
Abstract
The standard of care for newly diagnosed advanced ovarian cancer is surgical cytoreduction plus platinum-based chemotherapy; however, recurrent disease frequently occurs after treatment. Poly(ADP-ribose) polymerase (PARP) inhibitors as first-line maintenance therapy have been demonstrated to significantly reduce the risk of disease progression or death in patients with advanced ovarian cancer who have a complete or partial response to first-line platinum-based chemotherapy. Niraparib is the only PARP inhibitor that offers a significant progression-free survival benefit compared with placebo in this patient population regardless of the homologous recombination status. However, predictive factors for treatment responses and approaches to dose optimization remain to be investigated. In this study, two Chinese patients with newly diagnosed advanced ovarian cancer exhibited long-term responses to niraparib treatment, and hematological toxicity was successfully managed by dose adjustment. The literature on clinical trials and real-world experience on the efficacy, tolerability, and dose individualization of niraparib treatment in Western and Chinese patients was also reviewed. Future research is warranted to identify the characteristics of ‘long responders’ to niraparib treatment.
Keywords
Introduction
Ovarian cancer (a collective term for cancers of the ovary, peritoneum, and fallopian tube) is among the 10 most commonly diagnosed malignancies in women globally, causing an estimated 300,000 new cases per year. 1 Most patients are diagnosed with advanced disease, defined as the spread of the disease outside the pelvis (International Federation of Gynecology and Obstetrics [FIGO] stage III or IV). 2 The most common, and most aggressive, subtype of malignant ovarian cancers is high-grade serous epithelial carcinoma. 3 Newly diagnosed advanced ovarian cancer can be treated with debulking surgery or neoadjuvant chemotherapy plus interval debulking surgery (possibly with the use of hyperthermic intraperitoneal chemotherapy [HIPEC]), followed by platinum-based chemotherapy. 2 , 4 However, approximately 85% of patients will develop recurrent disease after the completion of primary treatment. 5
To reduce the risk of disease progression or death after first-line chemotherapy in women with advanced ovarian cancer, several maintenance therapies have been investigated. One feasible approach is the addition of bevacizumab, an antiangiogenic agent, to chemotherapy, followed by bevacizumab maintenance treatment. However, the main limitations of this strategy include safety concerns and a lack of data on patients who received neoadjuvant chemotherapy. 6 , 7 Since 2018, the introduction of poly(ADP-ribose) polymerase (PARP) inhibitors has transformed the landscape of first-line maintenance therapy for patients with advanced ovarian cancer who have a complete or partial response to first-line platinum-based chemotherapy.8–11
Among PARP inhibitors, niraparib is the only treatment option that significantly improved progression-free survival (PFS) compared with placebo for tumors regardless of the presence of BRCA mutations, homologous recombination deficiency (HRD), or homologous recombination proficiency (HRP), 12 suggesting that its mechanisms of action 13 , 14 differs those of other PARP inhibitors, which are mostly associated with the repair of DNA damage. In the pivotal phase III PRIMA study, 10 niraparib significantly improved median PFS compared with placebo in all key subgroups of patients with FIGO stage III or IV ovarian cancer who had a complete or partial response to platinum-based chemotherapy. Consistent results (Table 1) were obtained in a similar study conducted in Chinese patients, named PRIME, which was presented at the Society of Gynecologic Oncology 2022 Annual Meeting on Women’s Cancer. 15
Median progression-free survival (months) achieved in different subgroups of the PRIMA and PRIME studies.

HRD, homologous recombination deficiency; HRP, homologous recombination proficiency.
Despite the efficacy shown in clinical trials, there are few reports on the optimal dosing, tolerability, patient-reported outcomes, and treatment responses in real-world patients treated with niraparib, especially among Asian populations. The two cases presented in this study provide insights into the importance of dose individualization in preserving patient quality of life and thus facilitating continuation of niraparib treatment. The determinants of the responsiveness to niraparib treatment are also discussed.
Case reports
The reporting of this study conforms to the CARE guidelines. 16 All patient details were de-identified. Written informed consent for treatment and publication of this report was obtained from both patients. The Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster waived the need for approval for publication of the retrospectively obtained and anonymized data for these case reports.
Case 1
A nearly 70-year-old woman presented with urinary frequency and a large pelvic mass on physical examination. In August 2020, pelvic magnetic resonance imaging (MRI) and positron emission tomography (PET)/computed tomography (CT) revealed the presence of a large tubo-ovarian mass (along with ascites), multiple peritoneal nodules, and a left pelvic node. The preoperative cancer antigen 125 (CA125) level was 791.0 U/mL. The patient underwent laparoscopic bilateral salpingo-oophorectomy, peritoneal mass biopsy, and partial omentectomy. The intraoperative pathological diagnosis was high-grade serous adenocarcinoma on the surface of the left fallopian tube (with a tubal intraepithelial tumor found in the omentum). Both ovaries were free of cancer. FIGO stage IIIC disease was confirmed.
A multidisciplinary team decided to perform neoadjuvant chemotherapy followed by interval debulking surgery. From September to October 2020, the patient received three cycles of neoadjuvant chemotherapy with carboplatin (area under the curve = 5; intravenous [IV] infusion on day 1) plus paclitaxel (175 mg/m2; IV infusion over 3 hours on day 1) once every 3 weeks. On 11 November 2020, the CA125 level decreased to 16.8 U/mL, and interim PET/CT uncovered remarkable improvements of the pre-existing peritoneal metastases.
One week later, the patient underwent interval debulking surgery and HIPEC. The intraoperative findings confirmed the presence of residual tumors measuring up to 4 cm in the omentum, as well as smaller nodules over the transverse colon, distal ileum, left pelvic peritoneum, and mesosigmoid. The right diaphragm was thickened. The Peritoneal Cancer Index was 8, and no residual peritoneal disease was detected after the interval surgery. The subsequent genomic assay of the resected tumor revealed wild-type BRCA with HRD.
From December 2020 to February 2021, the patient received three additional cycles of chemotherapy with carboplatin and paclitaxel. Her post-chemotherapy CA125 level was 14.2 U/mL. In March 2021, in view of her platinum sensitivity, the patient was started on maintenance treatment with niraparib 200 mg once daily. After 3 weeks of treatment, she developed grade 4 thrombocytopenia, which required platelet transfusion, but no bleeding tendency was observed. She also experienced mild nausea and anorexia while taking the full dose of 200 mg. From May to October 2021, after recovering from thrombocytopenia, the patient resumed niraparib treatment at a reduced dose of 100 mg daily. From October 2021, the niraparib regimen was stepped up to a cycle of 200 mg daily for 1 day followed by 100 mg daily for 2 days (equivalent to an average daily dose of 133.3 mg). On the latest follow-up visit on 7 June 2022, the patient remained on the individualized niraparib regimen, and she had a diminished CA125 level of 7.5 U/mL with no evidence of clinical, serological, or radiological recurrence.
Case 2
A woman in her early 60 s presented with abdominal discomfort and a CA125 level of 4490 U/mL. On 12 February 2019, PET/CT disclosed a large omental mass measuring 14.7 cm, a left ovarian tumor measuring 7.6 cm, multiple abdominopelvic lymph nodes, multiple peritoneal metastases, small ascites, a small left supraclavicular node, and a subcarinal node (Figure 1). Cytological analysis of the ascitic fluid revealed metastatic adenocarcinoma that originated from the ovary. Considering the presence of multiple positive nodes and metastases, an interdisciplinary team at our center decided to prescribe the patient neoadjuvant chemotherapy. From February to April 2019, she received carboplatin/paclitaxel every 3 weeks for three cycles. The treatment response was good. Her CA125 level decreased to 72.7 U/mL, and PET/CT revealed reductions in the sizes and metabolic activities of the omental and ovarian masses. Previously hypermetabolic lymph nodes including the left supraclavicular node became metabolically quiescent.

Reductions of lesions detected on positron emission tomography/computed tomography in Patient 2. The left column presents the images obtained in February 2019 prior to neoadjuvant chemotherapy, and the right column presents the corresponding images from December 2021 after prolonged niraparib maintenance. (a) A large omental mass and a left ovarian tumor. (b) Multiple abdominopelvic lymph nodes. (c) A large omental mass and (d) Multiple peritoneal metastases
On 9 May 2019, we performed interval cytoreductive surgery (CRS) combined with HIPEC; however, she had residual peritoneal disease after the surgery. Pathology specimens indicated the presence of numerous high-grade serous carcinomas over the peritoneum, bowel mesentery, pouch of Douglas, subdiaphragmatic peritoneum, and large omental cake. Somatic tumor testing for BRCA genes was negative. From June to August 2019, she received IV plus intraperitoneal (IP) chemotherapy with paclitaxel/cisplatin every 3 weeks for three cycles. Follow-up PET/CT scan revealed no peritoneal lesions and only a small residual inactive left supraclavicular node.
On 19 November 2019, the patient started daily treatment with niraparib 200 mg. Two months later, she experienced grade 3 thrombocytopenia, grade 2 neutropenia, and grade 2 anemia. Niraparib treatment was thus suspended for 2 weeks. In January 2020, treatment resumed with alternate-day dosing of 100 mg/200 mg daily (equivalent to a weekly dose of 1000 mg; approximately 70% dose density of 200 mg daily). However, she developed grade 3 anemia (hemoglobin, 7.1 g/dL) and complained of lethargy affecting her ability to play tennis that necessitated blood transfusion. In mid-February 2020, the dose of niraparib was further reduced to 100 mg daily, and this dose was well tolerated. Despite mild nausea and gastrointestinal discomfort, the patient maintained her body weight and tennis performance and enjoyed a good quality of life. As of May 2022, she has remained on niraparib treatment for >30 months, and her condition was considered stable based on PET/CT performed in December 2021 (Figure 1). The tumors were confirmed to have a status of HRP.
Discussion
Both patients had FIGO stage III or IV high-grade serous ovarian cancer or carcinoma of the fallopian tube that was platinum-sensitive (Table 2). At the time, the use of niraparib as first-line maintenance therapy was off-label in our jurisdiction; however, it was supported by the results of the PRIMA study presented at the European Society for Medical Oncology Congress 2019, 10 , 17 which demonstrated the significant PFS benefit of niraparib treatment over placebo regardless of the status of homologous recombination (HR).
Patient characteristics.
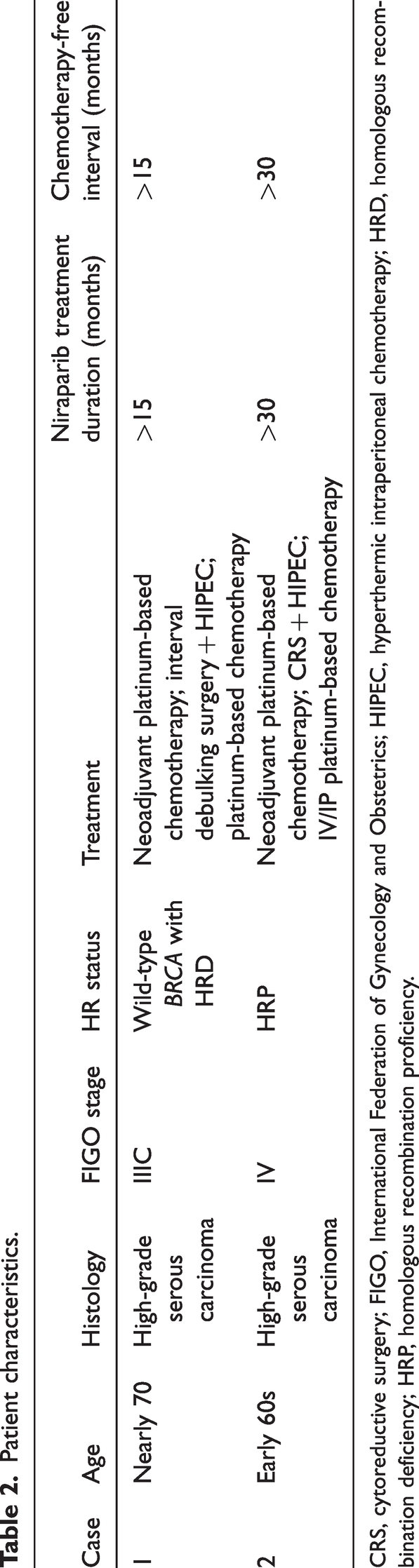
CRS, cytoreductive surgery; FIGO, International Federation of Gynecology and Obstetrics; HIPEC, hyperthermic intraperitoneal chemotherapy; HRD, homologous recombination deficiency; HRP, homologous recombination proficiency.
In addition to the sensitivity to platinum-based chemotherapy, the HRD status is a conventionally important determinant of the responsiveness to PARP inhibitor treatment. 18 Patient 1, who has wild-type BRCA with HRD, remained on niraparib treatment for >15 months with a good quality of life and no evidence of recurrence. Evaluated from the initiation of niraparib treatment, PFS has already exceeded 15 months, which was comparable to the median PFS of 19.6 months in the wild-type BRCA with HRD subgroup of PRIMA. 10 The corresponding median PFS in PRIME was 24.8 months. 15 Approximately 50% of the PRIME participants received neoadjuvant chemotherapy, and >75% had optimal postoperative outcomes. 15 Given that Patient 1 shared these prognostic characteristics, it is reasonable to expect that her post-niraparib PFS might ultimately be comparable to the PRIME data, i.e., approximately 10 months longer than her current record.
Although clinical decision-making remains challenging in patients with HRP, who account for nearly half of patients with high-grade serous ovarian cancers, 19 niraparib could be a feasible treatment option, as supported by a European expert panel, 12 as well as the long-term response observed in Patient 2, who received niraparib for >30 months with no disease progression as of May 2022. This treatment response was significantly more promising than the median PFS achieved across all subgroups of PRIMA 10 and PRIME. 15 Patient 2 might have a better prognosis and thus a longer response to niraparib treatment. This patient was treated with IV/IP chemotherapy and interval CRS/HIPEC, and it is unclear whether these factors were related to her good response to niraparib maintenance therapy. This case also demonstrated that the HR status is not necessarily the only primary predicator for responsiveness to niraparib.
Our case reports highlight the importance of a tailored dosing regimen that can help reduce adverse events (AEs), preserve quality of life, and facilitate compliance with long-term niraparib treatment, which is expected to be maintained for at least 3 years after first-line platinum-based chemotherapy to minimize the risk of recurrence. 10 , 12 In the PRIMA study, 10 approximately 65% of participants in the niraparib arm received a fixed dose of 300 mg daily per the initial protocol. After a protocol amendment, approximately 35% of patients received an individualized dose of 200 mg daily based on body weight and platelet counts. This practice was derived from a retrospective analysis of the NOVA trial, 20 , 21 which revealed that the efficacy of niraparib in terms of PFS was consistent across different initial doses (100, 200, or 300 mg daily) in patients with recurrent platinum-sensitive ovarian cancer and that a starting dose of 200 mg daily could reduce the risk of thrombocytopenia in high-risk patients (i.e., with a baseline body weight of <77 kg or a platelet count of <150,000/µL). According to the safety data in PRIMA, 10 most patients with thrombocytopenia can be managed by dose interruption, followed by re-initiation of treatment at the recommended dose or a reduced dose. The PRIME study, in which all niraparib-treated participants received an individualized starting dose, recorded an improved safety profile for niraparib, including a lower proportion of patients who required dose reduction than NOVA and PRIMA. 15 Both of our patients, who weighed 40 to 50 kg, could not tolerate a dose of 200 mg daily in the first 1 to 2 months because of hematological toxicity. Importantly, they could remain on treatment with dose interruption, dose reduction, or partial step-up to a 50% to 67% intensity of the daily dose of 200 mg with an opportunity to resume treatment at the recommended dose after AEs were corrected. For patients who cannot tolerate niraparib 200 mg daily because of AEs, this stepwise approach could facilitate their adherence to the recommended dose over the long term.
The AEs of niraparib reported in our cases, which were mostly hematological and gastrointestinal events, were consistent with those demonstrated in PRIMA 10 and PRIME, 15 as well as real-world experience in Chinese patients, 22 , 23 in which 12% to 17% of patients developed grade 3/4 thrombocytopenia. According to the niraparib prescribing information approved in Hong Kong, 24 patients should be monitored for hematological parameters during treatment by testing complete blood counts weekly for the first month, followed by monthly monitoring thereafter. In the event of thrombocytopenia, niraparib treatment should be suspended until the platelet count is normalized. Gastrointestinal discomfort is another common AE of niraparib. 10 , 15 , 23 Our patients found that taking niraparib at night or using antiemetics reduced the impact of nausea.
One strength of this study was its illustration of the clinical practicability of dose individualization to facilitate the continuation of niraparib treatment in Asian patients. Additionally, this study explored the potential for IV/IP chemotherapy and interval CRS/HIPEC followed by niraparib treatment to improve clinical outcomes, especially in patients with HRP. The treatment responses of these patient populations in a real-world setting are rarely reported in the current literature. The limitations of this study included insufficient generalizability because of the nature of case reports and the relatively short follow-up periods of the patients.
First-line maintenance therapy with PARP inhibitors has significantly reduced the risk of disease progression or death in patients with advanced ovarian cancer after a complete or partial response to first-line platinum-based chemotherapy. Niraparib serves as a treatment option for this patient population regardless of the HR status. Future studies are warranted to investigate predictors of response to niraparib treatment to identify ‘long responders.’ Most AEs of niraparib are manageable by dose reduction and dose interruption. A tailored regimen (e.g., using a 50%–67% dose intensity, followed by resuming treatment at 50% of the recommended dose of 200 mg daily after the resolution of AEs) could help lean patients remain on niraparib treatment with promising tolerability, disease control, and quality of life. Regular monitoring for hematological parameters during treatment is recommended.
Footnotes
Author contributions
The author is the sole contributor of this work and has approved it for publication.
Data availability statement
The author confirms that the data supporting the findings of this study are available within the article. Further inquiries may be directed to the author.
Declaration of conflicting interests
The author declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.