
Abstract
Objective
Fasciocutaneous free flap based on the peroneal artery (boneless version) is an option in our practice for head and neck reconstruction. However, the associated donor-site morbidity has rarely been discussed. Thus, this study investigated the long-term patient-reported donor-site morbidity associated with peroneal flaps.
Methods
In this single-center, retrospective, observational study, 39 patients who underwent a free peroneal flap were enrolled. We evaluated donor-site morbidity with a modified questionnaire from Enneking et al. and Bodde et al.
Results
Patient-reported daily life limitation was relatively low (5/39; 12.9%). Donor-site morbidities, namely pain (4/39; 10.3%), sensory disturbance (9/39; 23.1%), and walking limitation (9/39; 23.1%) were reported; most were rated minimal in severity. Among patients with walking limitation, muscle weakness (3/39; 7.7%), ankle instability (6/39; 15.4%), and gait alternation (6/39; 15.4%) were reported. Six patients developed claw toe.
Conclusion
Balancing successful reconstruction and donor-site morbidity is challenging. This long-term patient-reported survey revealed that harvesting peroneal flaps resulted in minimal or minor donor-site morbidity with no obvious impacts on the patients’ daily quality of life. Although free radial forearm flaps and anterolateral thigh flaps are standard, free peroneal flaps have been proven reliable, with acceptable donor-site morbidity.
Keywords
Introduction
Microsurgical free flap reconstruction has become standard in reconstructive surgery following head and neck cancer ablation because of its superior results in restoring appearance and function. A cutaneous flap with perforators from the peroneal artery was first described in 1993. 1 At our institute, peroneal flaps (fasciocutaneous or myofasciocutaneous flap) have been standard for reconstructing soft tissue defects after ablative surgery, such as tongue and esophageal defects that require thin and pliable flaps, or through-and-through defects involving the mouth angle and lips that require complex designs and reliable multiple perforators.2–6 In other institutes, the radial forearm free flap (RFFF) and medial sural artery perforator (MSAP) flap have been alternatives for defects that require a thinner and more pliable flap. However, we prefer the peroneal flap for several reasons. The conspicuous scar on the forearm and the risk of affecting hand function are major drawbacks of the RFFF.7,8 The MSAP flap is more suitable than the RFFF for small or medium-sized defects (approximately 15 × 6 cm); however, the peroneal flap can provide a larger skin paddle for reconstructing more complex defects (≥20 × 8 cm). 9 Furthermore, the peroneal fasciocutaneous or myofasciocutaneous flap can be designed as a chimeric flap for the reconstruction of complex defects after tumor ablation in head and neck surgery because the flap can be easily separated into several components.2,10
Apart from the principle of “replace like with like,” donor-site morbidity influences flap selection. To date, long-term donor-site morbidity of the peroneal flap has rarely been described in previous studies. 11 Therefore, this study analyzed the long-term donor-site morbidity, namely pain/sensory deficits, wound-healing, movement, claw toe, cosmetic result, and limitations in activities of daily living, to verify the clinical applicability of the peroneal flap.
Materials and methods
All patients underwent tumor resection and free peroneal flap reconstruction between January 2016 and October 2018. As postoperative assessment, the patients were interviewed by telephone using an outcome survey questionnaire modified from those of Enneking et al. and Bodde et al., with permission (Table 1).12,13 The interviews were part of the routine postoperative follow-up evaluation for head and neck cancer at our institute, and we collected these data for further analysis. Each patient was enrolled for at least 1 year after the operation. We deidentified the patients’ details at the end of the study. This study conforms to the SRQR reporting guidelines. 14
Questionnaire evaluating donor-site outcomes of the free peroneal artery-based flap.

Surgical technique
The free peroneal fasciocutaneous flap was harvested by experienced reconstructive surgeons as previously described.5,6 Briefly, an incision was made at the posterior border, and the flap was raised by subfascial dissection. The lesser saphenous vein and sural nerve were persevered when the flap was harvested. The flexor hallucis longus (FHL) muscle was harvested if needed. The donor site was primarily closed or covered with a split-thickness skin graft, depending on the wound size. 6
Donor-site evaluation
Donor-site surveys after free peroneal flap transfer were completed using questionnaires modified from those of Enneking et al. and Bodde et al.12,13 The questionnaires were modified for telephone interviews in five categories: pain/sensory disturbance, wound condition, movement, claw toe, and limitations in activities of daily living (Table 1).12,13 Furthermore, we reviewed the patients’ medical charts to evaluate wound healing problems or reoperation owing to donor-site comorbidity. Wound complication was defined as any wound healing problem, such as wound dehiscence, wound infection, or skin graft loss, that required invasive treatment.
Ethics statements
The study protocol was reviewed and approved by the Institutional Review Board for Clinical Studies of the Kaohsiung Veterans General Hospital (IRB approval No.: KSVGH20-CT2-05). The authors declare that the procedures in this study were performed in accordance with the regulations established by the Clinical Research and Ethics Committee and the Helsinki Declaration of the World Medical Association. The need to obtain informed consent was waived by the Institutional Review Board for Clinical Studies of the Kaohsiung Veterans General Hospital.
Statistical analysis
The relationship between donor-site morbidities and potential risk factors, namely diabetes mellitus, hypertension, carotid artery disease, smoking, alcohol consumption, betel nut chewing, body mass index, flap width, flap height, and duration of tourniquet use, were examined using the χ2 test or Fisher's exact test, as appropriate. All statistical analyses were performed using SPSS version 20.0 statistical software (IBM Corp., Armonk, NY, USA). Normally distributed continuous data are expressed as mean± standard deviation. Numerical data are expressed as frequency and percentage. The Chi-square test or Fisher’s exact test was used, as appropriate, to perform intergroup comparisons.
Results
This study enrolled 39 patients (38 men and 1 woman; mean age: 54.6 ± 11.2 years) who completed the telephone interview (Table 2). The mean size of the skin paddle was 6.27 × 12.35 cm (range, 5 × 7 cm to 10 ×27.5 cm). Interviews were performed postoperatively after a mean follow-up of 28.7 months (28.7 ± 10.5 months). All donor sites were closed with a split-thickness skin graft.
Patient and flap characteristics.
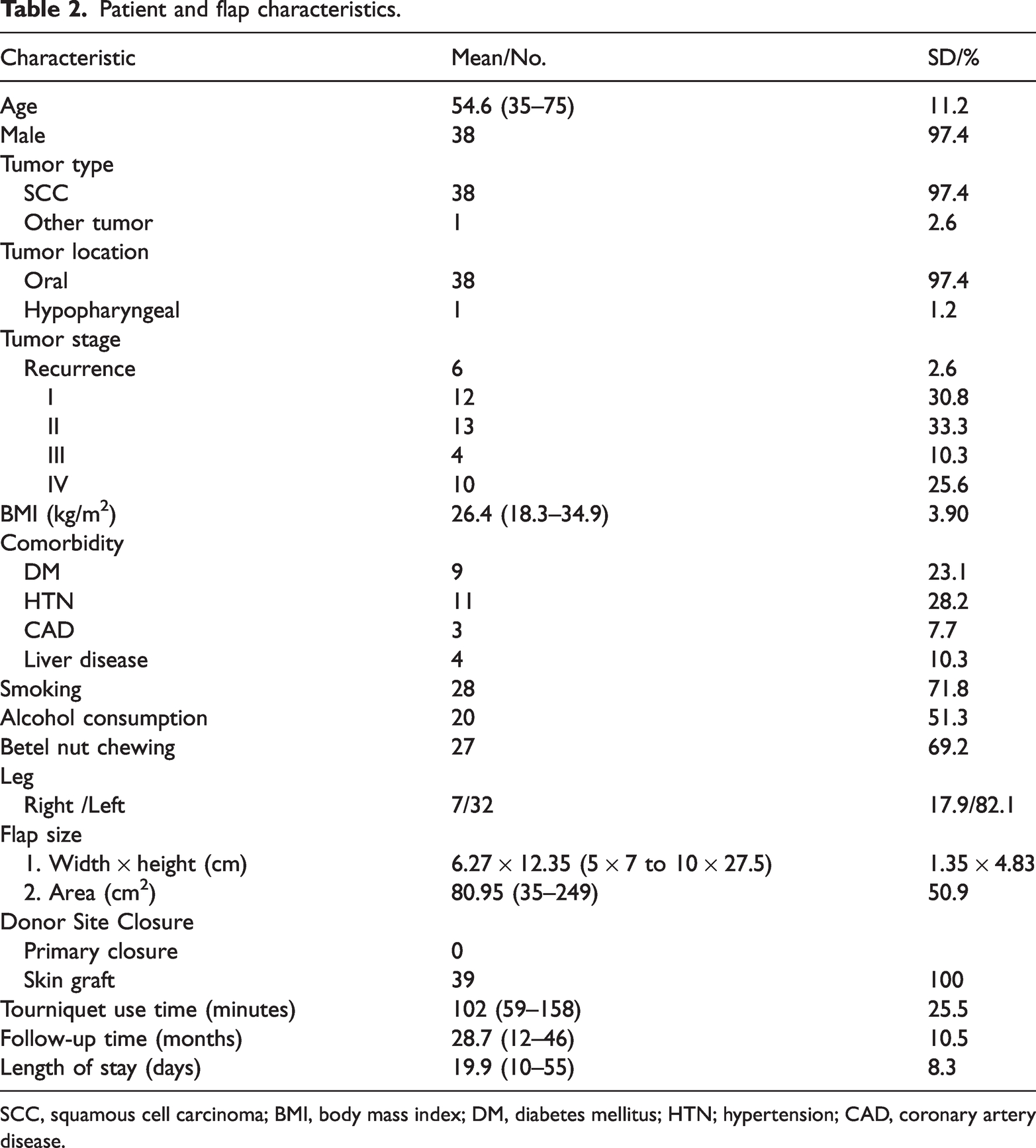
SCC, squamous cell carcinoma; BMI, body mass index; DM, diabetes mellitus; HTN; hypertension; CAD, coronary artery disease.
Overall, 33.9% of the patients complained of pain or sensory deficit at the donor site, namely mild pain (4/39; 10.3%), minimal sensory disturbance (7/39; 17.9%), and minor sensory disturbance (2/39; 5.1%). Among these patients, only one patient required occasional analgesics (Table 3).
Overall donor-site morbidity.

Except for one patient who rated the donor-site outcome as acceptable and still had a wound healing problem, 97.4% (38/39) of the patients rated the donor-site appearance of the peroneal flap as good after 2 years of follow-up (Figure 1). At the time of the telephone surveys, none of the patients complained of wound infection, edema, or hematoma (Table 3). According to the patients’ medical records, there were no wound complications that required invasive operation during the early postoperative follow-up. However, eight patients experienced partial skin graft loss (Figure 2); all wounds healed within 3 months without surgical intervention.

Patient with excellent wound healing.

Patient with partial skin graft loss.
The most common long-term complication associated with movement in our series was restricted running (8/39; 20.5%). Only two patients (2/39; 5.1%) required walking assistance (Table 3). Other long-term movement morbidities comprised ankle instability/stiffness (6/39; 15.4%), muscle weakness (3/39; 7.7%), and gait alteration (6/39; 15.4%). Six (6/39; 15.4%) patients developed claw toe, mostly in the big toe (Figure 3). Further investigation revealed that none of the patients complained of intolerable pain, metatarsalgia, or difficulty when wearing shoes or walking, and none requested surgical correction procedures, such as tenotomy or tendon lengthening. Despite these donor-site morbidity complaints, 87.2% (34/39) of the patients declared no limitations in their activities of daily living, and only one patient had a major limitation; i.e., difficulty climbing stairs.

Claw toe of the left big toe.
There were no statistically significant relationships between donor-site morbidities and potential risk factors.
Discussion
To the best of our knowledge, this is the first study to focus on the donor-site morbidity of a boneless version of the peroneal artery-based flap. The peroneal flap is a reliable choice in complex head and neck reconstructive surgeries.2–6 Issues regarding donor-site morbidity with peroneal flaps compared with other fasciocutaneous flaps, such as the anterolateral thigh flap or RFFF, are constantly debated among reconstructive surgeons. We used a patient-reported questionnaire rather than objective instrumental analysis because patient-reported outcomes can more accurately reveal the level of discomfort and impact of donor-site morbidities on patients’ daily lives.15,16
The questionnaire that we use evaluates five distinct domains of donor-site complications. In the pain/sensory domain, 4 (4/39; 10.3%) of the patients reported mild pain (occasional and not intense) after at least 1 year of follow-up. Only one patient required occasional analgesics. Donor-site pain rates after harvesting free fibular flaps range from 0% to 100%. 17 Other studies reported incidences of 7% to 21% for moderate pain, 18 43% for severe pain,18–20 and approximately 73% for persistent pain. 21 However, to the best of our knowledge, no previous report has described the prevalence of chronic pain after free peroneal flap harvest. The rate of chronic donor-site pain (4/39; 10.3%) in our study was consistent with rates in previous studies of donor-site wound pain after fibular flap harvest.17–21 This incidence was relatively lower than that in the free fibula flap groups in previous studies, indicating that preserving the fibula and surrounding muscle attachment of the lower leg reduced the development of postoperative pain, especially ankle pain or pain after prolonged walking.17,22
Patient-reported outcome evaluation provides valuable subjective feedback that reflects a patient’s actual experience and unmet needs. Understanding these complaints is helpful for surgeons to prevent nerve injury and improve the patient’s quality of life. Minimal and minor sensory disturbance was reported in 9 (9/39; 23.0%) patients in this study. The previously reported rate of sensory disturbance after fibula flap harvest ranged from 5.7% to 36%;18,23,24 our results were similar. This implies that harvesting a peroneal flap does not increase the incidence of nerve complications. Sensory disturbance usually occurred due to accidental injury to the sural nerve or superficial peroneal nerve during elevation of the cutaneous part of the flap. The fibula or peroneal flap procedure was almost identical during cutaneous elevation, leading to similar outcomes.
The free peroneal artery-based flap is a common alternative for head and neck soft tissue reconstruction worldwide; however, the optimal wound closure method for the donor site remains controversial. 25 Delayed wound healing is the most frequently reported early donor-site complication with the free fibula flap. Donor-site wound complications comprise wound dehiscence, infection, and loss of the skin graft, and the reported incidence of delayed wound healing is 2% to 38%.11,17 The risk of delayed healing and dehiscence increases as tension on the closure increases. 25 The size recommendation for primary closure of the donor site varied from 3 cm to 6 cm in previous studies.26–28 Shindo et al. stated that the width of the skin paddle alone is not a reliable parameter for determining the need to place a skin graft at the donor site. 29 Primary closure tended to result in a higher rate of wound complications compared with split-thickness skin grafting owing to increased tension. 29 Skin paddle location, operative time, muscle edema, harvested fibular length, and follow-up time are also crucial factors related to delayed donor wound healing. 30 Only one (1/39; 2.6%) patient in our study complained of minimal wound problems postoperatively. However, according to the patients’ medical records, 8 (8/39; 20.5%) patients experienced delayed donor wound healing 3 months postoperatively. In our study, regarding the peroneal flap, all donor sites were closed with skin grafts to ensure tension-free closure and to avoid delayed wound healing or compartment syndrome caused by excessive tension. 30 A distally located skin paddle, muscle edema (prolonged time elapsed after flap elevation to the end of head and neck tumor excision), and a large flap width (average width: 6.3 cm) were the major reasons for selecting skin grafting as the method of wound closure in our series. The incidence of delayed wound healing was much lower in our series compared with that in previous reports because all donor wounds were well-prepared and closed tension-free.
The peroneal flap, a boneless version of the peroneal artery-based flap, preserves the fibula during flap elevation. In our study, 8 (8/39; 20.5%) patients reported minor running restriction, and 1 (1/39; 2.6%) patient experienced difficulty climbing stairs. Among our patients, there were also complaints of muscle weakness (3/39; 7.7%), ankle instability (6/39; 15.4%), and gait alternation (6/39; 15.4%). The surgical procedure for peroneal flap elevation was described in our previous studies.2,4 Briefly, the FHL muscle was detached from the fibula, and isolation of the peroneal artery may cause muscle devascularization, which results in muscle weakness. 6 True ankle instability occurs when the distal end of the fibula is shorter than 6 cm to 8 cm, or less than 10% of the total fibular length. 31 Because the fibula remains intact after peroneal flap harvest, the sensation of ankle instability likely results from muscle fatigue or weakness after repetitive use, rather than actual ankle joint instability. 24 Peroneal artery isolation, which causes FHL muscle devascularization, is performed using the same procedure in both free fibula flap and peroneal flap (boneless version) harvesting. We routinely harvest the FHL muscle with the peroneal cutaneous flap at our institute. Anatomically, the FHL muscle is responsible for plantar flexion and inversion of the foot, and limited plantar flexion of the ankle may affect gait. 32 Lee et al. indicated that peak plantarflexion in the swing phase decreased significantly after fibula flap harvest. 33 We believe that plantar flexion can also be affected after harvesting the peroneal flap. Furthermore, abnormal gait can also result from pain. 34 Patients may adjust their gaits to prevent loading force at the area of pain, such as slowing their walking speed. 35
Claw toe deformity is another problematic morbidity resulting from loss of insertion, fibrosis, or ischemic contracture of the FHL during flap harvest.35,36 The incidence of claw toe deformity with the fibula flap varies from 0% to 36.6%.24,36 Ni et al. reported the incidence of claw toe with the fibula flap with a preserved FHL and harvested FHL as 60% and 13.3%, respectively. 36 The FHL loses its insertion into the fibula during flap harvest, and the devascularized FHL muscle contracts gradually over time, which are both considered contributing factors to claw toe deformity. 36 Excision of the FHL may relieve the claw toe deformity. 36 Alternatively, incorporation of the FHL when harvesting the fibula flap or peroneal flap does not significantly increase the donor-site morbidity.35–37 Six (6/39; 15.4%) patients experienced claw toe deformity in our study. The reason for the comparatively low incidence of claw toe deformity in our series is that the FHL muscle is routinely harvested with the peroneal flap at our institute.
This study also revealed a low rate (5/39; 12.9%) of quality of life limitations among the patients. To our knowledge, no other studies of peroneal flaps have evaluated patients’ quality of life. However, a study by Kansy et al. of another peroneal artery-based flap (fibula flap), revealed that 30% of the patients experienced poor overall quality of life (overall quality of life score < 40%). 18 Ling and Peng reported that the incidence of limitations at work varied from 0% to 21.4% (mean, 9.6%). 24 The minimal effects on activities of daily living after peroneal flaps in our study may have resulted from the low (minimal or minor) degree of most donor-site comorbidities.
The peroneal flap and RFFF are two types of fasciocutaneous flaps that are frequently used for complex reconstruction after tumor ablation in head and neck cancer because of their thin and pliable skin paddles.2–6 Compared with the RFFF, peroneal flap harvest has several advantages, such as the ability of a simultaneous approach by two surgical teams; larger skin paddles; more reliable perforators, which makes separate skin paddles feasible for reconstructing complex defects;6,38 and adding the FHL muscle to achieve better results without a marked increase in donor-site morbidity, when this procedure is necessary.37,39 However, donor scar aesthetics is a constant concern regarding these two flaps. Orlik et al. revealed that 33.3% of their patients were bothered by their scar and uncomfortable about wearing short sleeves in public. 40 According to a study by de Witt et al., 27% of the patients were concerned about scar cosmesis. 41 Jani et al. reported that 5.8% of the patients complained about the cosmesis of the donor scar at the site of the RFFF. 42 Regarding aesthetics, the scar that forms after peroneal flap harvest can be covered with long trousers or socks, making it more acceptable to patients. The peroneal flap has the same donor site as the fibula flap, and several studies have shown fair to moderate cosmetic outcomes. Maciejewski and Szymczyk reported 17% moderate and 5% poor outcomes in their study. 43 Bodde et al. reported that the aesthetics assessment yielded 10% moderate, 10% intermediate, and 10% poor outcomes. 13 Maben et al. reported that 40% of the patients were dissatisfied with the appearance of the scar. 44 In our study, 97.4% (38/39) of the patients were satisfied with their scars after peroneal flap harvest. Meticulous surgical technique, layer by layer closure of the wound, and effective scar treatment resulted in inconspicuous scars in our patients. Regarding function limitations, Liu et al. reported that patients who received an RFFF had significantly less grip strength 24 months after the operation compared with preoperative strength. 7 Jani et al. reported that 39.6% of the patients complained of problems lifting a heavy object after RFFF reconstruction. 42
Peroneal flap reconstruction has been the standard in free flap reconstruction at our institute for head and neck reconstruction. In some specific conditions, we prefer the peroneal flap rather than the anterolateral thigh flap. The thin and pliable nature of peroneal flaps is superior in tongue reconstruction after hemi-glossectomy. 3 In contrast, the anterolateral thigh flap may limit the motion of the residual tone owing to its bulkiness.3,8 The peroneal flap is another choice in reconstructing huge or complicated oral and maxillofacial defects, such as through-and-through buccal defects or extensive lip defects.2,4 This is because the peroneal artery encompasses multiple reliable perforators, which enables a chimeric flap design, including the separated double skin paddle, and suitable muscle bulk.2,4 Furthermore, the skin paddle of the peroneal flap is very pliable, which facilitates shaping.4,38 Additionally, we use a peroneal flap in hypopharyngeal reconstruction because of its unique characteristics, which make it easier to shape and inset without tension. 5 Furthermore, a separated double skin paddle can serve as a sentinel when monitoring a totally buried flap in hypopharyngeal reconstruction. 10
With advances in microsurgery, various alternative fasciocutaneous flaps are being used in head and neck reconstruction worldwide; however, each method has advantages and disadvantages. For example, in our experience, the lateral arm free flap, as with the RFFF, is difficult to harvest during tumor resection using a two-teams simultaneous approach, and the resulting scar is noticeable and difficult to hide, as with the RFFF. Furthermore, the pedicle of the lateral arm free flap is relatively short, and the diameter of the artery is also small; limited size is another disadvantage. 45 The medial sural artery perforator flap is often used in tongue reconstruction owing to its thin and pliable nature, but this flap cannot be used to treat a large and complicated oral defect. 46 The free latissimus dorsi myocutaneous flap was the last option for us because of the need to change the patient’s position to harvest the flap.
Deciding which flap to choose is never easy for a reconstructive surgeon. Donor-site morbidity plays a crucial role in flap selection for free flap reconstruction. In this study, most donor-site morbidities associated with the peroneal flap were reported as minimal to mild, and almost 90% of the patients declared no limitation in their activities of daily living. We believe that the peroneal flap is reliable and versatile, with acceptable donor-site morbidity for head and neck reconstruction in well-selected conditions.
The limitations of our study must be acknowledged. First, this study is limited by a lack of comparative studies focusing on the peroneal flap in the current literature. Therefore, comparing our donor-site morbidity to that in related studies with matched surgical procedures was difficult. Second, there are no universal assessment tools for each donor-site morbidity between studies for patient-reported outcomes. Third, because the number of head and neck reconstructions with RFFF or MSAP flaps is limited at our institute, it was difficult to show statistical differences between these flaps. Another limitation of this study is the limited sample size. Further prospective studies to evaluate the donor-site morbidity associated with the peroneal flap may be needed.
Conclusion
Free flap reconstruction is state-of-the-art in head and neck cancer treatment after tumor ablation. However, donor-site morbidity is the unavoidable disadvantage. Achieving the balance between successful reconstruction and concomitant donor-site morbidity is always challenging for the reconstructive surgeon. To the best of our knowledge, this is the first study focusing on the donor-site morbidity associated with the fasciocutaneous (boneless version) peroneal flap. The long-term patient-reported outcomes in this study revealed that harvesting a peroneal flap may result in minimal or minor donor-site morbidity with no obvious impact on the patients’ daily quality of life. Although several fasciocutaneous flaps, such as the RFFF, lateral arm flap, and anterolateral thigh flap, are standard in many institutes worldwide, the free peroneal flap may prove to be a reliable flap of choice, with acceptable long-term donor-site morbidity in head and neck reconstruction. This flap should be included in the list of candidates when free flap reconstruction is considered in head and neck cancer treatment.
Footnotes
Author contributions
Shih-Yu Lee: drafting of the manuscript, and data acquisition, analysis, and interpretation. Kuo-Chung Yang, Cheng-Ta Lin, Lee-Wei Chen, and Cheng-Ta Lin: data acquisition. Wen-Chung Liu: study conception, manuscript revision, and data acquisition, analysis, and interpretation.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.