
Abstract
Ingestion of a foreign body (FB) is a common emergency encountered in otorhinolaryngology. In most cases, FBs pass through the digestive tract spontaneously without any serious consequences, but some of them require nonsurgical interventions, and more severe cases require surgical interventions. The types of FBs ingested may differ in different countries and regions. In adults, bones, fish bones, and dental prostheses are most commonly found in the esophagus, and most of the FBs are retained in the esophagus less than 1 month. To the best of our knowledge, this is the first report of an unusual FB (a beer bottle cap) that was stuck in the upper esophagus for longer than 4 months. The main complaints of the patient were a sore throat and FB sensation, and an FB was diagnosed by a chest radiograph and computed tomography of the esophagus. He then had rigid endoscopic removal of the FB performed under anesthesia with propofol sedation. During a 3-month follow-up, the patient was asymptomatic and no esophageal stricture was observed. Impaction of FBs in the gastrointestinal tract can lead to severe adverse events. Therefore, early detection and timely management of FBs are important.
Introduction
Ingestion of a foreign body (FB) is a frequent clinical situation and a relatively common emergency encountered in the field of otorhinolaryngology. In adults, 80% of FBs pass spontaneously, but 10% to 20% of cases require nonsurgical intervention, and ≤1% require surgery. 1 Gastrointestinal FB ingestion tends to be accidental in adults, and bones, fish bones, and dental prostheses are the most common esophageal FBs found in adults. 2 Ingestion of a FB is usually viewed as a serious medical issue, and it needs to be removed as soon as possible. The duration of FB impaction differs among studies, but to the best of our knowledge, there have been no cases of a retained FB for longer than 3 months. Plain radiography and computed tomography (CT) are effective methods for detecting FBs in the esophagus. Rigid esophagoscopy and flexible esophagoscopy are good choices for treatment, but the choice of treatment is affected by many factors. We report a rare case of an unusual FB, a beer bottle cap, which was stuck in the upper esophagus for longer than 4 months and was removed by rigid endoscopy.
Case presentation
A 38-year-old man presented to our clinic with the complaints of a sore throat and FB sensation for the last 4 months. He had no family or psychosocial history. He was treated as having chronic pharyngitis at a local clinic. His symptoms were resolved with anti-inflammatory treatment. Therefore, no examinations were performed. He felt discomfort in the chest recently and was taken to the local hospital. Flexible esophagoscopy was performed, which showed a FB in the upper esophagus. He was then referred to our hospital. Chest radiography (three-dimensional reconstruction) showed a metal bottle cap impacted at the T1–T2 cervical spine level (Figure 1). A CT scan of the esophagus was also performed and showed a circular-like foreign object impacted in the cervicothoracic segment of the esophagus along with hypertrophy of the surrounding esophageal wall and an ambiguous peripheral fat gap (Figures 2 and 3). We planned to perform rigid endoscopic removal of the foreign object under anesthesia with propofol sedation, and the patient provided informed consent. On the next day, under anesthesia with propofol sedation, rigid endoscopic removal of a FB (beer bottle cap) of 2.5 × 2.5 cm was performed. A large amount of granulation tissue was observed inside the bottle cap (Figure 4a–c) and it was sent for a pathological biopsy. The pathological diagnosis was inflammatory granulation tissue with inflammatory necrosis and mycobacteria (Figure 4d). The patient was then kept under postprocedural observation with no food by mouth for 5 days and proper supportive care. On the fifth day, gastroscopy was reviewed, and longitudinal ulcers were observed in the upper esophagus with granulation tissue at the margin of the ulcers and no perforation (Figure 5). During a 3-month follow-up, the patient was asymptomatic and did not have esophageal stricture. His follow-up is still ongoing. The reporting of this study conforms to the CARE guidelines. 3

Chest radiograph (three-dimensional reconstruction) showing a metal bottle cap impacted at the T1–T2 cervical spine level (arrow).

Computed tomography scan of esophagus showing an impacted foreign object (arrow) in the esophageal lumen.

Computed tomography scan of the esophagus showing a foreign object in the esophageal lumen with the hypertrophy of the surrounding esophageal wall and ambiguous peripheral fat gap (arrow).
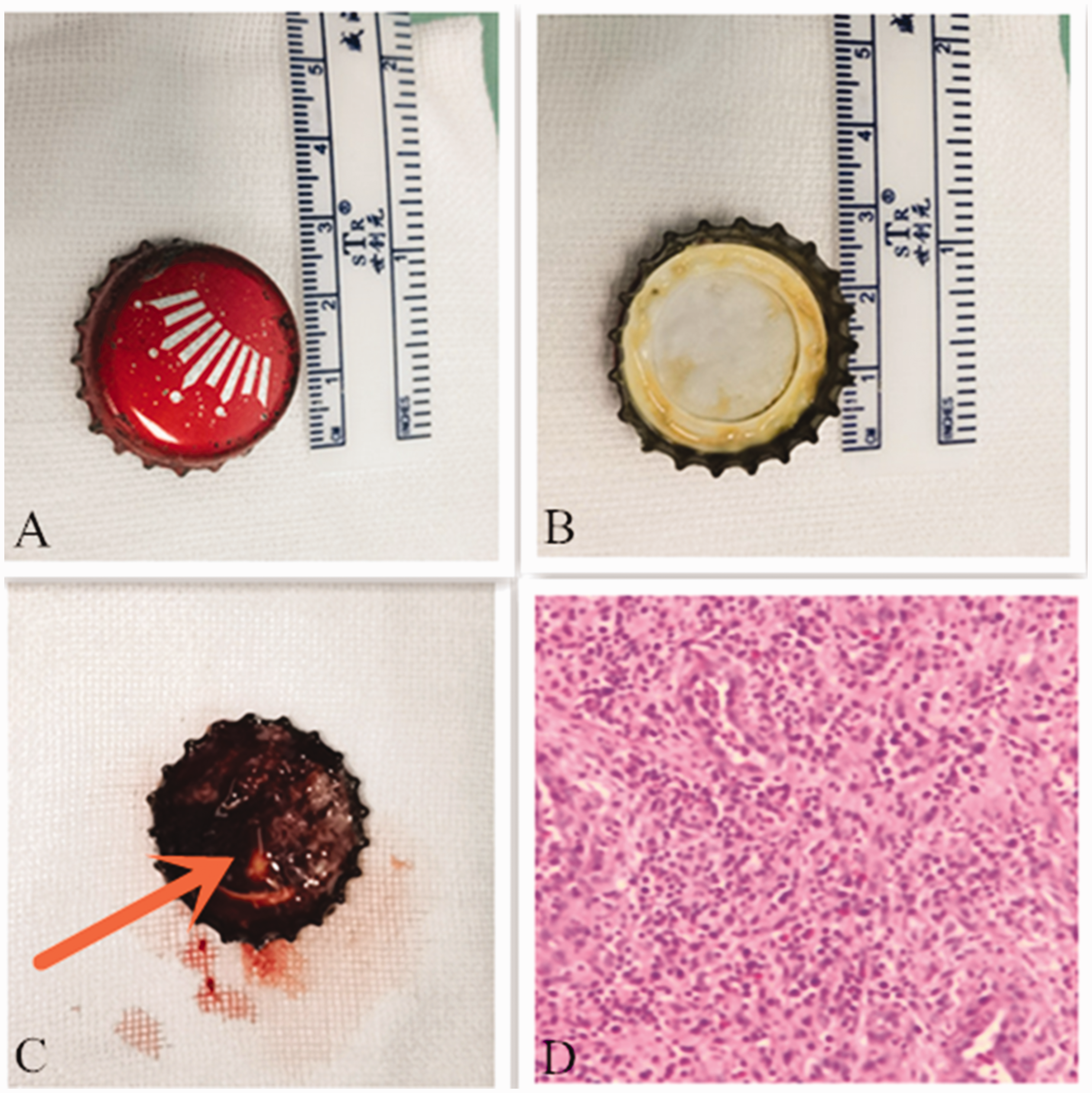
(a, b) Removal of a foreign body (metal bottle cap). (c) A large amount of granulation tissue can be seen inside the cap (arrow) and (d) Pathology shows inflammatory granulation tissue with inflammatory necrosis and mycobacteria.

Gastroscopy showing (a) longitudinal ulcers in the upper esophagus (left arrow), and (b) granulation tissue at the margin of the ulcers (right arrow) can be seen.
Discussion
The duration of FB impaction ranges from study to study, but most of them range from 0.25 to 192 hours.4–6 We describe the longest time a FB has been impacted in the esophagus in an adult patient. Gastrointestinal FB ingestion tends to be accidental in adults. Individuals with psychiatric or developmental difficulties, as well as those with social problems, are more likely to consume nonfood items. 4 Our patient did not have these problems, but his history was followed up and alcohol consumption was disclosed. Drinking may have clouded his judgment, and he failed to see the bottle cap in his wine glass. A clear history of FB ingestion is extremely important for reaching a rapid, definite diagnosis. However, our patient had an unwitnessed history of FBs. Because the FB showed incomplete obstruction, the patient’s symptoms were mild and he might have been able to eat food as usual. These are the reasons why a definitive diagnosis took a long time.
The types of FBs vary depending on dietary patterns, cultural characteristics, and sociocultural influences in different places.7–9 Bones, fish bones, and dental prostheses are the most common esophageal FBs found in adults. 2 FBs are primarily located in the esophagus, which is the upper part of the digestive tract.5,10 Most FBs are detected in the upper esophageal tract because it is the narrowest part of the esophagus, especially at the cricopharyngeal muscle. A beer bottle cap stuck in the esophagus is rare. We consider that the possible reasons for this finding in our patient are as follows: 1) while drinking, his brain was stimulated and the esophageal mucosa was insensitive; and 2) the teeth side of the cap was embedded in the narrowest part of the esophagus, along with wrapping of granulation tissue.
Depending on the size of esophageal FBs, they can partially or completely obstruct the esophagus. FBs can cause various symptoms, and retrosternal pain, dysphagia, and odynophagia are the most common symptoms in the adult population. 11 A patient with incomplete obstruction of a FB may have milder symptoms, but a patient with complete obstruction may suffer from difficulties swallowing liquids, excessive drooling, and even shortness of breath. Therefore, patients with complete obstruction need to have their FB urgently removed to avoid aspiration. 12 Moreover, ingestion of FBs is sometimes considered a serious medical condition because of possible complications, such as mucosal ulceration, esophageal perforation, mediastinitis, and vascular trauma.13–15 The impaction time of a FB is an independent risk factor for FB-related complications. As the time of impaction of a FB increases, there is a greater likelihood of perforation. However, in our case, surprisingly, the patient only developed esophageal ulcers. The sharpness of the object may also be a risk factor associated with adverse events, but more research on this possibility is required.
Plain radiography and an esophagram with barium are the traditional methods for detecting FBs because of their simplicity, convenience, and cost effectiveness. However, the low rate of diagnosis of plain radiography has resulted in its decreased clinical application. In addition, barium can enter the chest through an unknown perforation, thereby increasing the chance of infection. 16 In contrast, CT can show not only the presence of an impacted FB, but also its precise location, shape, size, and depth, the conditions of surrounding structures and soft tissues, and complications. However, receiving CT examinations to detect FBs may result in increased radiation exposure and a financial burden.
There has been much debate regarding the best methods to remove FBs. Gastroenterologists prefer flexible esophagoscopy. They believe that flexible esophagoscopy is a diagnostic and therapeutic tool with many advantages, such as avoiding the requirement for general anesthesia, technical facility, excellent visualization, and incidental diagnosis of other diseases. 1 However, otorhinolaryngologists advocate rigid esophagoscopy because the instruments used in this technique are larger and more powerful, and they can enlarge the space and easily grasp FBs. 6 Nevertheless, both approaches have their disadvantages. A flexible esophagoscope can barely grasp FBs that are located at the entrance of the esophagus. Rigid esophagoscopy has a limitation in patients who cannot lie down owing to a hunchback condition and in those who cannot endure general anesthesia.
Conclusion
Impaction of FBs in the gastrointestinal tract can lead to severe adverse events. Therefore, early detection and timely management of FBs are important. If no FB is found in the oropharynx or laryngopharynx that triggers pharyngalgia or an FB sensation, especially in those who drank alcohol, the esophagus should be examined or the patient should be followed up to avoid missing its diagnosis.
Research Data
Research Data for Long-term retainment of a foreign body in the esophagus in an adult: a case report
Research Data for Long-term retainment of a foreign body in the esophagus in an adult: a case report by Yong Li, Rongguo Wang, Qing Feng, Sai Zhang, Ce Wang and Xiaofei Song in Journal of International Medical Research
Footnotes
Author contributions
Study design: Rongguo Wang and Xiaofei Song.
Literature search: Qing Feng and Ce Wang.
Writing of the original draft: Yong Li.
Literature review and editing: Yong Li and Sai Zhang.
All of the data supporting the findings in this study are included in the published manuscript.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
The study protocol was approved by the ethics review committee of Hebei General Hospital (approval number: 202197). The patient provided written informed consent for publication.
Funding
The authors received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.