SD) latency period (i.e., 11.1 ± 7.3 hours and 8.8 ± 5.5 hours, for the expectant and active groups, respectively) analysis of separate time intervals showed that the latency period was statistically significantly shorter for the active group compared with the expectant group (P = 0.020) (Table 3). For example, only 4 (9%) of participants in the active group had not gone into labour after 18 hours after PROM compared with 14 (33%) in the expectant group (Figure 2).
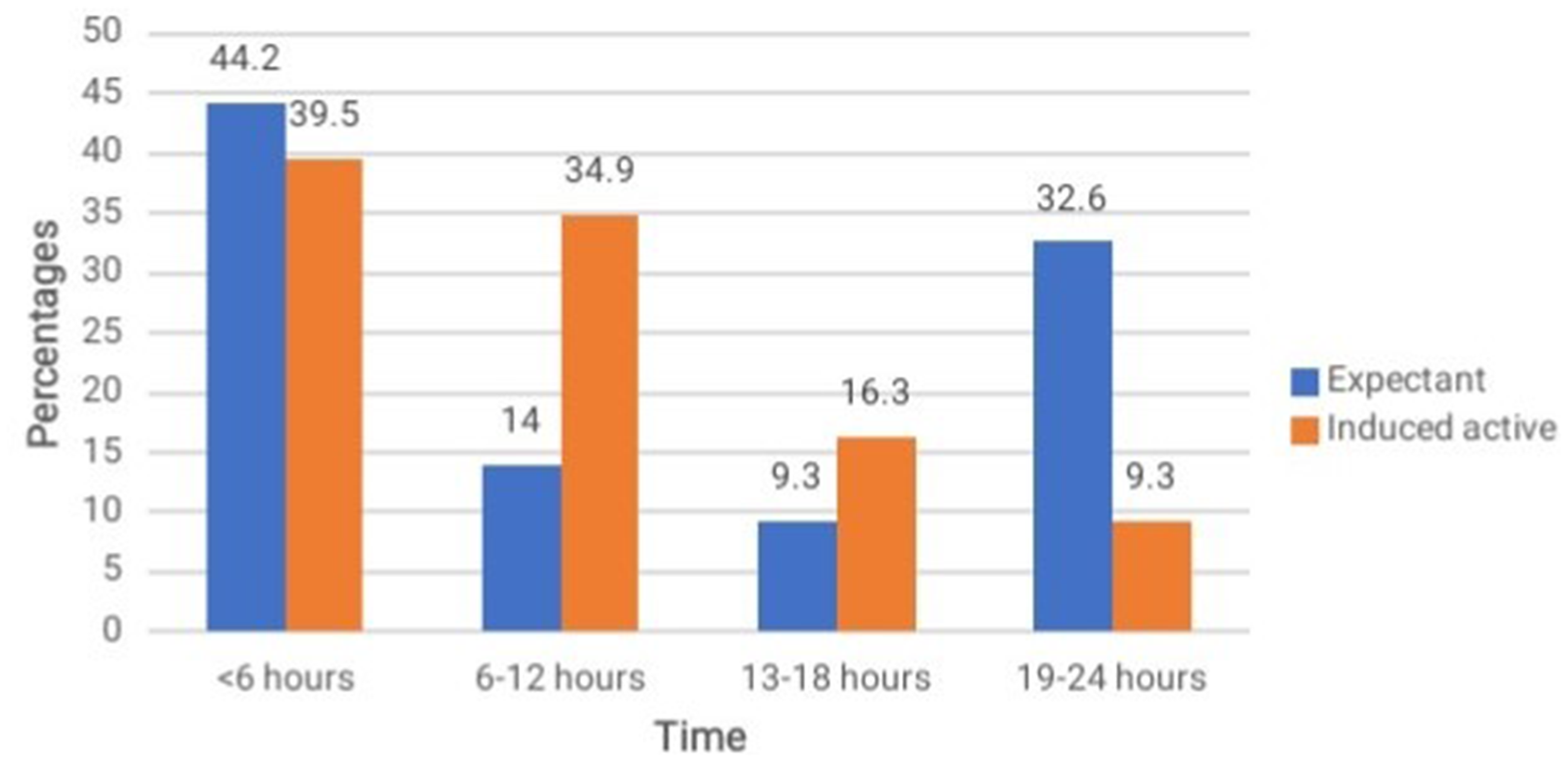
Latency period (i.e., interval between rupture of membranes to onset of labour) in expectant and induced active management groups.
There was no statistically significant difference between groups in mean (±SD) PROM-to-delivery times (i.e., 20.8 ± 5.9 hours and 18.7 ± 5.6 hours, for the expectant and active groups, respectively). However, although most deliveries in both groups occurred between 19 to 24 hours after PROM, fewer women delivered 18 hours after PROM in the active group (19 [44%]) compared with the expectant Group (27 [63%]) (Table 3).
There was a statistically significant difference (P = 0.010). between groups in mean (±SD) recruitment to delivery times after PROM (i.e., 14.7 ± 5.2 hours and 11.8 ± 5.0 hours, for the expectant and active groups, respectively). Analysis also showed a statistically significant difference (P = 0.04) in recruitment to delivery intervals between groups with fewer women delivered late after PROM (i.e., >18 hours) in the active group (8 [19%]) compared with the expectant group (18 [42%]) (Table 3 and Figure 3).

Recruitment to delivery intervals (i.e., time between being recruited into the study at the hospital to delivery of the baby) in expectant and induced active management groups.
As shown in Table 4, there was no statistically significant difference between groups in labour or delivery complications (i.e., maternal fever, abnormal uterine contractility patterns, requirement for augmentation of labour, need for instrumental delivery, postpartum haemorrhage and positive endocervical swab culture).
Labour and delivery complications.

Data are expressed as, n, n (%).
ns, not statistically significant.
There was no statistically significant difference between groups in foetal or perinatal complications (i.e., poor APGAR scores and NICU Admission) (Table 5). However, 9 (21%) of the newborns in the expectant group had subnormal APGAR scores of <8 in their 1st and 5th minutes after delivery compared with 4 (9%) in the active group. In both groups, the singular reason for NICU admission was foetal asphyxia (Table 5).
Foetal and perinatal outcomes and NICU Admission.

Data are expressed as, n, n (%).
NICU = Neonatal intensive care unit; ns, not statistically significant.
No baby delivered <6 hours after PROM was admitted to NICU (Table 6). Of the 13 babies born between 6 and 12 hours, only 2 were admitted to NICU. Of the 25 babies born between 13 and 18 hours, only one was admitted to NICU and only one of the 46 babies born after 19 hours after PROM was admitted to NICU. In addition, there was no statically significant difference between vaginal or caesarean delivery groups in cervical dilatation on presentation (Table 6).
Relationship between PROM to delivery and NICU admission and, route of delivery and cervical dilatation.

Data are expressed as n (%).
PROM = Premature Rupture of Foetal Membranes, NICU = Neonatal Intensive Care Unit; ns, not statistically significant.
Discussion
According to the primary outcome of this study, there was no difference in methods of delivery between active and expectant management of PROM at term. There was also no difference in feto- maternal complications between active and expectant management. However, active management significantly shortened the latency period and recruitment to delivery interval compared with expectant management.
The average age of our participants was 28 years which is similar to previous studies conducted in India or Egypt.22–24 Although not statically significant, we found that more women in the active management group (61%) than in the expectant management group (49%) presented to the hospital within 6 hours of PROM. These findings are comparable with studies from India and Brazil.24,25 In addition, we observed a statistically significant difference between groups in latency periods (i.e., the interval between PROM and onset of labour). For example, only 4/43 (9%) women in the active group had not gone into labour after 18 hours compared with 14/43 (33%) in the expectant group. These results are consistent with findings from another study from India that found all the women (50/50) in the active group had a latency period within 24 hours compared with 42/50 (84%) in the expectant group. 22 Our results are also consistent with findings another study from the UK 26 and one from Canada. 27
While there was no significant difference between management groups in PROM to delivery time, and, most deliveries in both groups occurred ≥19 to 24 hours after PROM, fewer women (19 [44%]) in the active group delivered after 18 hours compared with the expectant group (27 [63%]). This result is supported by a study conducted in a rural setting in India, where 23% of women in active management group compared with 30% in the expectant management group had a PROM to delivery interval of 10–15 hours. 23 Another study conducted in India involving women mainly from rural settings obtained similar results: 100% of women in active management group had a PROM to delivery interval within 24 hours compared with only 65% women in the expectant management group. 22
The strict adherence to the treatment protocols in the two treatment groups in this study supports the conclusion that induction of labour with sublingual prostaglandin E1 analogue (misoprostol) does not increase the risk of caesarean section, compared with the practice of expectant management. This finding is in contrast with results from several previous studies.28–32 However, we did observe that the rate of caesarean section was less in expectant management group (21%) compared with the active management group (30%) but the difference was not statistically significant.
Although not statistically significant, we found that 91% of newborns in the active group compared with 79% of newborns in the expectant group had APGAR scores ≥8 in the 1st and 5th minutes. By comparison, in a similar study conducted in India involving 50 women in each group, approximately 93% of neonates in each group had an APGAR score of >7 in 1st and 5th minutes. 22 In another study from Egypt, neonatal APGAR scores ≥ 7 taken in the 1st and 5th minutes were not statistically significant different between groups. However, for the active group, 78% of newborns had APGAR scores ≥7 in 1st minute compared with 84% in the expectant management group. The rate of APGAR scores ≥7 after 5 minutes was 100% in both groups. 23 The number of NICU admissions was low and identical in both groups (5%). These findings are consistent with those from other studies.22,24,33,34
Following the care provided to women and their babies in this study, the risk of neonatal infection and its sequalae were low and not influenced by the treatment practices. Therefore, there was no clear advantage to the mother and baby of one practice over another. While these results are comparable with some studies, 35 they differ from others that have found a low risk of neonatal infection if labour is induced shortly after the membrane rupture.36,37
The study had several limitations. For example, although we used the traditional tests of vaginal pooling, and nitrazine and fern tests of vaginal fluid for the diagnosis of PROM, other diagnostic tests have been proven to be more accurate than these standard tests, and so we may have missed some cases or over diagnosed others.38–40 In addition, the computation of the actual time of occurrence of PROM may have not been accurate because we relied on the account of the participants. Also, the diagnosis of chorioamnionitis and asphyxia were presumptive and not definitive. Furthermore, blinding of the treatments was not possible because of the obvious difference in management styles.
In summary, active management (immediate induction) of labour with sublingual prostaglandin E-1 analogue (misoprostol) and expectant management for PROM at term gave comparable outcomes in terms of rates of caesarean deliveries and maternal and perinatal complications. However, active management significantly shortened the latency period and induction to delivery intervals compared with the expectant management group. This may prove to be a desirable attribute of active management for PROM at term, especially in low resource settings. Women at term with PROM should be reassured that induction of labour is a reasonable option should they prefer this approach. In a resource poor environment like ours, active management may hold a slight advantage over expectant management where prophylactic intravenous antibiotics use in the expectant management may not be feasible or cost friendly. A large, randomized, placebo controlled, multi-centre study, with a high quality design would help corroborate and validate our results.
Footnotes
Acknowledgements
The authors are grateful to the research participants and all the hospital staff who took interest and helped out in the study, as well to the hospital management for creating an enabling environment and granting ethical approval.
Declaration of conflict of interests
The authors declare there are no conflicting interests.
Funding
This research was completely sponsored by the authors. There was no external funding to the research