
Abstract
Objective
To identify the clinical features and prognostic factors for sublingual gland carcinoma.
Methods
This was a case–control study. Patients with surgically treated sublingual gland carcinoma were retrospectively included in the Surveillance, Epidemiology and End Results database and divided into adenoid cystic carcinoma (ACC) and non-ACC groups. Primary outcome variables were disease-specific survival (DSS) and overall survival (OS). Prognostic factors for each group were analyzed using Cox models.
Results
We included 251 patients (115 men and 136 women). Compared with the non-ACC group, the ACC group had a larger average tumor size and received more adjuvant radiotherapy. In patients with ACC, the pathologic grade had an independent impact on DSS and OS, and patients who were undergoing adjuvant chemotherapy had worse DSS than those who were not receiving chemotherapy. In the non-ACC group, pathologic grade IV, lymph node metastasis, and adjuvant chemotherapy were associated with poor DSS and OS, and tumor extension predicted worsening DSS.
Conclusions
In sublingual gland carcinoma, the pathologic grade and adjuvant chemotherapy were the most important prognostic factors, whereas lymph node metastasis had a negative impact in non-ACC patients but not in ACC patients.
Keywords
Introduction
Salivary gland carcinoma accounts for approximately 5% of all head and neck cancers. 1 The carcinoma affects major or minor salivary glands; the sublingual gland is the least likely organ to be involved. 2
Reports of salivary gland carcinoma are limited given the rarity of the disease.3–12 Yu et al. 3 described 28 cases that were identified within 60 years in a famous medical center in China. Zdanowski et al. 4 studied 12 cases at the Brazilian National Cancer Institute, whereas Kojima et al. 5 described 12 patients in 12 Japanese medical institutions. These studies have reported inconsistent findings regarding lymph node metastasis, and the prognostic factors remain unclear. Additionally, the small scale of these studies diminishes the credibility of their conclusions. Park et al. 11 noted local invasion in 80% of 26 patients that was associated with decreased OS and disease-specific survival (DSS). Wu et al. 12 recently confirmed the impact of tumor stage on survival. Lee et al. 13 analyzed 210 patients in the Surveillance, Epidemiology, and End Results (SEER) database and demonstrated the prognostic roles of age, sex, stage, and surgery. However, the authors neglected several crucial factors including tumor extension and adjuvant treatment. Most importantly, all of these studies failed to analyze the impact of the pathologic type on prognosis. Adenoid cystic carcinoma (ACC) is the most common malignancy in the sublingual gland and shows inconsistent biological behaviors compared with the other types of carcinoma; ACC may therefore have different prognostic factors.
Therefore, this study identifies the clinical features and prognostic factors for sublingual gland carcinoma stratified by pathologic type.
Patients and methods
Patient selection
This was a case–control study, and the reporting of this study conforms to the STROBE guidelines. 14 All data were obtained from the SEER database, which provides information on cancer statistics to help reduce the cancer burden among the population of the United States. 15 The patients in the database had undergone surgical treatment for sublingual gland carcinoma between 1975 and 2019. The patients with primary epithelial disease were included; however, patients who lacked information on detailed surgical procedures or follow-up were excluded. Information on demographic characteristics, time to surgery (TTS), histological grade, tumor extension, treatment, and follow-up was extracted and analyzed.
Ethical approval was not required given that the data are accessible to the public.
Definitions of variables
The patients were divided into low- and high-risk groups based on the risk stratification criteria formulated by the World Health Organization. 16 Tumor size was determined based on collaborative stage tumor size (2004–2015), EOD 10-size (1988–2003), and EOD 4-size (1983–1987). Baseline neck status was analyzed in accordance with the derived EOD classification, the derived AJCC classification, the derived SEER combined classification, regional nodes examined (1988+), regional nodes positive (1988+), and the scope of regional lymph node surgery (2003+). Distant metastasis was determined based on the derived EOD classification, derived AJCC classification, and derived SEER combined classification. Tumor extension was defined as extracapsular and perineural invasion and was evaluated based on collaborative stage extension (2004–2015), EOD 10-extent (1988–2003), and EOD 4-extent (1983–1987). 17 TTS was defined as the duration between diagnosis and surgery.
Statistical analysis
The study population was divided into two groups (ACC and non-ACC), and demographics and pathology were compared between the two groups. The main endpoints were DSS and OS. DSS time was calculated from the date of surgery to the date of cancer-related death or last follow-up. OS time was calculated from the date of surgery to the date of any-cause death or last follow-up. Univariate and multivariate Cox analyses were used to determine the prognostic factors for DSS and OS. All statistical analyses were performed using the Statistical Package for the Social Sciences 20.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at p < 0.05.
Results
Baseline data
We included 251 patients (115 [45.8%] men and 136 [54.2%] women; mean age: 59 ± 14 years). Overall, 77.7% of the patients were White, and most patients were married and urban dwellers. The most common histologic type was ACC (40.6%). Forty-nine (19.5%), 105 (41.8%), 33 (13.1%), and 18 (7.2%) cancers were classified as grades I, II, III, and IV, respectively. Tumor size > 3 cm and neck lymph node metastasis were observed in 74 (29.5%) and 28 (11.2%) patients, respectively. Distant metastasis was observed in 18 (7.2%) patients and tumor extension was observed in 103 (41.0%) patients. One hundred sixty-one (64.1%) patients underwent treatment and had a TTS < 1 month. One hundred thirty-nine (55.4%) and 21 (8.4%) patients received adjuvant radiotherapy and chemotherapy, respectively. After a mean follow-up period of 99 ± 86 months, 118 patients died; among these patients, 64 died of cancer (40 and 24 patients died of distant metastasis and locoregional recurrence, respectively).
The ACC and non-ACC groups had a similar distribution of age, race, sex, marital status, household income, living area, pathologic grade, risk stratification, lymph node metastasis, distant metastasis, adjuvant chemotherapy, TTS, and tumor extension (all p > 0.05). However, the ACC group had a significantly larger average tumor size (p = 0.004) and received significantly more adjuvant radiotherapy (p < 0.001; Table 1).
Baseline data of the 251 enrolled patients with sublingual gland carcinoma.

ACC: adenoid cystic carcinoma.
*p: comparison between ACC and non-ACC groups.
Predictive factors for DSS and OS in ACC
In the univariate analysis, pathologic grade, risk stratification, distant metastasis, adjuvant chemotherapy, and tumor extension were associated with DSS. In the multivariate analysis, compared with pathologic grade I, grades III (hazard ratio [HR]: 3.93; 95% confidence interval [CI]: 1.45–20.72) and IV (HR: 9.28; 95% CI: 1.89–45.64) were associated with an increased risk of cancer-related death. Patients who were undergoing adjuvant chemotherapy had significantly worse DSS than those who did not receive chemotherapy (p = 0.041; Table 2, Figure 1).
Univariate and multivariate Cox analyses of predictors for disease-specific survival in adenoid cystic carcinoma of the sublingual gland.

TTS: time to surgery, HR: hazard ratio.

Comparison of survival in adenoid cystic carcinoma patients with differing clinical features. (a) disease-specific survival (DSS) based on pathologic grade; (b) DSS based on adjuvant chemotherapy; and (c) overall survival (OS) based on pathologic grade.
In the univariate analysis, age, pathologic grade, risk stratification, distant metastasis, adjuvant chemotherapy, and tumor extension were associated with OS. However, in the multivariate analysis, only pathologic grade was independently associated with OS. In contrast to pathologic grade I, grade II (p = 0.839) did not alter the risk of overall death; however, grades III (HR: 3.86; 95% CI: 1.95–15.66) and IV (HR: 6.74; 95% CI: 1.67–27.28) predicted worse OS compared with grade I (Table 3, Figure 1).
Univariate and multivariate Cox analyses of predictors of overall survival in adenoid cystic carcinoma of the sublingual gland.
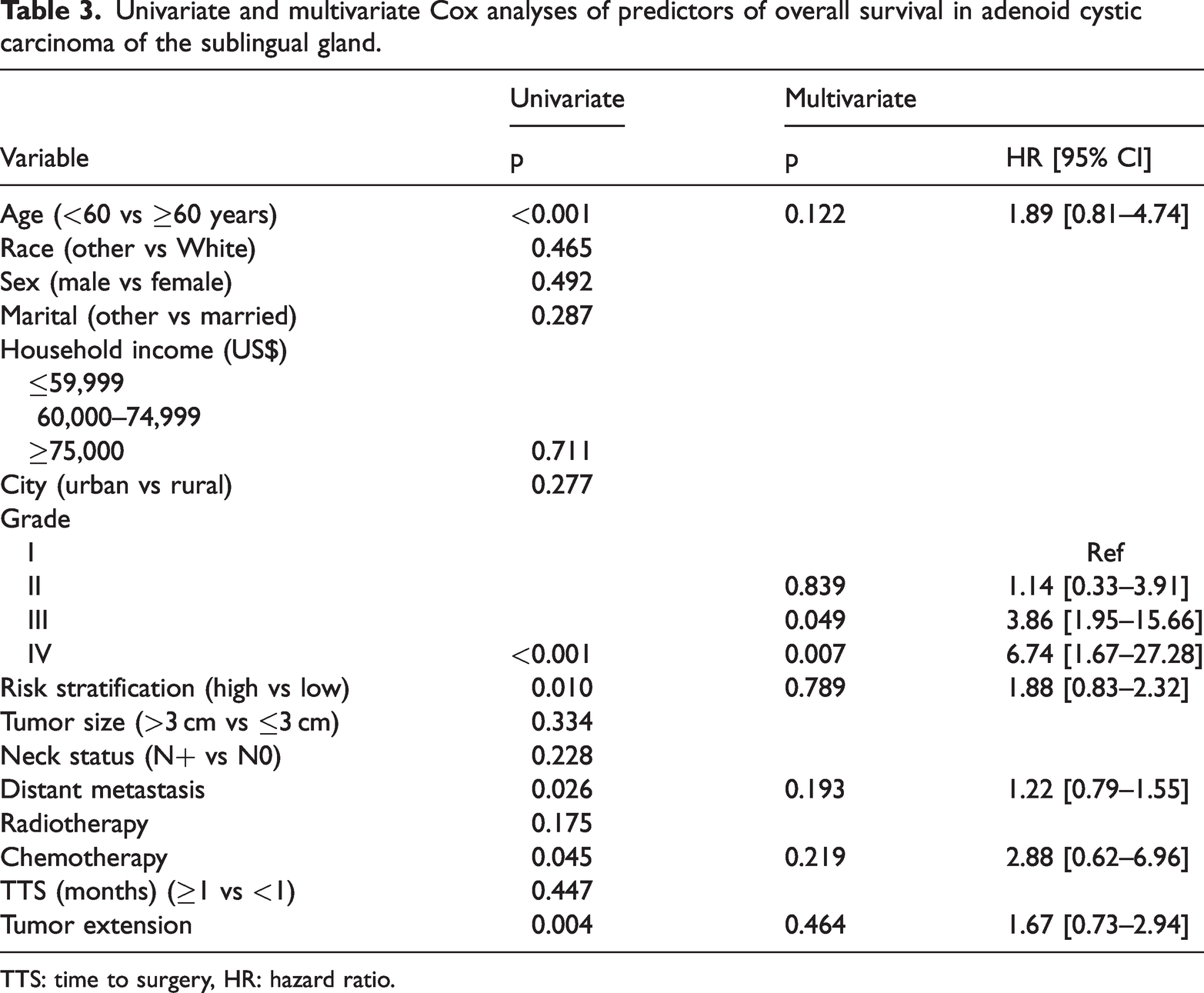
TTS: time to surgery, HR: hazard ratio.
Predictive factors for DSS and OS in non-ACC
Pathologic grade, risk stratification, tumor size, lymph node metastasis, distant metastasis, adjuvant chemotherapy, and tumor extension were included as factors in the Cox analysis. Pathologic grade IV (HR: 42.39; 95% CI: 4.84–371.04), lymph node metastasis (HR: 4.86; 1.90–19.37), adjuvant chemotherapy (HR: 1.89; 95% CI: 1.02–4.32), and tumor extension (HR: 1.97; 95% CI: 1.14–3.97) were independently associated with DSS (Table 4, Figure 2).
Univariate and multivariate Cox analyses of predictors of disease-specific survival in non-adenoid cystic carcinoma of the sublingual gland.
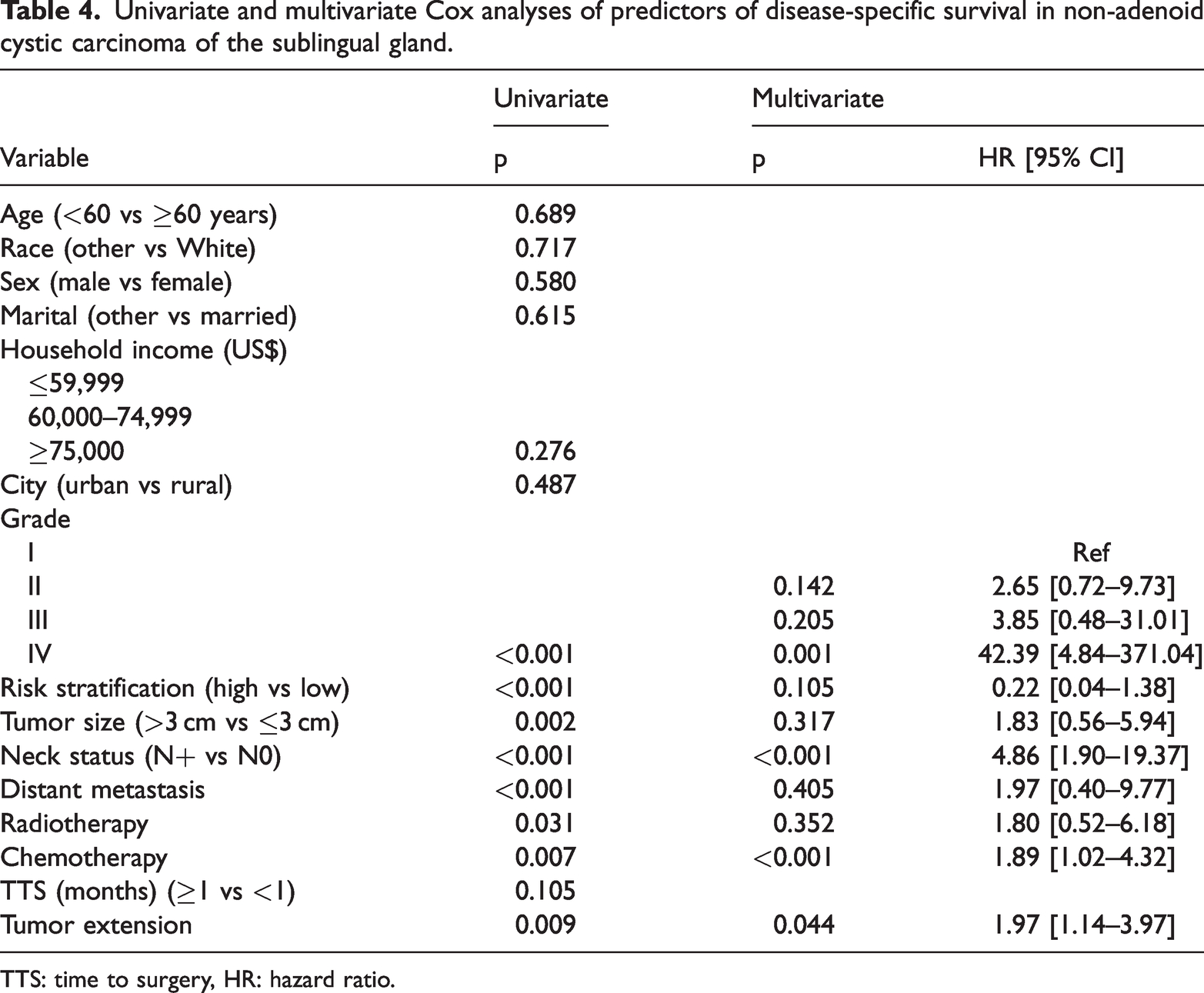
TTS: time to surgery, HR: hazard ratio.

Comparison of disease-specific survival (DSS) in non-adenoid cystic carcinoma patients with differing clinical features based on (a) adjuvant chemotherapy; (b) tumor extension and (c) pathologic grade; and (d) lymph node metastasis.
The multivariate analysis confirmed the independence of pathologic grade IV (HR: 29.32; 95% CI: 3.75–229.23), lymph node metastasis (HR: 2.89; 95% CI: 1.78–89.67), and adjuvant chemotherapy (HR: 2.16; 95% CI: 1.05–7.47) in predicting OS (Table 5, Figure 3).
Univariate and multivariate Cox analysis of predictors for overall survival in non-adenoid cystic carcinoma of the sublingual gland.

TTS: time to surgery, HR: hazard ratio.

Comparison of overall survival (OS) in non-adenoid cystic carcinoma patients with differing clinical features based on (a) adjuvant chemotherapy; (b) pathologic grade and (c) lymph node metastasis
Discussion
To the best of our knowledge, our study had the largest sample size among relevant studies. In patients with sublingual gland carcinoma, pathologic grade and adjuvant chemotherapy were the most important prognostic factors for DSS and OS. Lymph node metastasis was relatively uncommon but had a negative impact on prognosis in the non-ACC group that was not observed in the ACC group. We demonstrated the presence of differing prognostic patterns in sublingual gland cancer that can be stratified by pathologic type—a finding that must be considered during clinical management.
Pathologic grade is a crucial prognostic factor for salivary gland carcinoma. Lukovic et al. 18 established a clinical prediction-score model for distant metastasis in major salivary gland carcinoma. In the model, high-grade histology yielded a better risk coefficient than pT3-4, pN+, positive margin, and lymphovascular invasion. Kaya et al. 19 reported that grades III/IV had a significant adverse effect on OS (HR: 2.5) and DSS (HR: 3.2) in patients who were diagnosed with acinic cell carcinoma of the major salivary glands. However, these two studies did not identify the exact number of sublingual gland carcinomas. Ali et al. 20 reported that patients with high-grade carcinoma of the major salivary glands were 7.5 times more likely to present with distant metastasis than patients with low- or intermediate-grade tumors. Moreover, the high-grade group had a significantly lower 5-year recurrence-free rate (42.5%) than the intermediate-grade (88.9%) and low-grade (95.9%) groups. 21 However, the sample included only five cases of sublingual gland carcinoma. Recently, Kusafuka et al. 22 reported that the primary site was significantly associated with survival, and outcomes were significantly worse when the primary tumor site was the minor/sublingual salivary glands than when it was the major salivary glands. This difference can be attributed to differences between sublingual and parotid/submandibular gland cancers; however, only one study has reported an association between disease grade and survival. Lee et al. 13 reported no correlation between high-grade tumors and worse survival in patients with sublingual gland carcinoma. These findings are inconsistent with those in our study, in which pathologic grade had a significant impact on DSS and OS independent of pathologic type. The inconsistency may be attributed to differences in the definitions of pathologic grade and calculation methods.
The treatment of sublingual gland carcinoma usually begins with surgery followed by radiotherapy (Supplemental Figure 1).8,11,23 However, further studies are warranted to elucidate the roles of elective neck dissection and adjuvant therapy.
The presence of high-grade pathologic type and advanced-stage cancer increases the likelihood of lymph node metastasis. 24 Neck dissection allows the accurate determination of the pathologic stage and informs prompt adjuvant therapy upon detection of positive lymph nodes. Furthermore, regional recurrence is more likely to develop in patients who do not undergo neck dissection than in those who have the surgery,25,26 indicating the utility of elective neck dissection. However, in case of an occult metastasis rate <20%, over-treatment resulting from routine neck dissection must be considered. 27 In our study, the neck lymph node metastasis rate was only 11.2%. Rates as low as 0% have been similarly reported by Zdanowski et al. 4 and Sun et al., 8 suggesting that neck dissection is not routinely required. Moreover, routine neck dissection, which is indicated based on location, tumor stage, histopathological characteristics, and pathological type, did not provide an additional survival benefit in patients with salivary gland carcinoma.10,27 We noted that lymph node metastasis had a negative effect on prognosis in the non-ACC group that was not observed in the ACC group. This result may be explained by findings that suggest that lymph node metastasis is very uncommon in ACC, and the presence of even one positive lymph node does not decrease survival. 28
Adjuvant therapy was a crucial supplemental intervention that ensured disease control. We observed that chemotherapy was associated with worse OS and DSS compared with radiotherapy, even in cases in which the specific regimens or courses of chemotherapy were unknown. A possible explanation for this result is that a large contributor to the frequent cause of death was distant metastasis, which was relatively common in ACC. The patients with ACC usually required chemotherapy. However, to decrease recurrence and metastasis, chemotherapy was administered more often to patients with cancers that had adverse pathologic features than patients with ACC. However, chemotherapy has a limited impact on patients with parotid tumors.29,30 In a study of 495 patients with salivary duct carcinoma, Osborn et al. 31 reported that chemotherapy was utilized in 5.4%, 35%, and 70.7% of patients in stages I–II, stages III–IVB, and metastatic disease groups, respectively. However, chemotherapy did not significantly improve OS. In contrast, a chemotherapy (carboplatin + paclitaxel) study in patients with advanced-stage salivary gland carcinoma found that, although the objective response rate differed with pathologic diagnosis, the overall response rate was 39% and the median OS time was 26.5 months. 32 Further studies are warranted to investigate the medication regimens of the patients in our study.
Tumor extension is an adverse pathologic feature that can predict local or regional infiltration growth. In our study, 40% of the patients showed tumor extension, which is consistent with the findings of previous reports. 10 ACC is the most common histologic type and is characterized by neural invasion. However, the sublingual gland is relatively small, and a tumor >3 cm can easily grow out of the capsule. The high rate of tumor extension can be attributed to the surgical protocol. Transoral resection may be performed for small tumors. However, the preservation of the ductal system must be considered; otherwise, excision of the ipsilateral submandibular gland is recommended. 33 For large tumors, en bloc resection is the common first option. Additionally, lingual nerve ablation is usually required to achieve a negative margin. Finally, mandibulectomy is necessary in case of tumor invasion.
This study has several limitations. First, the retrospective study design decreased the study’s statistical power. Second, we did not consider the margin status and treatment intent, which may have affected survival outcomes. Third, given that our results were based on a United States population, it remains unclear whether the findings are generalizable to other populations.
In conclusion, pathologic grade and adjuvant chemotherapy were the most important prognostic factors for DSS and OS in sublingual gland carcinoma. Furthermore, lymph node metastasis was relatively uncommon but had a negative impact on prognosis in the patients without ACC that was not observed in the patients with ACC.
Footnotes
Author contributions
Study design: GQ, LW, CL, QZ, ZA, JQ
Manuscript writing: GQ, LW, CL, QZ, ZA, JQ
Study selection: GQ, LW, CL, QZ, ZA, JQ
Data analysis: GQ, LW, CL, QZ, ZA, JQ
Study quality evaluation: GQ, LW, CL, QZ, ZA, JQ
Manuscript revision: GQ, LW, CL, QZ, ZA, JQ
The final manuscript was read and approved by all of the authors.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Data availability statement
All data generated or analyzed during this study are included in this published article, and the primary datasets are available from the corresponding author upon reasonable request.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.