
Abstract
Carcinosarcoma is a rare malignant neoplasm comprising both epithelial and mesenchymal components. Hepatoid adenocarcinoma (HAC) is another rare type of cancer. To date, there are only four reported cases of concurrent carcinosarcomas with HAC across all tumor types, all of which were observed in uterine tumors. Here, we report an unusual case of gastric carcinosarcoma associated with alpha-fetoprotein (AFP)-producing HAC in a 76-year-old woman. Upon admission, the patient had an elevated serum AFP concentration (448 µg/L), a necrotic polypoid tumor of the central gastric cardia revealed by endoscopy, and no evidence of distant metastasis indicated by computed tomography (CT). Owing to malignancy indicated by biopsy, the patient underwent proximal subtotal gastrectomy. The resected tumor was composed of both an HAC component and a sarcoma component, microscopically. The sample was positive for AFP, hepatocyte paraffin (Hep-Par) 1, glypican-3, SALL4, CDX2, cytokeratin (CK) (pan), CK18, desmin, and vimentin staining immunohistochemically. In summary, the tumor was diagnosed as carcinosarcoma of the stomach with AFP-producing HAC. To our knowledge, this is the first report of gastric carcinosarcoma with AFP-producing HAC in the English literature describing gastric tumors.
Keywords
Introduction
Hepatoid adenocarcinomas (HACs) are extrahepatic tumors that resemble hepatocellular carcinomas and that produce alpha-fetoprotein (AFP). 1 , 2 HACs have been found in different organs, namely the lungs, 3 pancreas, 4 ampulla of Vater, 5 esophagus, 6 colon, 7 renal pelvis, 8 urinary bladder, 9 uterus, 10 and ovaries. 11 In 1985, Ishikura et al. first proposed the term “hepatoid adenocarcinoma” to describe primary gastric carcinoma. 1 HAC of the stomach accounts for only 0.3% to 1% of all gastric adenocarcinomas,12–14 and has a poor prognosis, 15 with an average survival time of 10 to 18 months.16–18
Carcinosarcoma of the stomach is an extremely rare biphasic tumor consisting of both carcinomatous and sarcomatous components. 19 Nie et al. estimated that carcinosarcoma accounts for only 0.05% of all radically resected gastric cancers. 20 Immunohistochemistry is the gold standard for diagnosing carcinosarcoma. 21 However, therapeutic data for the cancerous components of gastric carcinosarcoma with HAC differentiation are limited because of the low incidence.
In the present study, we report a case of carcinosarcoma of the stomach with AFP-producing HAC. This is the first case of cancerous components of gastric carcinosarcoma with HAC differentiation. This case expanded the spectrum of the heterogeneity of gastric cancer and raised therapeutic challenges because of the combination of two subtypes of gastric cancer known for their rarity and poor prognosis. The reporting of this study conforms to the CARE guidelines. 22
Case report
A 76-year-old woman with a 2-month history of epigastric pain was admitted to the Department of Surgical Oncology of the First Affiliated Hospital of Zhejiang University. Physical examination was unremarkable other than the finding of epigastric pain. Initial laboratory examination showed low plasma albumin (ALB) concentration (27.1 g/L; reference range: 35–50 g/L) and elevated serum AFP concentration (448 µg/L). Other routine serum parameters and tumor makers were unremarkable.
Endoscopic examination revealed a polypoid tumor (6 cm × 5 cm) with central necrosis at the cardia of the stomach (Figure 1). A malignant gastric tumor was suspected according to the pathological analysis of the biopsy. Computed tomography revealed a mass (6.1 cm × 3.6 cm) near the lesser curvature of the stomach, and no abnormalities were found in the liver and bile ducts (Figure 2).
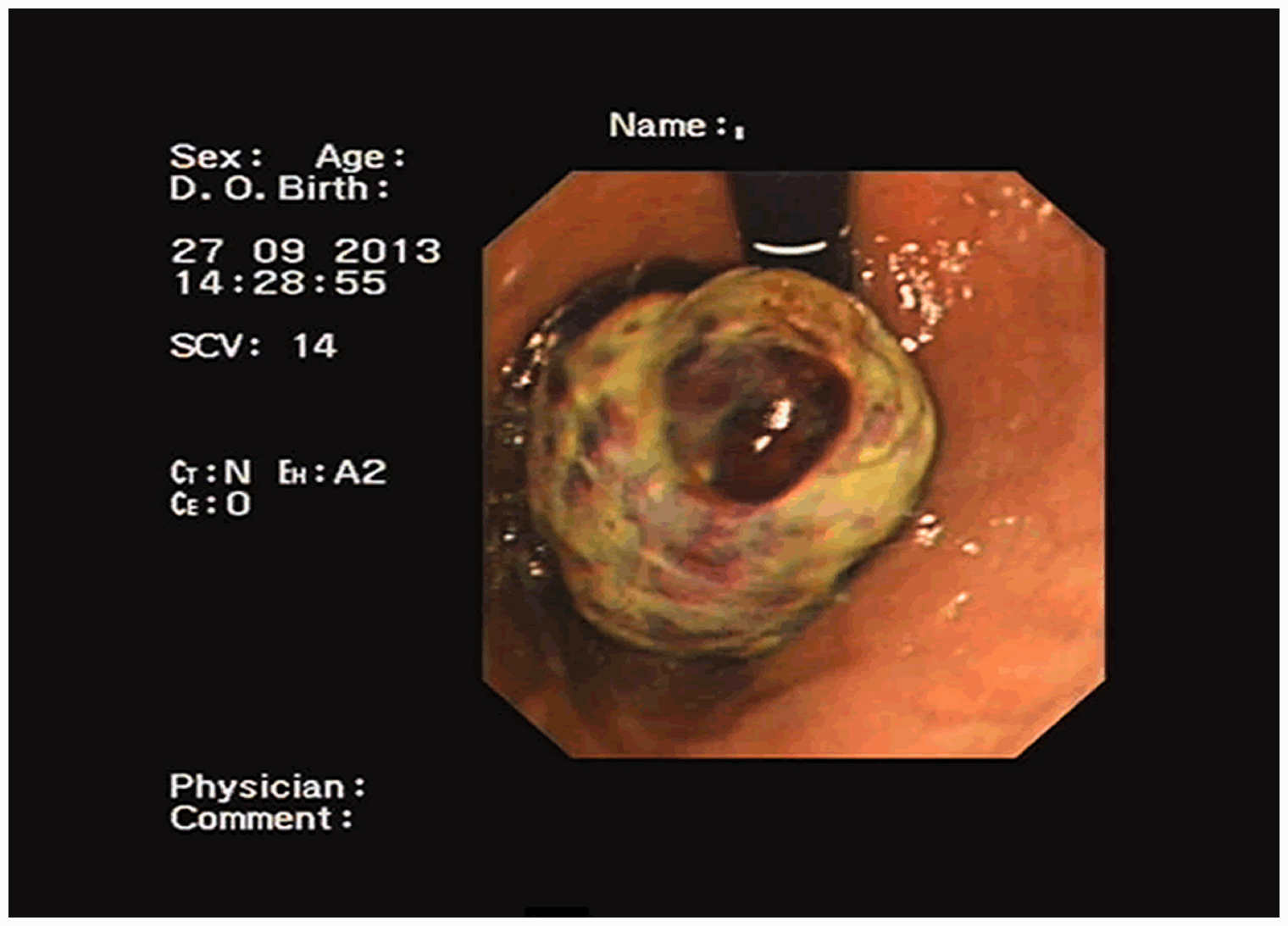
Endoscopy showing a polypoid mass with central necrosis at the cardia of the stomach.
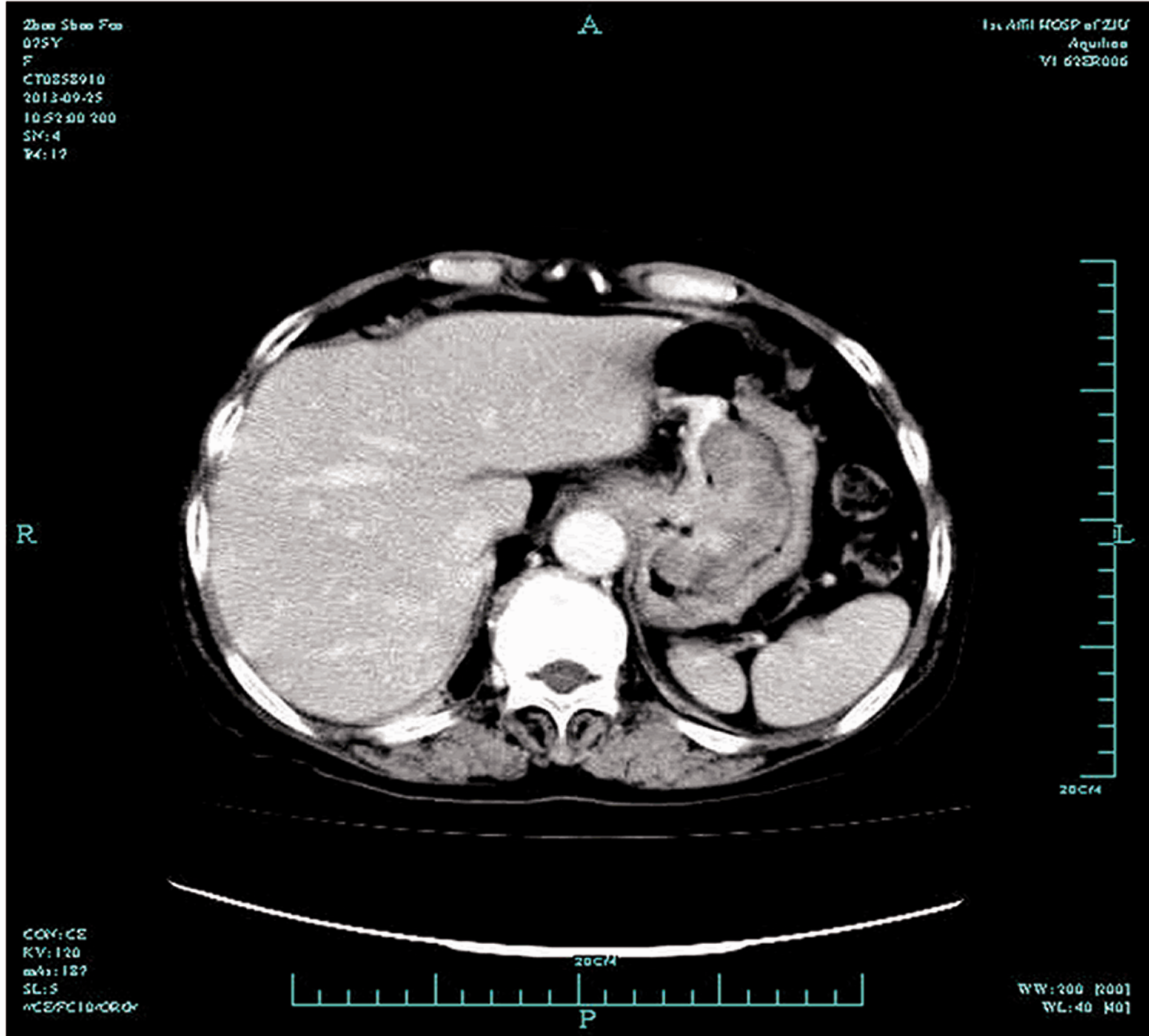
Abdominal computed tomography (CT) scan showing a mass (6.1 cm × 3.6 cm) near the lesser curvature of the stomach.
The patient subsequently underwent proximal subtotal gastrectomy. Macroscopically, an ulcerative polypoid tumor (5 cm × 3.5 cm × 2.5 cm) arising from the cardia of the stomach was observed. Microscopically, the tumor was composed of carcinomatous and sarcomatous components (Figure 3a). The mesenchymal component consisted of fascicles of spindle-shaped cells and numerous large, rounded, oval cells with hyperchromatic nuclei and occasional eosinophilic cytoplasm (Figure 3b). Cartilage-like cells and cartilage lacuna-like structures were also observed (Figure 3c). The carcinomatous component was a poorly differentiated or undifferentiated gastric adenocarcinoma with trabecular hepatoid cells arranged in sheets and cords with a hepatoid appearance (Figure 3d). The tumor infiltrated the submucosa of the stomach with no sign of metastases in the dissected lymph nodes. Immunohistochemical analysis showed positive staining for epithelial markers (pan-cytokeratin (CK) and CK-18), mesenchymal markers (vimentin, desmin), and a gastrointestinal differentiation marker (CDX2) (Figure 4a–e). The hepatoid-differentiated adenocarcinoma was positive for AFP, hepatocyte-paraffin (Hep-Par) 1, glypican-3, and SALL4 (Figure 4f–i). The tumor was pathologically diagnosed as carcinosarcoma of the stomach with AFP-producing HAC. Moreover, 1 week after the operation, the serum AFP concentration decreased to 27 µg/L.

Hematoxylin & eosin (HE) staining of the tumor tissue. a, Tumor showing a mixture of carcinomatous and sarcomatous components; poorly differentiated or undifferentiated carcinoma is seen; b, Specimen showing the presence of atypical spindle-shaped cells, and large, rounded, oval cells; c, Specimen showing cartilage-like cells and cartilage lacuna-like structures in part of the tumor; d, tumor arranged in sheets and cords with a hepatoid appearance. Tumor cells possess eosinophilic cytoplasm and markedly atypical nuclei.
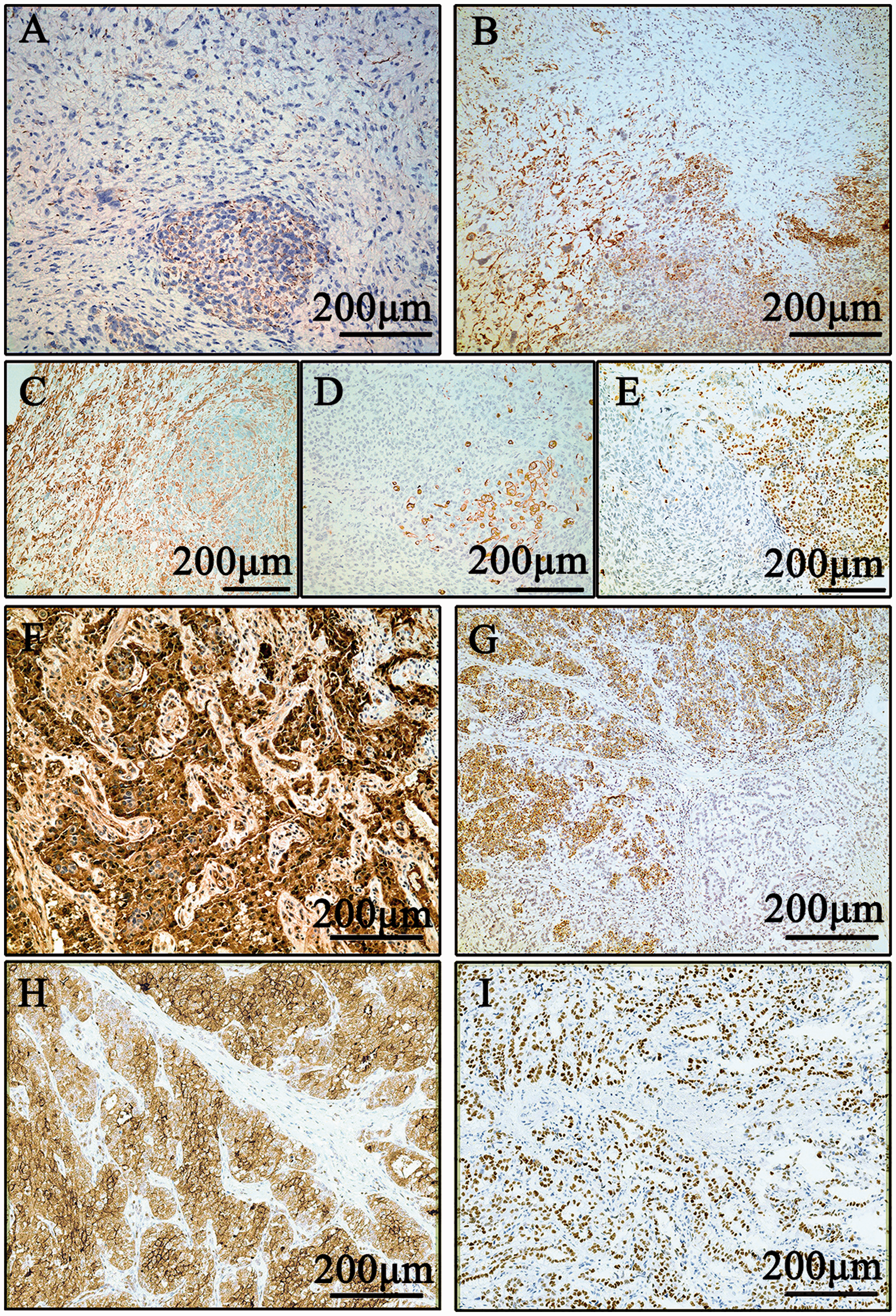
Immunohistochemical staining of the tumor tissue. a–i, Immunohistochemical staining for pan-cytokeratin (CK), CK-18, vimentin, desmin, CDX2, alpha-fetoprotein (AFP), hepatocyte-paraffin (Hep-Par) 1, glypican-3, and SALL4, respectively. Immunodetectable protein is indicated by brown staining; nuclei are counterstained blue.
No chemotherapy was administered owing to the patient’s poor general condition and that she and her family refused adjuvant therapy. The patient died of tumor metastasis 8 months after the gastrectomy.
Discussion
HAC of the stomach (HAS) is a type of gastric cancer that morphologically mimics hepatocellular carcinoma and which has a poor prognosis. 1 , 15 In 1985, Ishikura et al. proposed the term “hepatoid adenocarcinoma” for primary gastric carcinoma with features of hepatic differentiation and AFP production. 1 However, Nagai et al. (1993) reported that microscopically, HAS showed hepatoid features without AFP-staining. 23 Therefore, the diagnosis of HAS was not dependent on AFP production but rather on hepatic differentiation. Additionally, higher preoperative serum AFP concentration (≥500 µg/L) is associated with worse overall survival (OS) and disease-free survival (DFS) in HAS patients. 24
Carcinosarcoma is a rare biphasic tumor, defined by the World Health Organization (WHO) as “a malignant tumor composed of intimately mixed epithelial and mesenchymal elements of a type ordinarily found in malignancies of adults”. 25 The clinical symptoms and laboratory, endoscopic, and radiological findings of carcinosarcoma of the stomach are generally indistinguishable from gastric adenocarcinomas. Therefore, its diagnosis largely relies on pathological analysis, such as cell morphology and immunocytochemical staining. In our case, microscopic examination revealed both carcinomatous and sarcoma components. The carcinomatous component was arranged in sheets and cords with a hepatoid appearance, while the sarcoma components showed spindle-shaped cells and a cartilage lacuna-like structure. Furthermore, immunohistochemical results were positive for epithelial markers (pan-CK and CK18) and mesenchymal markers (vimentin and desmin) but negative for S100, cluster of differentiation (CD)34, CD117, and DOG-1 (data not shown). Considering the positive AFP staining of the tumor and the elevated preoperative serum AFP concentration (448 µg/L), the pathological analysis led to the final diagnosis of carcinosarcoma of the stomach with AFP-producing HAC.
Carcinosarcoma typically occurs in the uterus, breast, and lung, and rarely in the stomach. 21 The first case of carcinosarcoma of the stomach, or gastric carcinosarcoma, was described by Queckenstedt in 1904,26,27 and to date, only 84 cases have been reported. 20 ,28–32 Gastric carcinosarcomas occur predominantly in the male population and mainly among those over 60 years of age.19,21 The gastric cardia, which was the tumor site in our case, is the most common site of gastric carcinosarcoma in Chinese patients (approximately 50%) but not in Japanese patients (only 19%). 20 A review of 80 cases of gastric carcinosarcoma by Nie et al. showed that the most common carcinomatous component is Lauren intestinal-type adenocarcinoma (53/80, 66%), followed by Lauren diffuse type (9/80) and neuroendocrine carcinoma (9/80, 11%). 20 Our case is the first carcinosarcoma in the stomach with HAC as its carcinomatous component. To date, there have been only four cases of carcinosarcoma associated with HAC across all tumors, and all were in the uterus.33–35
Epithelial–mesenchymal transition (EMT) has been reported to be closely related to the development of carcinosarcoma. In EMT, epithelial cells lose shape and function and gradually transform into mesenchymal-like cells. Carcinosarcoma presents two morphological manifestations histologically, namely adenocarcinoma and sarcoma. The boundary between the two is clear, and there is no transition zone. CK is positive in cancer tissue, and vimentin is negative, while CK is negative in sarcoma tissue and vimentin is positive. Regarding EMT of adenocarcinoma, there is often a histological transition zone between the cancer and the sarcoma. The tumor cells in this zone have an intermediate morphology and a phenotype indicating epithelial and mesenchymal cells (double-positive for CK and vimentin), with CK expression in the cells in the sarcoma. In our case, these two components (adenocarcinoma and sarcoma) were not separated by a clear boundary or an obvious transition zone. We consider that the tumor tissue in this patient showed both sarcoma-like differentiation and cancer-like differentiation, with positive epithelioid markers (pan-CK, CK-18) and mesenchymal markers (vimentin, desmin). However, there was sufficient evidence to rule out the possibility of EMT in this case.
Therapeutic data for both carcinosarcoma and HAC in the stomach are minimal owing to the rarity. Most cases of gastric carcinosarcoma were diagnosed at locally advanced stages owing to the rapid progression. 28 In our case, the tumor was confined to the submucosa, and the pathological tumor-node-metastasis (pTNM) stage was T1bN0M0. To date, only four cases (excluding our case) of gastric carcinosarcoma confined to the submucosa have been reported, and these were reviewed by Kuroda et al. 28 Interestingly, all four cases were from Japan. 28 Radical gastrectomy is considered the only curative treatment for gastric carcinosarcoma. 28 However, the prognosis of gastric carcinosarcoma patients after radical gastrectomy is poor, and the estimated mean postoperative survival is only 7 to 10 months. Furthermore, more than 50% of cases develop reoccurrence in the first postoperative year.35–37 Chemotherapy and radiotherapy have been reported in a few case reports; 37 , 38 however, the prognosis was still poor. Regarding HACs of the stomach, the tumor is treated similarly to common gastric adenocarcinoma, but only a few cases of effective chemotherapy 39 , 40 and radiotherapy 41 have been reported. In our case, the patient refused any further treatment after surgery; therefore, no information regarding the patient’s response to adjuvant therapy was available.
Although therapeutic data for HAS and gastric carcinosarcomas are limited, researchers have investigated their molecular characteristics, which might shed light upon potential targeted therapies. Targeted gene sequencing of 42 HAS tumors revealed that copy number gain of 20q11.21–13.12 frequently occurs (50%) in HAS and might be associated with more adverse biobehavior. 24 In addition, mutation analysis revealed that TP53 (30%) is the most frequently mutated gene in HAS, followed by CEBPA (22%) and RPTOR (13%). No specific gene alteration has been reported to date for carcinosarcoma in the stomach. For rare gastric cancers with a poor prognosis, we propose that patient-derived human tumor xenograft (PDTX) models might have great potential for optimizing adjuvant therapy. PDTX models closely retain the histopathologic, genetic, and phenotypic features of the original clinical cancer, which offer a powerful tool for studying tumor biology and evaluating anticancer drugs. 42 We are currently developing PDTX models of AFP-producing gastric cancer and are exploring appropriate therapeutic strategies for this subtype of gastric cancer.
In conclusion, we have described the first case of gastric carcinosarcoma with AFP-producing HAC in the English literature describing gastric tumors. Pathological and immunohistochemical analyses are essential for diagnosing this subtype of gastric cancer. This rare gastric cancer subtype lacks practical therapeutic approaches and is associated with a poor prognosis. PDTX models should be used to facilitate the discovery of appropriate therapeutic strategies for this rare subtype of gastric cancer.
Footnotes
Acknowledgments
The authors thank Runnan Xu, Jiaying Ruan, Hao Xie, Haohao Wang, and Haiyong Wang for assistance with the data analysis. The authors greatly thank all the staff and assistants in the Department of Surgical Oncology, the First Affiliated Hospital, Zhejiang University School of Medicine for their support in collecting samples.
Authors' contributions
LST and ZQL conceived and designed the study and wrote the manuscript. JL, QZ, and HBZ collected and analyzed the data, and LST, ZQL, and HBZ contributed to writing the manuscript. Both LST and ZQL read and approved the final manuscript.
Availability of data and materials
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The present study was performed in accordance with the First Affiliated Hospital, Zhejiang University School of Medicine Human Research Ethics protocol (Approval No.: 2018-309). Written consent was obtained for the publication of this case report and any accompanying images. A copy of the written consent is available for review on reasonable request.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.