
Abstract
Sclerosing encapsulating peritonitis (SEP) is a disease that is rarely encountered clinically. Preoperative diagnosis of SEP can be difficult. However, with imaging technology, such as computed tomography (CT), this condition can be diagnosed without surgery and pathological analysis. SEP is characterized by small intestine being partially or completely encased by a layer of a thick grayish-white fibrocollagenous membrane similar to a cocoon. The most common symptoms of SEP are abdominal pain, nausea, and vomiting. SEP often leads to intestinal obstruction. Our hospital treated three emergency patients who complained of acute or chronic abdominal pain. CT showed “cauliflower sign” in two cases. The three patients were diagnosed with SEP intraoperatively. In a female patient with ascites, the situation was extremely serious, and this condition had not been reported in detail previously. Fortunately, all patients were discharged without complications. We should pay special attention to patients with SEP who have ascites, which indicates a serious situation.
Keywords
Introduction
Sclerosing encapsulating peritonitis (SEP) is characterized by the small intestine being partially or completely encased by a fibrous membrane. 1 Owtschinnikow 2 first reported this disease as “peritonitis chronica fibrosa incapsulata” in 1907, while Foo et al first used the name “abdominal cocoon” in 1978. 3 The prevalence of SEP is not clear. Akbulut provided a detailed classification of SEP, which is divided into primary and secondary forms according to the underlying etiology. 4 Primary SEP has also been termed idiopathic SEP or abdominal cocoon, which has no definite cause. Secondary SEP always has a history of peritoneal dialysis, abdominal tuberculosis, medicine intake, abdominal surgery, or organ transplantation. The highest risk factor for secondary SEP is peritoneal dialysis. 5 We report three cases of SEP, including one case with ascites, which has not been reported in detail previously, and describe all of the main types of SEP in detail by case studies.
Case report
Our hospital treated three emergency patients who complained of acute or chronic abdominal pain. All of these patients were diagnosed with SEP. The average age of the patients was 53.3 years (range, 50–56 years), with one man and two women. All patients underwent emergency contrast-enhanced computed tomography (CT). Tumor biomarker tests, such as those for carcinoembryonic antigen, carbohydrate antigen-125, and carbohydrate antigen-199, showed normal levels (Table 1).
Data of three patients with SEP.

Hb: hemoglobin; WBC: white blood cell; BUN: blood urea nitrogen; CEA: carcinoembryonic antigen; CA-125: carbohydrate antigen-125; CA-199: carbohydrate antigen-199.
The male patient (patient 1) had acute abdominal pain that lasted for 8 hours without a history of abdominal surgery, medicine intake, or peritoneal dialysis. On a clinical examination, the abdomen was tender and distended. CT showed “cauliflower sign” as previously described, 6 where small intestinal loops congregated to the center of the abdomen by a sac (Figure 1a, b). Exploratory laparotomy was performed and a thick fibrous membrane covering the small intestine was revealed intraoperatively (Figure 2a). Therefore, this case was diagnosed as primary SEP. The patient underwent resection of the membrane, adhesiolysis, and intestinal decompression. A histological examination of the membrane tissue showed proliferative glassy fibrous tissue with chronic inflammatory cell infiltration (Figure 3). The patient was hospitalized for 1 week.

Computed tomographic images of patients 1 and 2. (a–c) The small intestine is encapsulated with a membrane like a cocoon (white arrow) (a, b: patient 1). (c) A large amount of ascites can be seen in the abdominal cavity (patient 2).
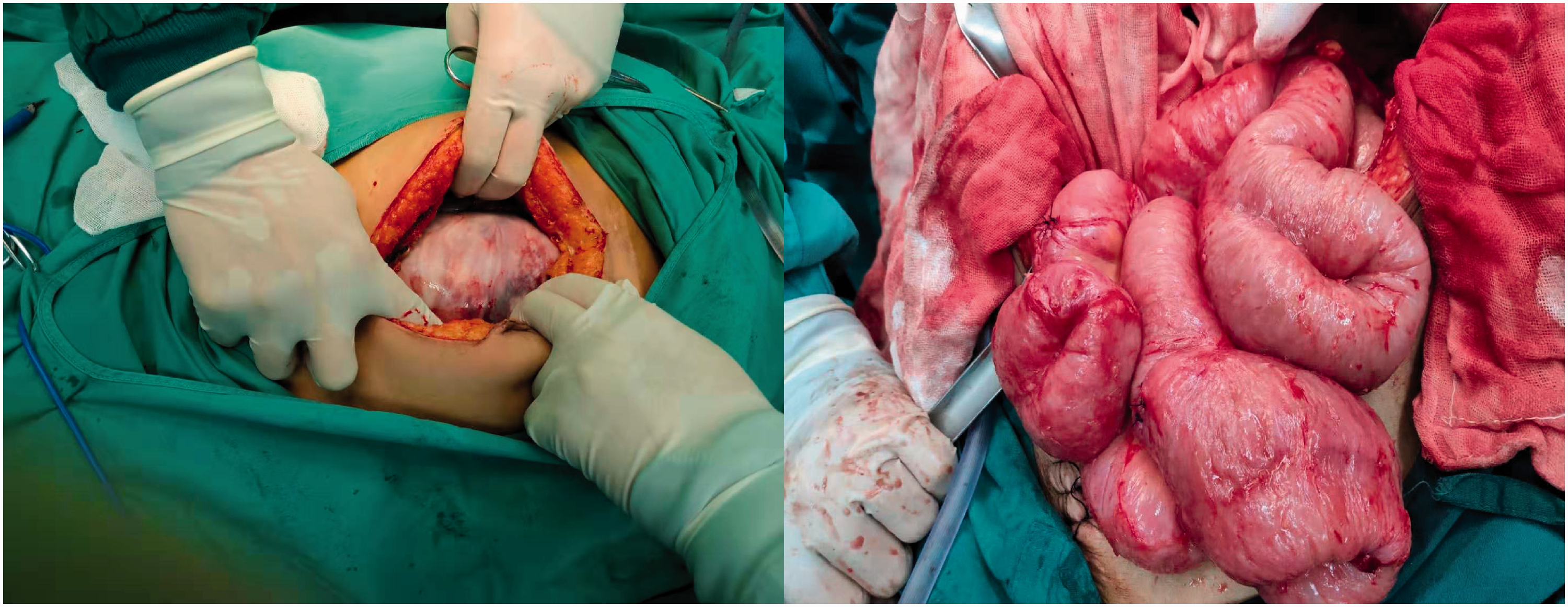
Intraoperative findings. (a) The small intestine is covered with a thick fibrous membrane (patient 1). (b) Fibrin membranes were resected after enterolysis (patient 3).

Histology of membranous tissues shows proliferative glassy fibrous tissue with chronic inflammatory cell infiltration (hematoxylin and eosin, ×40) (patient 1).
One female patient (patient 2) presented with acute abdominal pain for nearly 1 day and had no major medical or clinical history. Her abdomen was also tender and distended during a clinical examination. CT showed a similar result to that for patient 1, but there was a large amount of bloody ascites, which was confirmed by abdominocentesis (Figure 1c). During the operation, we found a fibrous membrane covering all of the small intestines. The small intestines clung together and were dark red without twisting or strangulation. The wall of the small intestine was thickened. There was a large amount of bloody ascites in the abdominal cavity. Therefore, this case was diagnosed as primary SEP. The patient’s vital signs were unstable since the start of monitoring. We only removed the ascites, placed an abdominal drainage tube, and then closed the abdomen. The patient was sent to the intensive care unit for conservative treatment. Surprisingly, the patient gradually recovered, except for a poorly healed incision.
The other female patient (patient 3) had chronical abdominal pain, nausea, and vomiting for nearly half a year who had undergone peritoneal dialysis more than 4 years previously. The patient had been treated conservatively several times previously. A clinical examination showed pain in the whole abdomen, especially in the upper abdomen. A sticky fibrin membrane on the top of the bowel containing brown and thick peritoneum was observed intraoperatively. Therefore, this case was diagnosed as secondary SEP. The patient underwent adhesiolysis (Figure 2b) and the operation lasted for 4 hours. Because of the intestinal dysfunction, the patient was treated with glucocorticoids on day 7 and allowed to eat orally on day 14. The patient had a good recovery.
All patients were satisfied with the treatment that they received. None of the patients have been readmitted and they were well on follow-up.
Discussion
SEP is a rare disease which is characterized by the small intestine being partially or completely encased by a fibrous membrane. This membrane is formed of collagen and fibrous tissue accompanied by nonspecific chronic inflammation. There have been case reports of SEP, including imaging or observational studies.7,8 SEP can occur in all age groups and the oldest patient reported in the literature was 90 years old. 9 The most common manifestation of SEP is small intestinal obstruction, which accounts for two thirds of the patients. 10 This disease can be divided into two categories of primary SEP also known as idiopathic sclerosing peritonitis, abdominal cocoon, or abdominal cocoon syndrome, and secondary SEP. The precise definition of primary SEP is that there is no accurate factor to explain this disease. The cause of primary SEP may be related to congenital fetal dysplasia. 11 Patients with secondary SEP always have a history of peritoneal dialysis, abdominal tuberculosis, medicine intake, abdominal surgery, or organ transplantation.
Preoperative diagnosis of SEP is difficult because of a lack of specificity in the early clinical manifestation. An abdominal X-ray of SEP may show dilated intestines with air–fluid levels. CT is the most useful imaging technique, especially in the diagnosis of intestinal mesenteric ischemia leading to necrosis.12,13 CT can show cauliflower sign where small intestinal loops congregate to the center of the abdomen encased by a fibrous membrane, as observed in patients’ 1 and 2. Other imaging features include ascites, peritoneal thickening, and peritoneal calcification. Histopathological examination of the membrane is always fibrous tissue with or without an inflammatory reaction.
The treatment of SEP includes conservative treatment and surgical treatment. Conservative treatment consists of fasting, use of a nasogastric tube, enteral or parenteral nutrition, somatostatin, cessation of peritoneal dialysis, immunosuppression, and corticosteroids. Explorative laparotomy is rational if the patient has recurrent intestinal obstruction or acute abdomen, especially in conjunction with the patient’s CT findings. Surgical treatments, such as enterolysis and membrane resection, are recommended for patients who have a history of recurrent intestinal obstruction or who fail to respond to conservative treatment. Enterectomy is performed for patients with intestinal necrosis, but anastomosis of the intestinal loops is not recommended because it may cause a high percentage of surgical complications, such as intestinal fistula. If resection needs to be performed, a stoma is highly recommended, especially in patients who have gastrointestinal perforation. 14 Care should also be taken not to remove too much of the small intestine, which could cause short bowel syndrome.
Peritoneal fibrosis may lead to ascites by blocking lymphatic vessels, which is a nonspecific symptom. 15 However, abdominal ascites often indicates a severe case. In one of our cases (patient 2), bloody ascites was observed by abdominocentesis, which suggested intestinal necrosis. At laparotomy, we found that the small intestine was dark red and observed the activity of the intestine for nearly 1 hour, but we were still unable to decide how to proceed. Even if the small intestine had been resected, the patient still would not have had a good prognosis. We ended the operation by placing an abdominal drainage tube and the patient recovered.
Peritoneal dialysis can be complicated by SEP, which is the most severe complication. Dialysis solution and repeated infections may damage the normal physiological function of the peritoneum. This pathophysiological process undergoes three stages of turbidity, deformation, and fibrosis.12,13 In one of our cases (patient 3), the patient had stopped peritoneal dialysis and received conservative treatment several times, which was ineffective. The disease had seriously affected the quality of life of the patient. We finally performed adhesiolysis without intestinal resection. In such patients, surgeons need to be careful because such operations take a lot of time to perform.
Conclusion
SEP is a disease that is not frequently encounter in clinical work, and some patients with SEP are asymptomatic. Early diagnosis of SEP needs to be made in combination with the patient’s symptoms and an auxiliary examination, especially contrast-enhanced CT. Therefore, CT has become a necessary and important tool if the cause of intestinal obstruction or acute abdomen is unknown. Initially, patients with primary SEP can be treated conservatively. If there is repeated intestinal obstruction or conservative treatment for acute abdomen is ineffective, patients require immediate surgical treatment. For patients with secondary SEP, especially those with a history of peritoneal dialysis, surgery is often required. Patients with SEP who have ascites, which indicates a serious condition, require special attention. If surgery is necessary, the fibrous membrane should be removed and intestinal adhesions should be released. Enterectomy should also be avoided as much as possible, which may lead to serious complications, such as intestinal fistula.
Footnotes
Ethics statement
Written consent for publication was granted by the patients who agreed that details/images may be viewed on the Internet and accessed by the general public. The Ethics Committee of Affiliated Yantai Yuhuangding Hospital of Qingdao University approved this study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.