
Abstract
Neurofibromatosis type 1 (NF1) is an autosomal dominant genetic disease that causes multi-system damage. It is rarely associated with angle-closure glaucoma, especially in pediatric patients. We herein report a case of unilateral chronic angle-closure glaucoma in a patient with NF1. A 5-year-old girl with a large subcutaneous soft mass and multiple scattered coffee-milk spots presented with low vision, increased intraocular pressure, and angle closure in her right eye. Lisch nodules were seen in both eyes. In her right eye, ectropion uveae was observed at the top and bottom margins of the pupil. Magnetic resonance imaging of the skull and orbit revealed no abnormalities. Finally, trabeculectomy was performed on the right eye, after which the right eye showed a stable intraocular pressure. NF1 combined with angle-closure glaucoma is rare and easily missed in the clinical setting. Early diagnosis and treatment may achieve good results.
Keywords
Introduction
Neurofibromatosis type 1 (NF1) is a common disease that mainly affects the peripheral nervous system and skin. 1 Early diagnosis of NF1 is very difficult in pediatric patients because different clinical manifestations appear as children grow. 2 Although potential markers of early diagnosis have been recently studied, 3 there is no reliable screening test in clinical practice.
Chronic angle-closure glaucoma may not cause any symptoms until significant optic nerve damage occurs. Thus, early diagnosis and treatment can effectively reduce the damage to the optic nerve. Although glaucoma is rarely associated with NF12,4–14 (Table 1), it may be the earliest clinical sign in some patients with NF1.2,14
Clinical characteristics of patients with glaucoma and neurofibromatosis in the past 20 years.

pts, patients; F, female; M, male; C, cataract; Bl, blepharoptosis; L, Lisch nodules; G, glaucoma; EU, ectropion uvea; NV, neovascularization; RVPT, retinal vasoproliferative tumor; PAS, peripheral anterior synechiae; LPNF, lid plexiform neurofibroma; IOP, intraocular pressure.
We herein report a case of unilateral chronic angle-closure glaucoma associated with NF1 in the effort to increase awareness of these diseases and offer some insight on achieving their early diagnosis. The reporting of this study conforms to the CARE guidelines. 15
Case report
A 5-year-old girl was brought to Qingdao Eye Hospital because of a 1-year history of vision deterioration in her right eye accompanied by a large subcutaneous soft mass in the right parieto-occipital region and multiple coffee-milk spots scattered across the skin of her neck and back (Figure 1).

Multiple coffee-milk spots scattered on the skin of the neck and back.
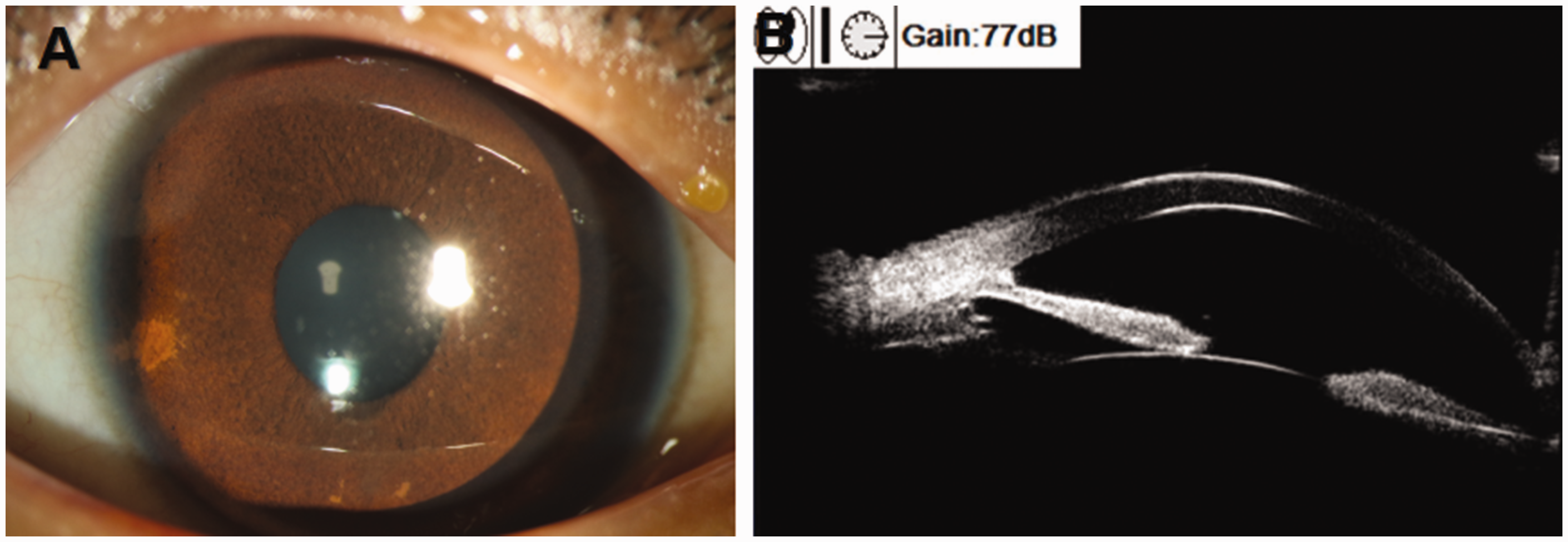
The complete ophthalmic examination revealed that the best-corrected visual acuity was 4/100 in the right eye with −4.00 diopters sphere, whereas the left eye had 20/20 vision. The intraocular pressure (IOP) of the right and left eye was 30 and 14 mmHg, respectively. Slit-lamp examination of the right eye showed multiple Lisch nodules, iris atrophy, and a significant number of iris papillary protrusions on the surface of the iris. Ectropion uveae was observed at the top and bottom margins of the pupil (Figure 2(a)). Slit-lamp examination of the left eye showed the presence of Lisch nodules on the iris and iris papillary growths (Figure 3(a)). The cup–disc ratio was 0.6 and 0.3 in the right and left eye, respectively. The fundus of the right eye showed slight retinal pigment epithelium atrophy because of enlargement of the eye (axis length: right, 29.10 mm; left, 22.96 mm).

Images of the right eye. (a) Lisch nodules, ectropion uveae, and numerous iris papillary protrusions on the surface of the iris. (b) Angle closure, peripheral anterior synechia, and flat iris nodules. (c) Angle closure, flat iris nodules in peripheral iris. (d) Loose trabecular meshwork and endothelial-like cells (stain, hematoxylin and eosin; original magnification, ×200).
Images of the left eye. (a) Lisch nodules and numerous iris papillary protrusions on the surface of the iris and (b) Angle closure in inferior temporal region of the left eye and point-like focus of high echo at the corresponding ciliary body.
Ultrasound biomicroscopy was performed in both eyes to evaluate the anterior chamber structures and the ciliary bodies. Angle closure was observed in the right eye (Figure 2(b)), and a significant number of flat iris nodules were visible in the peripheral iris under gonioscopy (Figure 2(c)). The angle closed in the inferior temporal region of the left eye, and a point-like focus of high echo was present at the corresponding ciliary body (Figure 3(b)). Specular microscopy demonstrated decreased endothelial density and increased polymegathism and polymorphism in the right eye (Figure 4). Magnetic resonance imaging of the skull and orbit revealed no abnormalities.
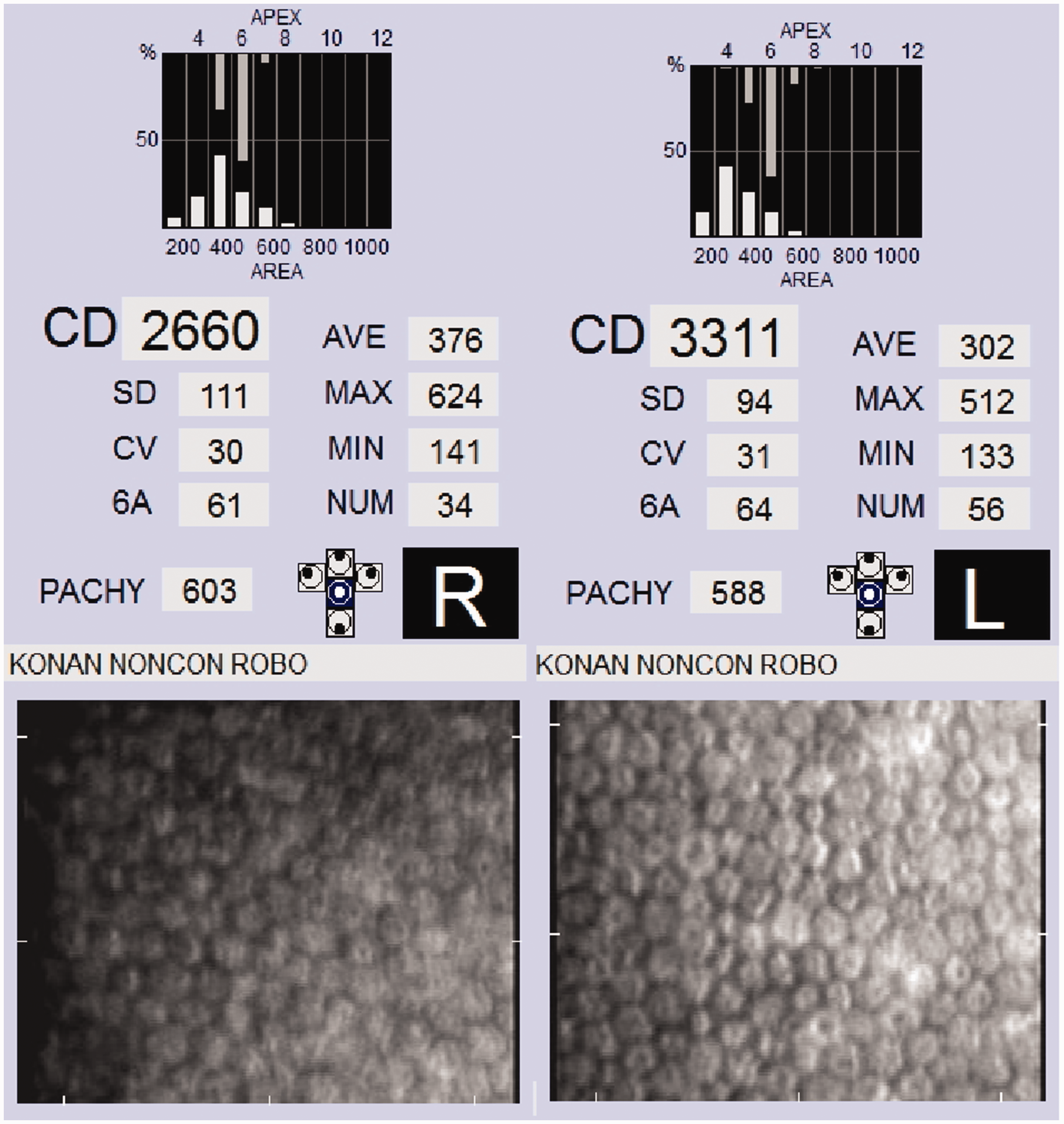
Specular microscopy demonstrated decreased endothelial density and increased polymegathism and polymorphism in the right eye.
Trabeculectomy was performed on the right eye, after which the right eye showed a stable IOP ranging from 10 to 15 mmHg during the following 6 months. Loose trabecular meshwork and endothelial-like cells could be seen in the pathologic examination of the trabecular meshwork (Figure 2(d)).
Discussion
NF is an autosomal dominant genetic disease that results in multi-system damage. It is caused by abnormal neural crest cell differentiation and can be divided into NF1 and NF2. 1 The patient in the present report had NF1, which is related to mutations in the NF1 gene at 17q11.2. 16
The pathogenesis of this glaucoma is still unknown. The following mechanisms have been considered: 1) direct blockage of the anterior chamber angle by neurofibromas, 2) developmental angle abnormalities, 3) secondary angle closure by neurofibromatous cysts or a thickening of the ciliary body and choroid, and 4) neovascular glaucoma. 17
Although our patient presented with glaucoma in the right eye, both eyes were affected. The inferior temporal angle of the left eye was closed, and a point-like focus of hyperechoic echo was present at the corresponding part of the ciliary body. Neurofibroma is speculated to involve the temporal and inferior ciliary body, finally leading to closure of the angle. However, there were no abnormalities in the ciliary body, eyelid, intraorbital region, choroid, or retina of the right eye. Pathologic examination showed an aggregation of endothelial-like cells on the surface of the trabecular meshwork. Therefore, we speculate that the pathogenesis of this patient’s glaucoma in the right eye may have had two causes: 1) A large number of peripheral iris nodules directly blocked the angle, and 2) proliferation of endothelial cells at the iris and the angle, trabecular meshwork obstruction, and pre-iris adhesion affected the aqueous drainage, leading to increased IOP and further aggravating the pre-iris adhesion, 14 forming a positive feedback cycle. Although the IOP in the left eye was normal, the changes in the left eye should continue to be closely monitored.
The right iris in this patient had obvious ectropion uveae near the pupillary edge. A previous study showed that among patients with NF, 61.54% (8/13) of patients with glaucoma presented with ectropion uveae. 13 However, the specific mechanism of ectropion uveae in NF is still unknown. Edward et al. 11 speculated that the mechanism might be related to the loss of neurofibromin (NF1 gene product) and elevated mitogen activated protein kinase gene expression in corneal endothelial cells. Abnormal proliferation of the corneal endothelium encroaches on the chamber angle, resulting in elevated IOP. Abnormalities in the number and morphology of the corneal endothelium in the right eye, as well as the finding of endothelial-like cells on the trabecular meshwork surface, were also found in our patient. Moreover, this ectropion uveae alteration in NF may be progressive. Esfandiari et al. 18 described a 3-year-old patient with NF who had unilocular ectropion uveae and developed glaucoma in this eye at the age of 10 years. IOP changes should therefore be closely followed up in patients presenting with ectropion uveae. Additionally, such patients have lower success rates with surgery than those with congenital glaucoma, which tends to require filtration or shunt surgery and may be associated with significant atrial angle abnormalities. 19
The incidence of NF1 with congenital glaucoma is low and clinically rare. Glaucoma can be its first symptom and is easily missed. In this patient, because of early detection, minimal eye tissue involvement, and relatively mild symptoms, the IOP was ideally controlled after simple trabeculectomy. However, the long-term efficacy still needs to be followed up.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231173828 - Supplemental material for Unilateral chronic angle-closure glaucoma in a pediatric patient with neurofibromatosis: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605231173828 for Unilateral chronic angle-closure glaucoma in a pediatric patient with neurofibromatosis: a case report by Mingming Jiang, Jing Zhang, Xiaomei Wan, Yichao Ding and Feijia Xie in Journal of International Medical Research
Footnotes
Author contributions
Data acquisition: MMJ, XMW, YCD, and FJX. Writing (original draft): MMJ. Writing (review and editing): JZ. Final approval of manuscript: all authors.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Declaration of patient consent
The patient’s father provided informed consent for treatment as well as written informed consent for publication of the case. This report contains no personal information that could lead to identification of the patient. This study was approved by the Ophthalmology Ethics Committee of Qingdao Eye Hospital.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.