
Abstract
We describe the case of a patient who swallowed a small fish bone and felt it lodge in her pharynx, but failed to seek medical attention in a timely manner. One week later, no foreign body was found in the hypopharynx or larynx, but a small purulent cyst was present in the epiglottic vallecula. A computed tomography scan showed a high-density area on the lingual surface of the epiglottis, which was considered to represent an embedded fish bone. A week later, the patient’s discomfort had subsided, and flexible videoendoscopy showed that the purulent cyst in the epiglottic vallecula had disappeared. We surmise that the purulent cyst had ruptured spontaneously and the foreign body had been discharged. This represents an example of how an impacted small foreign body may be spontaneously discharged from the body.
Introduction
Fish bones are among the most common causes of foreign body impaction in the pharynx and esophagus. In the present case, the patient swallowed a small fish bone and felt it lodge in her pharynx, but she failed to seek medical attention in a timely manner. One week later, no foreign body was found in the hypopharynx or larynx, but a small purulent cyst was present in the epiglottic vallecula.
Case report
The reporting of this case conforms to the CARE guidelines. 1
A 25-year-old female patient felt a small fish bone in her throat while eating fish. She felt the fish bone stick to the left side of the midline of the pharyngeal cavity and had a slight sensation of a foreign body in her pharynx. One week later, the foreign body sensation in her pharynx had not disappeared, but rather had worsened. Flexible videoendoscopy did not reveal a fish bone, but a purulent cyst was apparent in the left epiglottic vallecula (Figure 1). It was not clear whether this purulent cyst had been caused by the fish bone; therefore, a non-enhanced computed tomography (CT) scan was performed and a three-dimensional reconstruction of the pharynx was generated. The CT scan showed a high-density image on the lingual surface of the epiglottis, which was considered to be the embedded fish bone. Specifically, high-density areas representing the fish bone can be seen on two axial CT slices (Figure 2), two sagittal CT slices (Figure 3) and three coronal CT slices (Figure 4). The thickness of the CT scan was 0.5 mm; therefore, the diameter of the foreign body was estimated to be approximately 1 to 1.5 mm and its length approximately 1.5 to 2 mm. On the basis of a consideration of the history of the patient and the results of laryngoscopy and CT examination, we concluded that the purulent cyst located in the epiglottic vallecula was the result of fish bone impaction. A week later, the patient’s discomfort disappeared, and flexible videoendoscopy showed that the purulent cyst in the epiglottic vallecula had disappeared (Figure 5).

Flexible videoendoscopy image showing a purulent cyst in the left epiglottic vallecular.

Axial computed tomography image. The arrow indicates the fish bone in the cyst.
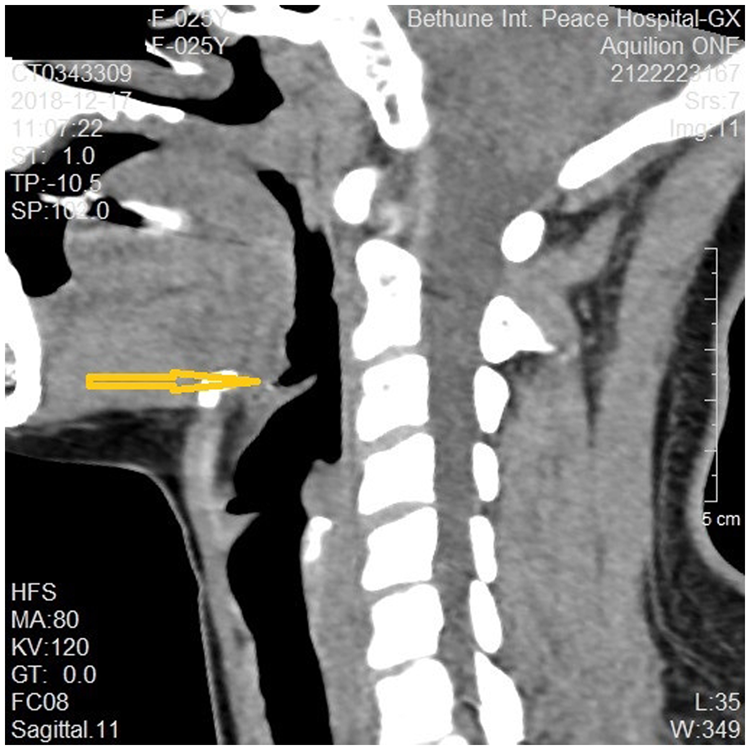
Sagittal computed tomography image. The arrow indicates the fish bone in the cyst.

Coronal computed tomography image. The arrow indicates the fish bone in the cyst.

Flexible videoendoscopy showing that the purulent cyst in the epiglottic vallecula had disappeared.
Discussion
It has been shown that 80% to 90% of ingested foreign bodies enter the gastrointestinal tract, but in only 10% to 20% of cases, they puncture the mucosa or become trapped, necessitating endoscopic or surgical removal. 2 Fish bones that become embedded in the oropharynx or hypopharynx are more commonly found in the tonsil, tongue base, epiglottic vallecula or piriform fossa.2–4
If a fish bone becomes impacted in the pharynx and medical treatment is delayed, it will persist for a long time. Furthermore, friction with the foreign body may cause the local development of ulcers or white matter on the area of mucosa that is in contact with the foreign body, 3 and this aids the localization of the foreign body. If the impacted fish bone is long, it can penetrate deep into the mucosa because of the pressure of swallowing. If the tip of the fish bone can be seen on examination, it can be removed, but if the impacted fish bone is small and the patient continues to eat normally, it can enter the mucosa. Such fish bones may not be detected on examination if this does not take place in a timely manner. Over time, mucosal ulcers or purulent cysts may form locally. With the loss of necrotic tissue in the ulcer or the rupture of the purulent cyst, the fish bone may be expelled from the mucosa. CT has been found to be useful for the evaluation of patients with suspected pharyngoesophageal foreign bodies, because it can be performed rapidly and generates diagnostically useful coronal and sagittal images that can be used to prepare a 3-D reconstruction. 5
We think that the present case is interesting because the patient is the only one in whom we have identified pathological changes caused by a small fish bone. The patient mistakenly swallowed a small fish bone when eating, but she continued to eat normally. One week later, she underwent electronic fiber laryngoscopy, which did not reveal the tip of the foreign body but did reveal a cystic mass with a diameter of approximately 3 mm in the left epiglottic vallecula. Therefore, a thin-slice unenhanced CT scan was performed, which showed a high-density lesion at the corresponding location of approximately 2 mm in length. Subsequently, rupture of the purulent cyst permitted the discharge of the foreign body to occur. This case report describes the complete pathological process. Specifically, small foreign-body impaction occurred, a local purulent cyst formed and then ruptured, and the foreign body was expelled. Such a fish bone impaction and subsequent expulsion has not been previously reported to the best of our knowledge.
Conclusion
If small fish bones become impacted in the pharynx, a small abscess or purulent cyst may form locally in the mucosa, which may then rupture spontaneously, with the foreign body then being discharged from the body. This represents one way in which an impacted small foreign body may be discharged from the body, and this knowledge could be used to reassure anxious patients and teach medical students.
Supplemental Material
sj-jpg-1-imr-10.1177_03000605231187947 - Supplemental material for Delayed pathological finding of a small fish bone causing a purulent cyst in the pharynx: a case report
Supplemental material, sj-jpg-1-imr-10.1177_03000605231187947 for Delayed pathological finding of a small fish bone causing a purulent cyst in the pharynx: a case report by Xiao Shufen, Zhang Juan, Wang Ling and Dong Fangru in Journal of International Medical Research
Supplemental Material
sj-jpg-2-imr-10.1177_03000605231187947 - Supplemental material for Delayed pathological finding of a small fish bone causing a purulent cyst in the pharynx: a case report
Supplemental material, sj-jpg-2-imr-10.1177_03000605231187947 for Delayed pathological finding of a small fish bone causing a purulent cyst in the pharynx: a case report by Xiao Shufen, Zhang Juan, Wang Ling and Dong Fangru in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
Written informed consent was obtained from the patient for their anonymized information to be published in the article. Ethics approval to report this case was obtained from the Ethics Committee Of Bethune International Peace Hospital (approval number: 2020-KY-44).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.