
Abstract
Rosai–Dorfman disease (RDD) is a rare, benign, non-Langerhans cell histiocytic proliferative disease. RDD with central nervous system involvement is extremely rare. Surgical excision is generally regarded as the appropriate treatment of choice for this disease, especially when the lesion causes neurological compression. RDD can be accompanied by systemic symptoms, such as malaise, fever, weight change, leukocytosis, anemia, and hormonal disturbance, which may be challenging during general management. Little is known regarding peri-anesthesia management of this rare disease. We report a case of a patient in his 20s who had recurrent RDD and had general anesthesia with perioperative management. He was obese and hepatic insufficiency. This case report adds to the literature regarding the perioperative anesthetic management of RDD with central nervous system involvement.
Keywords
Introduction
Rosai–Dorfman disease (RDD) is a rare, benign, non-Langerhans cell histiocytosis with massive lymphadenopathy of uncertain etiology and a prevalence of 1:200,000. 1 RDD is commonly characterized by massive, painless, non-tender, bilateral cervical lymphadenopathy, and can be associated with systemic symptoms such as fever, weight loss, malaise, leukocytosis, and anemia. 2 RDD predominantly affects children and young adults with an average age of onset of 20.6 years. Extranodal involvement is usually observed in 50% of patients with RDD, while the central nervous system (CNS) is affected in only 5% of cases, usually as dural- or parenchymal-based lesions.3,4 CNS involvement can also mimic other diseases, such as meningioma, and is usually not associated with nodal disease. 5 The hallmark of RDD is emperipolesis, a major biological phenomenon, in which different types of bone marrow cells, such as lymphocytes or neutrophils, exist in the cytoplasm of histiocytes with a background of mature lymphocytes and plasma cells. 6 To date, the surgical approach of RDD remains the most successful treatment option when this disease involves the CNS. 7 In the case of anesthesia in RDD, an exhaustive pre-anesthetic evaluation is essential to identify associated clinical manifestations, which may affect the management of anesthesia. However, little is known regarding peri-anesthestic management of this rare disease. We report a case of a patient with recurrent RDD who had general anesthesia with perioperative management. He also had obesity and hepatic insufficiency. To the best of our knowledge, this situation has not been documented in previous literature.
Case description
A male patient in his early 20 s, who was 178 cm in height and weighed 120 kg with a body mass index of 37.9 kg/m2, was admitted to the Department of Neurosurgery in our hospital with no light perception in the right eye. His peripheral neuropathy and visual symptoms were secondary to a mass effect from a surrounding lesion and direct optic nerve invasion. He had sellar/suprasellar tumor resection under general anesthesia 1 year previously for decreased visual acuity and visual field contraction. A histopathological examination showed RDD. This condition had improved after surgery, but the same symptoms had re-appeared over the last 6 months. Computed tomography showed intracranial lesions (Figure 1). Magnetic resonance imaging showed a homogeneous isointense mass lesion in the sellar region. T1-weighted and T2 weighted liquid-suppressed sequence imaging showed an intracranial mass (Figure 2). On the basis of a previous study and experience,8,9 the patient had received chemotherapy with intravenous vindesine 4 mg and carboplatin 800 mg monthly for two times, but no improvement occurred. His alanine aminotransferase (ALT) concentration was 113.6 U/L and aspartate aminotransaminase (AST) concentration was 39.9 U/L before chemotherapy. His ALT and AST concentrations were elevated to 284.6U/L (7 times higher than normal) and 141.9 U/L (3.5 times higher than normal), respectively, after chemotherapy. The patient was upset by his visual symptoms and requested surgery. After 1 week of liver protection therapy in the Department of Gastroenterology, a preoperative examination showed abnormal liver enzymes with a decrease in serum ALT and AST concentrations to 143 U/L and 98 U/L, respectively. Additionally, his total bilirubin concentration was 19.8 µmol/L, direct bilirubin concentration was 7.4 µmol/L, albumin concentration was 40.3 g/L, total protein concentration was 67.2 g/L, and creatinine concentration was 66.8 µmol/L. A B-mode ultrasound examination revealed mild fatty liver (Figure 3). Despite expressing considerable concern about the possible risks of surgery and anesthesia, the patient accepted them and consented to have general anesthesia. The patient then underwent resection of the lesion in the sellar area with right frontotemporal craniotomy (Figure 4).
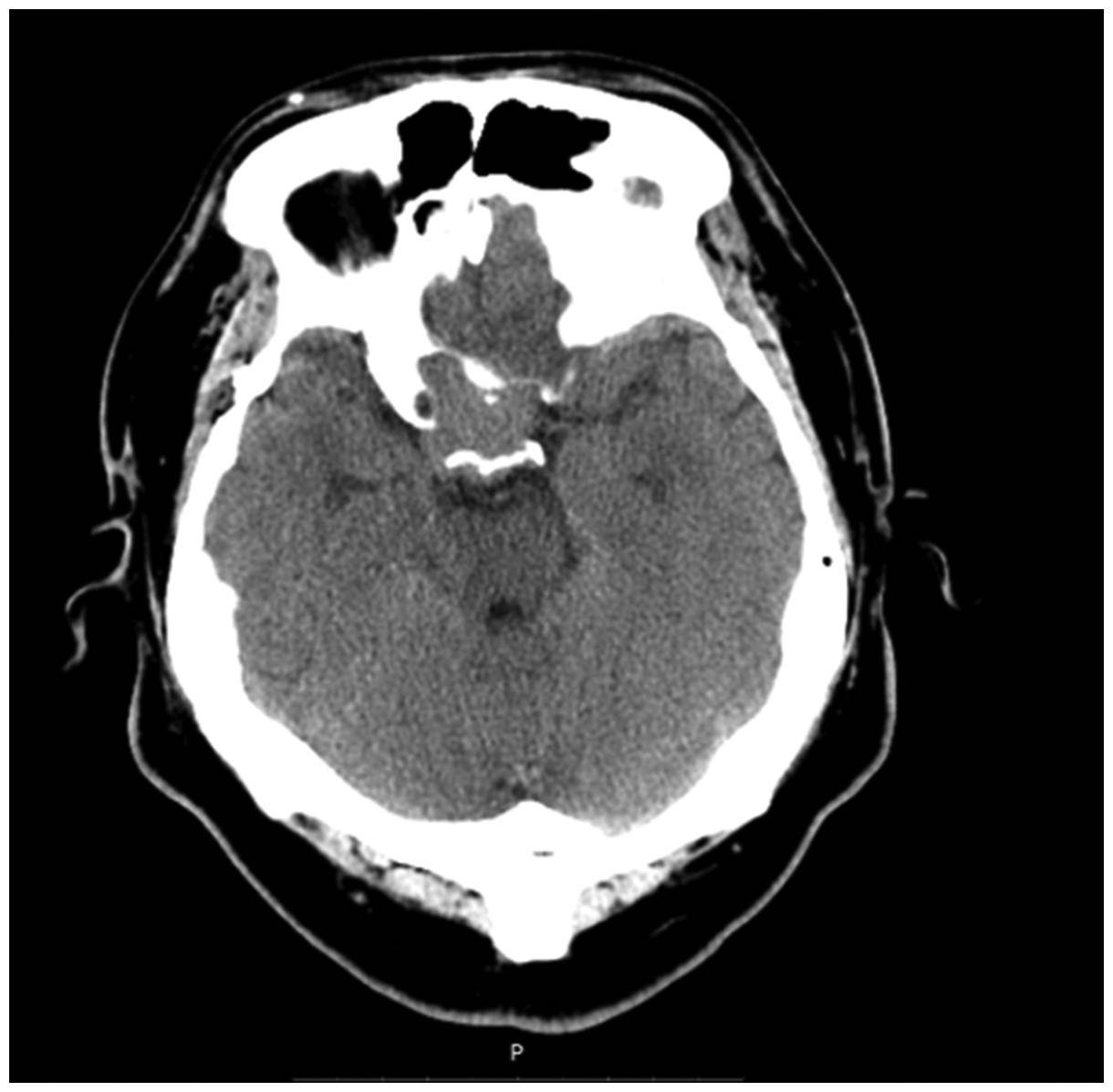
Computed tomography shows intracranial lesions.

T1-weighted (left) and T2 weighted (right) liquid-suppressed sequence imaging shows an intracranial mass.

A B-mode ultrasound examination shows mild fatty liver

Intraoperative images before (top panel) and after (bottom panel) intracranial mass resection.
Management of anesthesia
On his arrival in the operating room, his blood pressure was 118/68 mm Hg and his heart rate was 78 beats/minute. Standard anesthetic monitoring was performed, including an electrocardiogram, pulse oximetry, invasive blood pressure, and end-tidal CO2. During preoxygenation, anesthesia was induced with 30 μg sufentanil, 20 mg cisatracurium, and 120 mg propofol. After intravenous injection of 20 mg cisatracurium, the motor response after jaw-thrust was tested to assess an adequate anesthetic depth. Tracheal intubation was performed under video laryngoscopy using a steel wire reinforced tube with an internal diameter of 8 mm and a high-volume, low-pressure cuff that was inserted smoothly in a single attempt. Lung sounds were confirmed by stethoscope, and no wheezing or accidental sounds were heard. Femoral venous catheter placement was performed under ultrasound guidance. The protocol for maintaining anesthesia consisted of remifentanil (0.1 μg/kg/min) and sevoflurane (0.9–1.1 minimum alveolar concentration) mixed with 60% air/oxygen, while the bispectral index was maintained between 45 and 55. The patient’s lungs were ventilated at a respiration rate of 12 breaths/minute at an inspiratory to expiratory ratio of 1: 2. With regard to mechanical ventilation, a volume-controlled ventilation mode was applied, with a volume of 8 to 10 mL/kg and an end-tidal CO2 of 30 to 40 mmHg. A positive end-expiratory pressure of 5 cmH2O was used during the whole operation to avoid the development of postoperative pulmonary atelectasis. Before placement of a head holder and making a skin incision, bilateral scalp nerve blocks were performed using 20 mL of 0.5% ropivacaine. The entire surgical procedure lasted 490 minutes with the patient’s upper body in an elevated position. The patient was successfully extubated following a bispectral index >90, tidal volume >500 mL, respiratory rate of 13 times/minute, and pulse oxygen saturation >95% with inhalation of 21% oxygen.
Thereafter, the patient was transferred to the postoperative anesthesia care unit for further evaluation. No perioperative or anesthetic complications occurred. Finally, the patient was discharged home on the 12th postoperative day with a postoperative pathological diagnosis of RDD (Figure 5).
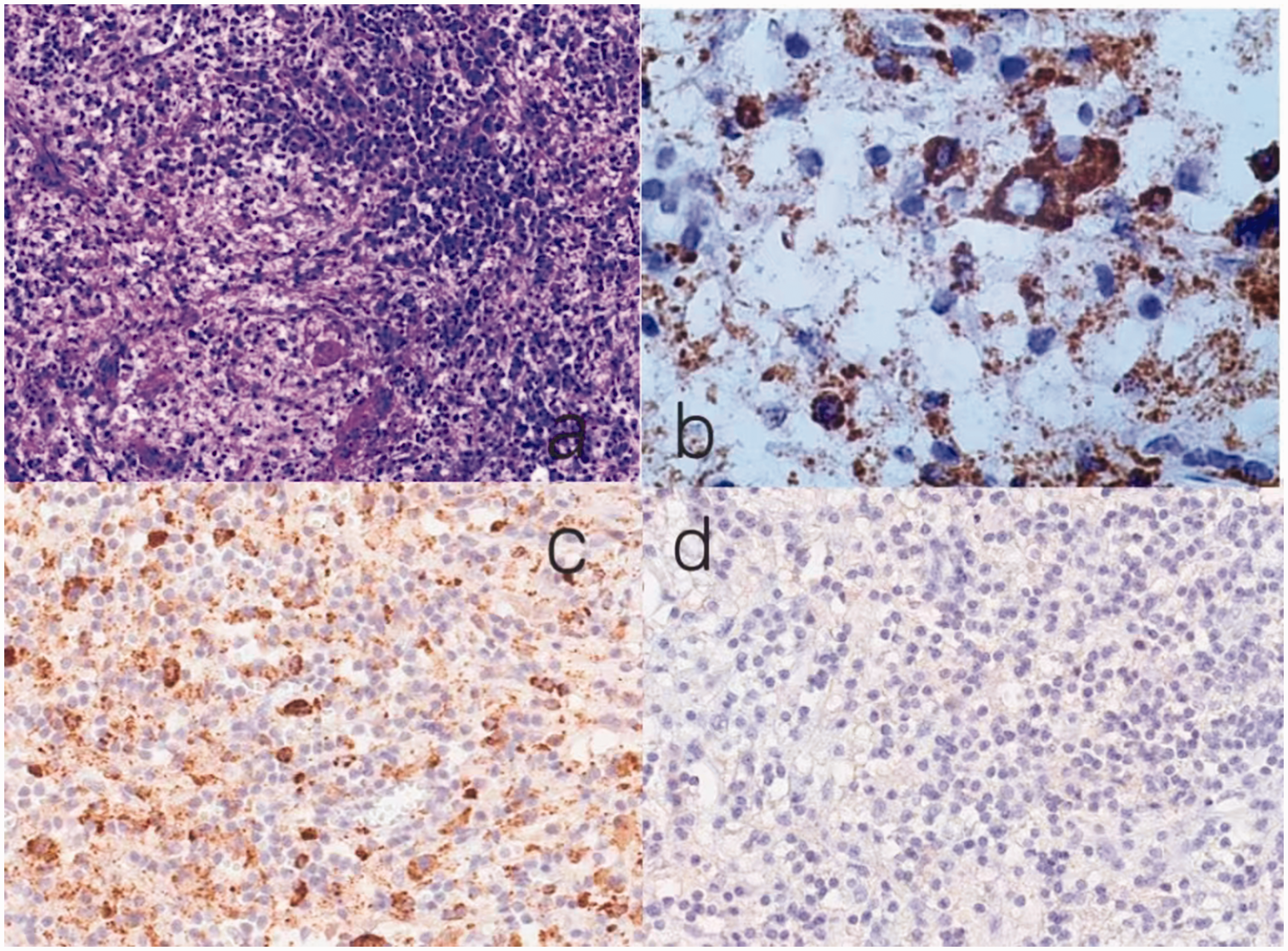
Histopathological examination. (a) Polymorphous infiltrate of histiocytes, lymphocytes, and plasma cells. (b) Histiocytes are positive for CD68. (c) Histiocytes are positive for S-100 and (d) Histiocytes are negative for CD1a.
Discussion
RDD showing CNS involvement is extremely rare. Patients with RDD usually display a self-limiting clinical course, but rapid progression of extranodular lesions including CNS involvement can result in a poor prognosis. 10 Surgical excision is generally regarded as the appropriate treatment of choice for RDD, especially when the lesion causes neurological compression. 11 This case report is the first to describe the safe administration of inhalation anesthesia with an uneventful perioperative course in a patient with RDD from the perspective of anesthetic management.
In pre-anesthetic evaluation of RDD, evaluation of the degree of organ involvement and the location of intracranial occupation is essential. An assessment of the respiratory system should include checking for extrinsic airway compression and an obstructive or restrictive pattern on lung function tests because RDD with cervical lymphadenopathy is commonly present. Tracheal intubation should be performed under video laryngoscopy for the preparation of difficult airway intubation. The intracranial mass in this patient was located at the sellar region on the right side, which was adjacent to the cavernous sinus, anterior and middle cerebral arteries, the pituitary, and the trigeminal nerve. Moreover, the mass wrapped around the internal carotid artery siphon, and postoperative adhesion may have occurred after the last surgery. These findings may have contributed to a high risk of massive hemorrhage and cardiovascular and autonomic responses due to intraoperative cranial nerve traction. Peripheral intravenous cannulation is necessary for the administration of fluids and medication during anesthesia. However, because of cervical lymph node involvement in patients with RDD, when performing central venous catheter placement, choosing the femoral vein and operating under ultrasound guidance may be safer. Additionally, preoperative physical and imaging examinations should be performed to avoid lymphadenopathy puncture. Blood for transfusion and vasoactive medications should be prepared before the operation. During the operation, anesthesiologists should pay close attention to the surgeons’ procedure and the vital signs of patients to anticipate possible problems. Moreover, when the location of the mass is close to the posterior pituitary and there is possible damage to the pituitary, careful monitoring of perioperative hormone concentrations is required. On the basis of previous clinical experience of postoperative medication application for sellar region mass resection, thyroxine and desmopressin were administered prophylactically to our patient. 12 Thyroid hormone and pituitary gonadal hormone concentrations in the patient were maintained in the normal range until he left the hospital.
Our patient’s height was 178 cm and weight was 120 kg with a body mass index of 37.9 kg/m2. He was classified as obese class II in accordance with the classification of body weight according to the World Health Organization. 13 In patients with obesity, absolute values of total blood and plasma volume appear to be increased. However, when body weight is taken into account, patients with obesity have a blood volume of only approximately 45 mL/kg compared with 70 mL/kg in patients with a normal weight. 14 Therefore, the induction of general anesthesia might increase the risk of hemodynamic instability. Previous studies have reported that a scalp nerve block alleviates the craniotomy-associated response due to dramatic stimuli, such as incisions, drilling, and screwing, and thus provides hemodynamic stability.15,16 In our case, after supraorbital, auriculotemporal, greater occipital nerve and lesser occipital nerve nerve blockade, no sharp fluctuation in heart rate or blood pressure was observed after the placement of a head holder and performing the skin incision. Volatile anesthetics with more lipophilic properties are thought to accumulate in fat tissue, causing delayed emergence after anesthesia longer than 2 to 4 hours. However, sevoflurane is a novel type of inhaled anesthetic with no upper respiratory irritation and low respiratory inhibition. After inhalation of sevoflurane is terminated, it may be quickly metabolized and eliminated through the respiratory system. Therefore, inhalation anesthetics with relatively low lipid solubility, such as sevoflurane, may be beneficial for rapid awakening and stable recovery of protective airway reflexes. 17 To minimize atelectasis formation during mechanical ventilation, the application of adequate positive end-expiratory pressure provides beneficial effects on arterial partial pressure of oxygen and the alveolar–arterial oxygen difference in patients with obesity. Additionally, ventilating with 60% instead of 100% oxygen prevents the formation of atelectasis during induction and subsequent anesthesia. 18
Our patient was considered to have abnormal preoperative liver enzyme results, with a serum ALT concentration more than 1.5 times higher than the upper limit of normal in the week before surgery. 19 This finding may be related to his fatty liver history and application of chemotherapy drugs. The decreased ability of the liver to metabolize drugs needs to be considered when choosing the type and the dose of anesthetic. Inhalation anesthesia and intravenous anesthesia are widely used anesthetic approaches in craniotomies. 20 Studies have shown that using inhalation agents alone or in combination with small doses of opioids can be considered a reasonable regimen for patients with liver disease.21,22 To minimize rug metabolism through liver, sevoflurane should take priority over other inhaled anesthetics because of its characteristics of rapid induction, recovery, and minimal biotransformation. With regard to neuromuscular blocking agents, cisatracurium is recommended because of its pH- and temperature-dependent Hofmann elimination in plasma and tissues. Although volatile anesthetics may cause drug-induced liver injury, 23 no rise in serum ALT concentrations or other complications were observed in our patient after surgery. Our findings may provide an alternative for clinicians in choosing an anesthetic regimen for patients with perioperative elevated liver enzymes.
RDD is characterized histopathologically by the accumulation of CD68-positive, S100-positive, and CD1a-negative histiocytes with frequent emperipolesis. 24 Organ involvement includes skin and subcutaneous tissue RDD, lymph node RDD, bone RDD, CNS RDD, and glandular tissue RDD. 9 Our patient was diagnosed with CNS RDD. RDD of the CNS is rare and tends to occur in an isolated area, which typically involves the meninges. This condition presents as an enhancing dural-based lesion with surrounding vasogenic edema, which is often confused with meningioma owing to their similar imaging qualities. A definitive diagnosis of RDD of the CNS is established by a histopathological examination of biopsy tissue. A microscopic examination typically shows a polymorphous infiltrate of histiocytes, lymphocytes, and plasma cells in a fibrous stroma. 25 Two subtypes of histiocytes (large histiocytes and medium-sized histiocytes), which are differentiated by size, are present in RDD. Large histiocytes typically show emperipolesis, containing well-preserved lymphocytes and are usually S-100 positive, 26 which is consistent with the histopathological examination results in our patient. Medium-sized histiocytes may not show emperipolesis, and are probably representative of histiocytes at an earlier stage and are S-100 negative. Large and medium-sized histiocytes are positive for CD68. Non-surgical options for RDD of the CNS include irradiation, chemotherapy, and steroids. However, resection of the intracranial mass may still be the most effective treatment for this condition.
Conclusion
As a rare disease, research on RDD affecting the CNS still needs further investigation. We describe here a case of successful anesthetic management of recurrent RDD of the CNS in a patient with elevated liver enzymes and obesity. Combined with the characteristics of neurosurgery, we present an alternative anesthetic management approach using inhalation anesthesia with sevoflurane and remifentanil, and discuss the anesthetic concerns of this rare disease. In summary, detailed knowledge of the systematic involvement of RDD along with the different effects of anesthetic medications in these patients may lead to a safe anesthetic-surgical procedure. The reporting of this study conforms to the CARE guidelines 27 .
Footnotes
Author contributions
Yu Lu and Xinlei Zhang conceived the idea for this study. Xiangjun Zhou performed the literature search and was responsible for writing the manuscript with the assistance of Xinlei Zhang. Hanjie Liu and Dezhi Li conducted the study and performed data collection with the assistance of Song Liu. All authors were involved in data interpretation.
Data availability statement
Original research data are available for this report.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
We obtained consent from the patient to perform all of the treatments. We also obtained written signed consent to publish from the patient. This study was approved by Beijing Tiantan Hospital’s Institutional Review Board.
Funding
This study was supported by the National Natural Science Foundation of China (No. 82171364 to SL); the Beijing Municipal Health Commission (No. PXM2020_026280_000002 to SL); and the Institut pour la Recherche sur la Moelle Epiniere et l’Encephale (IRME, Paris, France) (to SL). The sponsors had no role in the trial design, trial conduct, data handling, data analysis or writing, and publication of the manuscript.