
Abstract
Infantile leukemia is a rare hematological malignancy that occurs in the first year of life. It is an aggressive disease with peculiar immunophenotypic, cytogenetic, and molecular characteristics. It can be myeloid or lymphoid in origin. More than 80% of cases involve KMT2A gene rearrangement in the lymphoblastic subset, versus 50% in the myeloid subset. In this study, we present three cases of this rare entity to add knowledge about its clinical presentation and diagnostic profiles. These cases of infantile B-lymphoblastic leukemia (B-ALL) were retrospectively reviewed at the Department of Hematology, Section Cytogenetics at Indus Hospital and Health Network. The clinical characteristics, complete diagnostic profile, immunophenotypic profile, fluorescence in situ hybridization (FISH) results, treatments, and outcomes of the patients were assessed. All three infants were girls who presented with hyperleukocytosis, and they were diagnosed by eight-color flow cytometry. FISH studies revealed KMT2A gene rearrangement in two of the three patients. Infantile B-ALL is a biologically distinct disease carrying a poor prognosis. Female preponderance, hyperleukocytosis, and hepatosplenomegaly are common findings in this subgroup. No standard protocol for this rare entity has proven ideal for managing these young infants.
Keywords
Introduction
Infantile leukemia is a rare and biologically distinct disease from all other types of leukemia. It accounts for 2.5% to 5% of all pediatric cases of acute lymphoblastic leukemia (ALL) and 6% to 14% of all pediatric cases of acute myeloid leukemia. 1 Age at diagnosis has been recognized as an important prognostic factor for both the incidence and survival of ALL. 2 According to published statistics, the incidence of infantile leukemia is 41 cases/million, i.e., approximately 160 cases/year, and 5-year survival rate of approximately 45% is considerably lower than that for leukemia in older patients.2,3 B-lymphoblastic leukemia (B-ALL) is common in this age group, and it has a peculiar immunophenotype, such as no CD10 expression, in most cases. Central nervous system (CNS) infiltration by blasts is frequently observed in this subgroup. 4 B-ALL harbors KMT2A (previously called MLL) gene rearrangement in approximately 80% of cases, and this is known to be associated with poor prognosis. 5 Despite the improved outcome of childhood acute leukemia, infantile leukemia carries a dismal outcome. All treatment protocols to date are associated with some controversies. Furthermore, because of the aggressive nature of the disease, treatment-related complications are also common in such fragile hosts. 3 Infantile B-ALL is a resistant disease that generates tremendous interest because of its unique biology. A careful workup comprising immunophenotypic, cytogenetic, and molecular analyses is desirable for predicting the disease course and determining the outcome. In this study, we present three cases of infantile B-ALL to add knowledge about its clinical presentation and diagnostic profile.
Case presentation
Patients
We collected retrospective data for three patients from November 2020 to February 2021 in the Department of Hematology, Section Cytogenetics, Indus Hospital & Health Network (Karachi, Pakistan). Clinical data were collected from the electronic medical records of the hospital.
Methods
The immunophenotypic analysis was performed by eight-color flow cytometry (BD FACS CANTO-II, BD Biosciences, Franklin Lakes, NJ, USA) using an extensive panel of markers. Cases were analyzed using FACSDiva™ software (BD Biosciences). Interphase fluorescence in situ hybridization (FISH) was performed using dual-color dual fusion probes for BCR::ABL1 and RUNX1::RUNX1T1, whereas KMT2A and CBFB gene rearrangement was assessed using a break-apart probe. All probes were provided by Metasystem (Altlußheim, Germany). Karyotyping was performed using the conventional GTG-banding technique. Both FISH and karyotyping were performed using a Cytovision MB8 automated cell imaging system (Leica Biosystems, Wetzlar, Germany).
Written informed consent for participation has obtained from the parents of the patients. Ethical approval was obtained from the institutional review board of our institution (approval number: IHHN_IRB_2022_10_008). The reporting of this study conforms to the CARE guidelines. 6
Case No. 1
A 6-week-old girl presented to the Emergency Department with a 15-day history of pallor. The mother had no medication history during pregnancy and no antenatal visits. However, the delivery was uneventful. On physical examination, the patient’s temperature was 37°C, her respiratory rate was 68/minute, and her heart rate was 170/minute. Bilateral crepitations were present on chest auscultation, and abdominal examination revealed hepatosplenomegaly. The baseline complete blood count (CBC) revealed 40% blasts on a peripheral smear (Figure 1a) with a hemoglobin level of 6 g/dL, total leukocyte count (TLC) of 45.5 × 109/L, and platelet count of 10 × 109/L. Immunophenotypic analysis by flow cytometry was performed on bone marrow aspirate, which revealed 66% small-to-medium-sized blasts exhibiting the following phenotype: positivity for CD9, CD19, CD34, CD38, CD45, CD58, CD79a, and TdT and negativity for intracellular CD3, CD10, CD13, and CD20 (Figure 1b).

Clinical data of Case 1. (a) Peripheral smear. (b) Fluorescent in situ hybridization revealed KMT2A gene rearrangement and (c) Results of flow cytometry.
The patient was diagnosed with precursor B-ALL. FISH was performed for BCR::ABL1, ETV6::RUNX1, and KMT2A rearrangement, and KMT2A gene rearrangement was present in 71% of cells (Figure 1c). Because of her poor prognosis, the patient was kept on palliation, and her parents were counseled accordingly.
Case No. 2
A 5-week-old girl, the second child of a consanguineous marriage, visited the Emergency Department with a complaint of petechial rashes all over her body for 15 days. Her weight was 2.8 kg, and she was delivered via elective caesarean section. The antenatal and postnatal periods were unprecedented, but she had no history of in utero exposure to radiation. Her body temperature was 37°C, her respiratory rate was 35/minute, and her heart rate was 140/minute. On systemic examination, the infant had hepatosplenomegaly with significant cervical lymphadenopathy and petechial rashes. Multiple CBCs were performed during the patient’s care. Initially, she developed thrombocytopenia (Table 1). After a few days, the peripheral blood smear revealed 92% blast cells in addition to thrombocytopenia (Figure 2a).
Serial monitoring of the complete blood count in Case 2.

PCV, packed-cell volume; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; RDW-CV, red cell distribution width-coefficient of variation; WBCs, white blood cells.

Clinical data of Case 2. (a) Peripheral smear, (b) Fluorescent in situ hybridization revealed KMT2A gene rearrangement and (c) Results of flow cytometry.
The bone marrow aspirate was hypercellular, and the smear revealed small-to-medium-sized blasts characterized by a high nuclear-to-cytoplasmic ratio, fine nuclear chromatin, indistinct nucleoli, and scant-to-moderate pale basophilic non-vacuolated agranular cytoplasm. These blasts were negative for myeloperoxidase (MPO) on cytochemistry. Immunophenotyping by flow cytometry was performed using bone marrow aspirate, and this analysis revealed that the blasts were strongly positive for CD19, CD34, and CD79a; weakly positive for TdT and CD45, variably positive for CD9 and CD58; partially positive for CD10; and negative for intracellular CD3, CD13, CD20, and MPO. The patient was diagnosed with B-ALL (Figure 2b).
FISH was performed for BCR::ABL1, ETV6::RUNX1, and KMT2A rearrangement. There was no evidence of BCR::ABL1 or ETV6::RUNX1 fusion, whereas KMT2A gene rearrangement was present in 70% of the examined cells (Figure 2c). An initial workup was performed in our hospital, but the patient did not return for further treatment.
Case No. 3
A 7-month-old girl presented with high-grade fever and small swelling in the inguinal region for 6 days. There was no significant past medical history. She was not immunized. Before presentation, she had recently received a red blood cell and fresh frozen plasma transfusion in her hometown. On physical examination, her weight was 6.2 kg, she was febrile, and she had hepatosplenomegaly and inguinal lymphadenopathy. Baseline CBC revealed the following findings: hemoglobin, 9.4 g/dL; TLC, 79.9 × 109/L; and platelets, 20 × 109/L. Peripheral blood smear (Figure 3a) examination revealed 65% blasts and negativity for MPO on cytochemistry. Immunophenotyping by eight-color flow cytometry performed on peripheral blood revealed strong positivity for CD9, CD19, CD45, CD58, CD79a, and TdT; weak partial positivity for CD10; and negativity for intracellular CD3, CD13, CD20, CD33, CD34, and intracellular MPO. Hence, a diagnosis of B-ALL was made according to the morphological and immunophenotypical findings (Figure 3b). FISH using the B-ALL panel revealed no evidence of BCR::ABL1 or ETV6::RUNX1 fusion and KMT2A gene rearrangement (Figure 3c). Karyotyping by G-banding revealed a three-way translocation between the long arms of chromosomes 1, 5, and 13 (Figure 4). The patient was admitted to the pediatric intensive care unit. B-ALL high-risk protocol therapy was started. After initial stabilization, the family elected to receive alternative medicine/spiritual treatment.

Clinical data of Case 3. (a) Peripheral smear. (b) Fluorescent in situ hybridization revealed the normal signaling pattern for KMT2A and (c) Results of flow cytometry.

Karyotyping by G-banding in Case 3 revealed a three-way translocation.
A summary of all three cases is presented in Table 2.
Summary of the three cases.
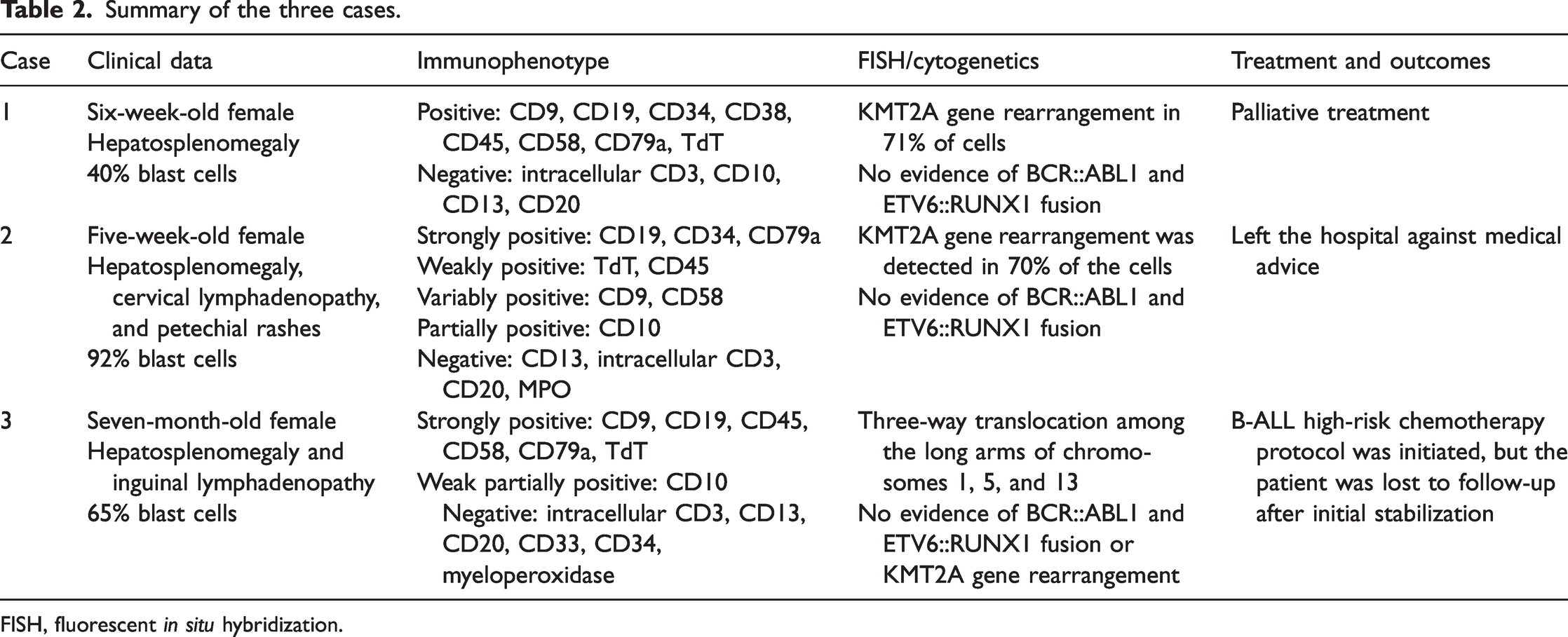
FISH, fluorescent in situ hybridization.
Discussion
Infantile leukemia refers to acute leukemia occurring in the first year of life. In addition to acute leukemia, neuroblastoma and brain tumors are also reported in this age group, and these neoplasms all occur at the same frequency. 3 There is a slight predominance of lymphoid leukemia over myeloid leukemia in infants, and among cases of lymphoid leukemia, approximately 95% belong to the B-lineage. KMT2A gene rearrangement is the genetic hallmark of infants with leukemia. This gene is located on the long arm of chromosome 11 (11q23). Any partner chromosome can be involved in this translocation. It is a recurrent non-random translocation found in B-ALL. The resulting fusion protein is known to participate in leukemogenesis by increasing HOXA9 expression. 7 Another postulated mechanism that promotes leukemia is the increased expression of the tyrosine kinase FLT3. 8 Two of our cases were positive for KMT2A gene rearrangement. Infants with this genetic alteration, especially those younger than 6 months, have a particularly poor prognosis. The patient in this study who was negative for KMT2A rearrangement carried a three-way translocation in conventional cytogenetic studies. However, the aberration was not specific to B-ALL. The data from different studies are listed in Table 3.
Data from previously published infantile leukemia studies.

WBCs, white blood cells; B-ALL, B-lymphoblastic leukemia; AML, acute myeloid leukemia.
Epidemiological data for infantile B-ALL are scarce, but most of the published literature supports the female predominance of this disease, as also evident in our study. Hyperleukocytosis, hepatosplenomegaly at presentation, and a CD10-negative immunophenotype are well-known adverse clinicopathological factors in this subtype of B-ALL, all of which were observed in our cases. 9 Additionally, CNS infiltration is a frequent clinical characteristic in this group. According to reported studies, the pro-B immunophenotype is more common in infants. All three patients in this study were negative for CD20. One patient was negative for both CD10 and CD20, whereas one patient exhibited partial CD10 expression. Only one patient was positive for CD10. In contrast to the published literature, aberrant expression of myeloid antigens was not observed in our cases. Only one patient exhibited CD13 positivity.
In general, the treatment of infantile B-ALL differs from that of childhood B-ALL. Despite advances in therapy, the mortality rate of infantile leukemia remains high. Several studies have explored the molecular characteristics and clinical outcome of this rare entity, and the findings suggested that its etiology differs from those of other childhood leukemias and possibly involves prenatal factors.10,11 Three large groups conducted clinical trials specific to infant ALL, including Interfant (Interfant-06), COG (AALL0631), and JPLSG (MLL-10). These groups adopted a risk stratification approach based on KMT2A gene rearrangement. The results of Interfant-06, which compared myeloid-type consolidation to a lymphoid protocol, were not promising. 12 COG AALL 0631 incorporated an FLT3 inhibitor, which induced some improvement in a select group of patients; however, the overall event-free survival rate remained unchanged. 14 The results of JPSLG were optimistic, but hematopoietic stem cell transplant (HSCT) is challenge for countries such as Pakistan. 14 Most centers in lower-to-middle–income countries have limited health resources. Similarly, our hospital is also providing services despite financial constraints. Currently, we do not have a HSCT facility in our center. Patients undergoing HSCT are highly vulnerable to complications and toxicities. Therefore, a good multidisciplinary team and standardized supportive services are required to offer HSCT to these patients. Fascinating discoveries in molecular biology have led to the development of novel therapeutic strategies that resulted in better outcomes. In developed countries, CD19- and CD33-directed treatments are already in different phases of clinical development. Emerging targeted therapies are most likely to be beneficial for young patients with ALL. The parents of all three patients were counseled about the disease prognosis. After diagnostic workup and initial stabilization, two patients left before treatment, whereas one patient was admitted and offered palliative therapy. The survival rate in older children is reaching 90% in developed countries, but infants with leukemia have an extremely poor 5-year survival rate of ≤50%. The availability of newer targeted therapies and HSCT along with good supportive care may improve the outcomes of such patients in our settings.
In conclusion, infantile B-ALL is a unique disease with age-related clinicopathologic and genetic manifestations. Despite limitations, this case series provides a significant contribution to the scarce literature reported on this entity, especially in our region.
Footnotes
Acknowledgment
We offer our sincere thanks to Mr. Talha Israr (assistant manager, flow cytometry laboratory, Indus Hospital & Health Network, Karachi, Pakistan) for his contribution to this study.
Authors’ contributions
NM and SI conceived the designed the study. SM analyzed and interpreted the patient data and wrote the initial draft of the manuscript. SP and NJ critically reviewed the manuscript for important intellectual content. All authors read and approved the final manuscript.
Data availability statement
Data from this study are available upon reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study received no funding, grants, or other support.