
Abstract
Endoscopic transaxillary thyroidectomy is a common method for remote-access thyroidectomy. The approach typically uses a gasless method, and a long incision to insert a special retractor. In addition, it is considered only suitable for unilateral lobectomy because of problems accessing contralateral parts of the thyroid gland. We describe here, a case of a young woman who had a total thyroidectomy performed using an endoscopic approach. We reduced the non-inflated 4–6 cm incision that is usually required, into three holes, and performed unilateral transaxillary thyroidectomy; this was verified by radioactive iodine uptake and thyroglobulin levels during follow-up. The approach was clinically successful and resulted in minimal scarring. More studies are required to optimize this promising technique.
Background
Endoscopic thyroidectomy is a relatively new surgical method that meets patients’ cosmetic needs and offers better quality of life outcomes due to a lack of neck scarring.1,2 In addition, the method provides a magnified view to surgeons, making it easier for them to identify and protect important structures such as the recurrent laryngeal nerve, the superior laryngeal nerve, and the parathyroid glands. 3 Although operation time is prolonged, the technique has few disadvantages compared with traditional open thyroidectomy and the clinical outcomes are similar.4,5 While several remote-access thyroidectomy sites including, breast, axillary, transoral, and bilateral axilla-breast approaches have been developed, there is no consensus on the best approach. 6
Initially, transaxillary thyroidectomy was performed using a unilateral axillo-breast approach and robot assisted manipulation with gas-insufflation using a 3-port system.7–9 A gasless method was established in 2001 and it has now become the most widely used endoscopic transaxillary thyroidectomy procedure. 10 Over the years, the procedure has improved and studies show it is comparable to open thyroidectomy in terms of early surgical outcomes and complications. 10 The procedure involves an incision of approximately 4–6 cm in the axilla so that a special retractor can be placed to stretch the clavicular head of the sternocleidomastoid muscle (SCM). In some cases, the placement of an additional trocar through a 5 mm incision is also required. 10 The length of the incision in this gasless transaxillary approach is longer than that in other remote-access thyroidectomy approaches. 11 Due to the occlusion of the trachea that occurs in this approach, it is challenging to perform a total thyroidectomy from a unilateral axillary approach. 12 Therefore, surgeons typically use a bilateral approach or use another remote-access thyroidectomy procedure when total thyroidectomy is required. 13
Although several studies have reported the use of robot-assisted total thyroidectomy through a unilateral axillary approach,7–9 to our knowledge, no studies have reported this procedure using endoscopy. Indeed, because of the perceived difficulty in accessing the contralateral anatomy of the thyroid gland, endoscopic transaxillary thyroidectomy is considered only suitable for unilateral lobectomy. 14 However, we describe here, a report of endoscopic total thyroidectomy performed through a unilateral transaxillary approach.
Case Report
A female patient in her early 40’s was diagnosed with a thyroid nodule during a physical examination; she was 161 cm in height and weighed 57 kg. She had not experienced tracheal compression or any voice change. Ultrasonography showed a 1.1 cm nodule in the right lobe of her thyroid gland. The thyroid was determined to be TI-RADS grade 4B (i.e., suspicious (10–80% malignancy), 15 and no significant cervical lymph node enlargement was identified. A thyroid biopsy showed papillary thyroid carcinoma with a mutation in the BRAF gene. All results from routine pre-operative examinations were within normal ranges. The patient expressed strong cosmetic considerations prior to the operation. The planned surgical process was unilateral axillary total thyroidectomy and right central lymph node dissection.
Following anaesthesia, the patient’s neck was hyperextended while the right upper extremity was abducted. Two 5 mm incisions were made to serve as openings through which to perform the operation: one was located at the top of the axillary crease and the other was located at the vertex of the upper outer quadrant of the mammary gland. A 10 mm incision made at the midpoint of the line connecting the two points was used as an observation opening. The subcutaneous tunnel was punctured, and the cavity was gradually enlarged and expanded, starting approximately 3 cm below the clavicle.
An incision was made between the sternal head and clavicular head of the SCM. The elevator SCM muscle clavicle head was pulled up with percutaneous sutures. The suture was fixed on the anaesthesia frame by rubber band traction (Figure 1). The internal jugular vein and common carotid artery were dissociated, exposed, and protected. The infrahyoid muscles and the right lobe of the thyroid were lifted with percutaneous sutures. The right lobe of the thyroid and the right level VI lymph nodes were resected from the posterior approach to the anterior. The right lobe specimen was cut at the isthmus and removed (Figure 2). The upper right parathyroid gland was preserved in situ, and the lower parathyroid gland was auto transplanted in the pectoralis major muscle.

The sternocleidomastoid muscle strap muscles were moved with sutures and fixed on to the anaesthesia frame.
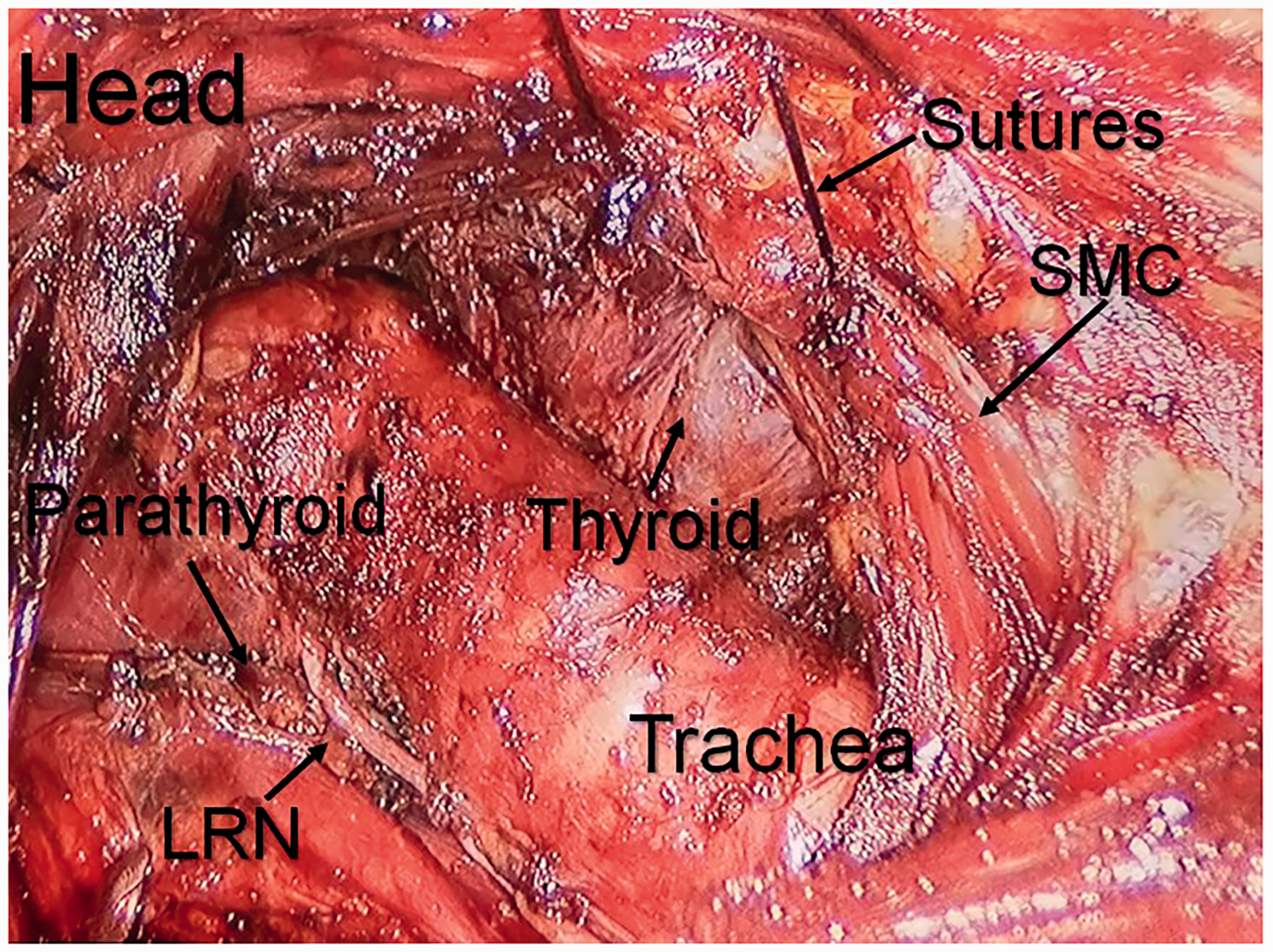
After the right thyroid gland was removed, the contralateral lobe of the thyroid gland was pulled forward along with the strap muscles. LRN: laryngeal recurrent nerve; SCM: sternocleidomastoid.
The ends of conventional endoscopic instruments cannot be steered, and so it is challenging to remove the contralateral thyroid lobe (Figure 3a). However, a steerable robotic arm makes transaxillary total thyroidectomy feasible (Figure 3b). The left lobe of the thyroid was pulled upward by percutaneous sutures and then the left recurrent laryngeal nerve was located at the inferior pole of the left lobe. (Figure 3c). The cephalad was dissociated along the nerve, and the recurrent laryngeal nerve was exposed until the point where it entered the larynx. The superior thyroid blood vessels were removed with an ultrasonically activated scalpel, and the left thyroid lobe was wholly dissociated from the trachea. The left thyroid lobe was entirely removed by separating the space between the left thyroid lobe and the ribbon muscle (Figure 4). A drainage tube was placed through the lowest puncture hole in the surgical area (Figure 5). The total operation time was 175 minutes.

(a) A conventional endoscopic instrument cannot access the entire thyroid during a trans-axillary procedure. (b) A steerable robotic arm makes trans-axillary total thyroidectomy feasible and (c) Contralateral lobe of thyroid was retracted by the suture.

A view of the surgical field after removal of the left lobe of the thyroid. CCA: common carotid artery; RLN: recurrent laryngeal nerve.

The incision site.
On the first day post-operation, the patient had no hoarseness and no difficulties drinking or eating; the drainage volume was 15 ml. The patient’s drainage tube was removed 72 hours after the operation and she was discharged from hospital on the same day. Post-operative pathology confirmed the diagnosis of papillary thyroid carcinoma in the right lobe with metastasis to one of eight lymph nodes tested. At a follow-up visit a month after the operation, the patient showed no voice changes and her blood levels were as follows: calcium, 2.2 mmol/l (normal range: 2.1–2.5 mmol/l); parathyroid hormone, 19 pg/ml (normal range: 15–65 pg/ml); thyroglobulin, <0.04 µg/l (normal range: 1.5–38.5 µg/l).
Ethics committee approval was not required for this case report. Signed informed consent was obtained from the patient before publishing her anonymised data. The reporting of this study conforms to CARE guidelines. 16
Discussion
Conventional thyroidectomy via an open approach can leave significant cervical scars which may affect a patient’s appearance and confidence. The emergence of robotic technology has led to the development of advanced surgical techniques that are minimally invasive. Remote-access thyroidectomy provides an option for patients who are strongly influenced by the aesthetic aspects of surgery.1,2 Indeed, robotic or endoscopic thyroidectomy aims to reduce surgical wounds as much as possible, and so reduce pain and meet aesthetic needs while achieving desired therapeutic effect. However, robotic surgery can be expensive and is not universally available. 17 To develop a non-robotic strategy to perform transaxillary total thyroidectomy, we improved an existing endoscopic technique. We reduced the non-inflated 4–6 cm incision into three holes, and performed unilateral transaxillary thyroidectomy.
We had the same surgical field of view as in a gasless operation without the need for a long incision to insert the retractor. Most surgery involves the anterior SCM approach to visualizing the thyroid gland rather than the inter-SCM approach. 7 To address this problem, we sutured the SCM clavicular head and infrahyoid muscles in multiple sites percutaneously, and lifted the muscles with an external rubber suture and fixed them on the anaesthesia frame. As a result of these manipulations, the thyroidectomy could be done using an inter-SCM approach.
Unlike robotic arms, the end of the endoscopic instrument cannot be steered freely, which typically makes removal of the contralateral lobe of the thyroid via endoscopy difficult. To remove the contralateral lobe, we performed several adjustments to the endoscopic method. Initially, to create enough visual space, we removed the right lobe of the thyroid together with the isthmus before resection of the contralateral thyroid lobe. Thereafter, the contralateral lobe was retracted with care avoiding the trachea. Furthermore, the gland lobe together with strap muscles was tracked upward and laterally by the suture, so the recurrent laryngeal nerve and oesophagus could be seen from the opposite side. The sutures were removed at the end of the process, and no noticeable scar was left on the neck, The surgical scar that was left with only three ports is much smaller than the scar that is left after a gasless operation.
Despite the success of this procedure, it had some limitations that need to be considered prior to widespread implementation of this technology. For instance, our patient had a small thyroid tumour and a low BMI which facilitated the successful implementation of the surgery. Whether such a technique is also suitable for patients with a large BMI and more thyroid volume remains to be explored. In addition, some patients who underwent total thyroidectomy also require a bilateral central neck resection. Whether the contralateral central neck lymph node could also be resected using a unilateral transaxillary approach, requires further investigation.
While the robotic approach to total thyroidectomy is attractive, the financial cost is greater than that for endoscopic surgery, which has impacted its use in hospitals.17,18 We have provided preliminarily evidence that suggests, in select case, it is feasible to perform total thyroidectomy using an endoscopic unilateral transaxillary approach. This procedure needs to be performed in more patients, and long-term follow-ups are required.