
Abstract
Paraduodenal hernias (PDHs) are rare types of internal hernias that pose a significant diagnostic and therapeutic challenge because they can present with non-specific symptoms ranging from digestive disorders and chronic abdominal pain to symptoms of intestinal obstruction which may be life-threatening. We describe here a woman in her early 30’s who presented to the emergency department with a three-hour history of generalized intermittent crampy abdominal pain. She had experienced multiple similar episodes of this pain over the past 20 years. Totally laparoscopic technique was used to complete the diagnosis and treatment of a large left PHD with accompanying acute intestinal obstruction. The operation was successful and the patient was discharged from hospital 10 days later. PDH should be considered if a patient complains of recurrent abdominal pain without any other obvious explanation; a laparoscopic approach can be used to identify and repair the hernia.
Keywords
Background
Paraduodenal hernia (PDH) is a rare congenital condition caused by abnormal rotation and fixation of the midgut during embryonic development. 1 The hernia can be broadly separated into left and right and PDHs account for up to 53% of all internal hernias and 0.2–0.9% of small intestinal obstructions. 2 A PDH poses a significant diagnostic and therapeutic challenge for clinicians because of its rarity and the fact that it can present with non-specific symptoms ranging from digestive disorders and chronic abdominal pain to symptoms of intestinal obstruction. 3 In addition, there is no specific imaging manifestation or laboratory findings to distinguish PDH from other pathologies. 4 All of these factors complicate diagnosis and may cause a delay in effective treatment which can result in strangulated intestinal obstruction, intestinal perforation or even death. 5 We describe here, a case in a young woman with acute intestinal obstruction where a large, left PDH was successfully identified and treated using a totally laparoscopic approach.
Case presentation
A female patient in her early 30’s came to the emergency department after experiencing three hours of nonspecific intermittent, crampy, stomach pain. Her pain was accompanied by nausea and multiple episodes of vomiting, and the pain grew worse after meals. Her last defecation was three days prior to the presentation. She had experienced multiple similar episodes of this pain over the past 20 years, which worsened after meals and improved with a specific body positioning. She had no prior history of abdominal surgery.
An abdominal examination showed distended abdomen with mild tenderness and peritonitis in the left upper quadrant. Blood test results showed that her neutrophil percentage was 85%. A computed tomography (CT) abdominal scan and three-dimensional CT reconstruction showed a smooth encapsulated sac-like mass of small intestinal loops between the stomach and the pancreas at the level of the ligament of Treitz (Figure 1). An internal hernia with small intestine torsion was suspected and so an emergency laparoscopic exploration was undertaken. The hernia orifice was found on the left side of the ligament of Treitz. There was a cluster of small intestines herniated into the fossa of Landzert and incarcerated. A diagnosis of left PDH was confirmed and we performed a laparoscopic repair.
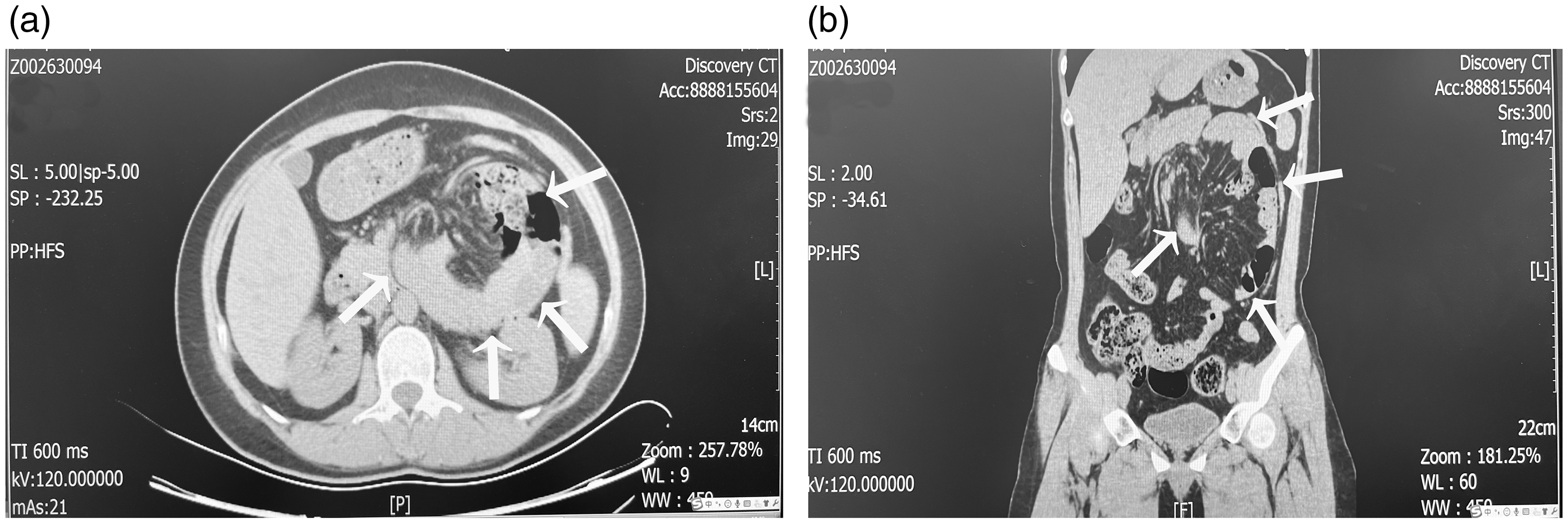
Computed tomography (CT) scan of the abdomen (a: Axial and b: Coronal Images) demonstrating sac-like clustered small bowel loops (white arrows) in the left upper quadrant located anterior to the pancreas and posterior to the stomach.
The hernia orifice was opened and approximately two metres of dilated small intestinal loop was released from the hernia sac (Figure 2a). Due to prompt surgical intervention, the small intestinal blood flow was not seriously affected and so intestinal ischemia, intestinal necrosis, and/or small bowel perforation were avoided. Fortunately, the patient did not require small bowel resection. To avoid injury to the inferior mesenteric vein and ascending left colic artery, the hernia orifice was closed carefully with 2-0 V-Loc absorbable suture (Covidien LLC) (Figure 2b). The operation was successful with no adverse consequences. The patient was given parenteral nutrition support for seven days before returning to a normal diet. She was discharged from hospital with no postoperative complications 10 days after surgery.

Intraoperative pictures showing (a) the left paraduodenal hernia with jejunum as content (white arrows showing the hernia orifice) and (b) closing of the defect (white arrows) with 2-0 V-Loc absorbable suture (Covidien LLC).
This case study was approved by Institutional Research Human or Animal Ethics Committee, Qingdao Municipal Hospital (No: 7877) and signed informed consent was obtained from the patient before publishing her anonymised data. The reporting of this study conforms to CARE guidelines. 6
Discussion
Internal hernias are rare, may be acquired or congenital, and pose a diagnostic and therapeutic challenge for clinicians.3,4 PDHs are the most common type of internal hernia and are often associated with non-specific symptoms, most cases only being identified at the time of surgery. 4 Left PDHs which occur when the intestinal tract prolapses to the dorsal side of the descending mesocolon via the dorsal side of the inferior mesenteric vein (Landzert's fossa), are three times as common as right PDHs which occur when the intestinal tract prolapses to the right via the dorsal side of the superior mesenteric vein (Waldeyer's fossa).4,7 Left PDHs usually present in the 4th to 6th decades of life, with a mean age of presentation at 38.5 years. 1 Since these hernias are rarely seen in practice, it is important for clinicians and radiologists to familiarise themselves with the condition because an unidentified PDH can result in ischaemia, strangulation, intestinal obstruction and fatality.1,5
This case report illustrates the importance of taking a detailed medical history because, similar to our patient, approximately 50% of patients recall previous nonspecific, recurrent, abdominal pain, 8 which typically worsens after meals and improves with body position. 9 Importantly, radiological investigations have significant value, as medical history and physical examination findings can be inconclusive. Abdominal CT scans may show a well-circumscribed cluster of small bowel loops to the left or right of the midline.10,11 Stretching or displacement of mesenteric vessels at the entrance to the hernia orifice is another key sign of an internal hernia. 7
Surgical repair of PDHs is recommended including elective repair in asymptomatic cases. This is because up to 50% of cases will result in obstruction and are associated with a mortality rate of >20%. 12 Surgery may be performed using either the traditional open approach or a minimally invasive laparoscopic approach. 13 According to our experience, laparoscopic herniorrhaphy is a useful minimally invasive technique for both definitive diagnosis and treatment of PDH with acute intestinal obstruction. Compared with other cases reported in the literature, the hernia sac in our patient was large and although complicated, we successfully completed the surgery under laparoscopic techniques without using an open approach. Studies have shown that laparoscopic herniorrhaphy for PDH has significant advantages over open techniques, in terms of less postoperative pain, earlier upgrade of diet, shorter hospital stays, lower rates of ileus, lower morbidity,14,15 and as illustrated in our case, cosmetic benefits. In the case presented here, prompt surgery resulted in a good clinical outcome for the patient.
Irrespective of the surgical approach, the principles of treatment for PDH include reduction of the hernia content, resection of any necrotic intestinal segment, and repair of the hernial orifice by closure or wide opening. This is done by performing an incision along the avascular plane of the mesocolon or dividing the inferior mesenteric vein so that the hernia sac becomes part of the peritoneal cavity. 16 According to our experience, our team prefers closing the hernial orifice to wide opening, because the former can result in a reduction of recurrence without significantly increasing the risk of displacement of the inferior mesenteric vein. Compared with reduction of the hernia contents, treating the hernia orifice is thought to be more difficult and is associated with some complications,17,18 including the inferior mesenteric vein injury or recurrence.
In summary, PDH should be considered in the differential diagnosis of a patient with a history of recurrent abdominal pain without any other obvious explanation, such as a history of abdominal surgery, an external hernia, or an intra-abdominal inflammatory disease. The laparoscopic approach to treatment has advantages because it can be used both to identify the condition and to repair the hernia.
Footnotes
Acknowledgments
The authors would like to thank all members of the study team, the patient, and her family.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research project received no specific grant support from any funding agency in the public, commercial, or not-for-profit sectors.