
Abstract
The entry of a metallic foreign body into the thyroid gland via the esophagus is a rare occurrence, with no previously reported cases. We present a 42-year-old woman who was admitted to hospital with right-sided neck pain, reporting that she had inadvertently swallowed a fish bone. She underwent laryngoscopy, which showed no fish bone in the throat, and no obvious bleeding in the bilateral tonsils and pear-shaped fossa. X-ray examination showed a needle-shaped foreign body in the neck, and a computed tomography scan of her neck showed a 0.1-cm diameter, 2.0-cm long foreign body in the right thyroid. She underwent emergency surgery and a needle of the corresponding size was found in the thyroid gland. This case demonstrates the importance of adequate preoperative assessment and an appropriate surgical approach for thyroid metallic foreign bodies.
Introduction
Foreign bodies in the neck, including metallic and non-metallic objects, is a relatively common clinical finding. 1 Most metallic foreign bodies (MFBs) encountered during both peace and wartime are shrapnel, projectiles, and iron filings, with maxillofacial foreign bodies being more common. 2 However, MFBs in the thyroid are rare, and to the best of our knowledge, this study represents the first such reported case. Emergency surgery is required because of the neck’s specific anatomy and the important physiological functions of the organs. 3 In the present study, we report on the diagnosis and management of a patient with a thyroid MFB, and review the relevant literature.
Case report
A 42-year-old woman was admitted to Shaoxing People’s Hospital (First Affiliated Hospital of Shaoxing University) with a 1-day history of right-sided neck pain due to a foreign body. The patient reported that she had inadvertently swallowed a fish bone 1 day before admission to hospital. Her neck pain did not disappear after drinking vinegar and eating vegetables, and even tended to increase, thus the patient came to hospital for treatment. Her temperature was 37.6°C, heart rate 76 beats/minute, respiratory rate 20 beats/minute, and her blood pressure was 116/75 mmHg. There was no redness or swelling of the neck skin and her thyroid was not visible in the neck. Palpation indicated mild tenderness of the right thyroid gland, with no obvious mass or enlarged lymph nodes in neck. The patient underwent laryngoscopy in the Emergency Department, which showed no fish bone incarceration in the throat, and no obvious bleeding in the bilateral tonsils or pear-shaped fossa. It was suspected that a foreign body might have penetrated the esophagus, and the patient was admitted to the Otolaryngology Department. The following day, she underwent esophagoscopy, which showed that the first 20 cm of the esophageal mucosa was smooth and rosy, with no bleeding spots, ulcers, or perforations, and no fish bones or other foreign bodies. However, X-ray examination showed a needle-shaped foreign body in the neck (Figures 1a, 1b), and a computed tomography scan of the neck showed a foreign body measuring 0.1 cm in diameter and 2.0 cm in length in the right thyroid (Figures 1c, 1d).

Imaging examination showing thyroid foreign body. X-ray of the lateral neck (a) and front neck (b) showing position of the foreign body (arrow). Non-enhanced (c) and enhanced (d) CT scans of the neck showing position of the foreign object (arrow).
After consultation, the patient was transferred to the Department of Breast and Thyroid Surgery for emergency surgery. During the operation, the tissues between the lateral side of the thyroid gland and the carotid artery were obviously adhered and a small ulcer was seen on the lateral surface of the right thyroid. The surrounding tissues were congested and edematous, but no obvious foreign bodies were observed. The upper and lower thyroid poles were freed to reveal the entire thyroid body and the thyroid gland was cut along the ulcer point, revealing a needle (diameter, 0.1 cm; length, 2.0 cm) in the gland (Figure 2). The patient’s family confirmed that this needle was used for scraping fish scales. The needle may thus have inadvertently punctured the fish and been swallowed when the patient ate the fish. The needle was very sharp, and repeated swallowing had caused it to pierce the esophagus and enter the right thyroid gland. A follow-up X-ray examination 2 days later showed no obvious foreign bodies in the neck, and the patient was discharged.
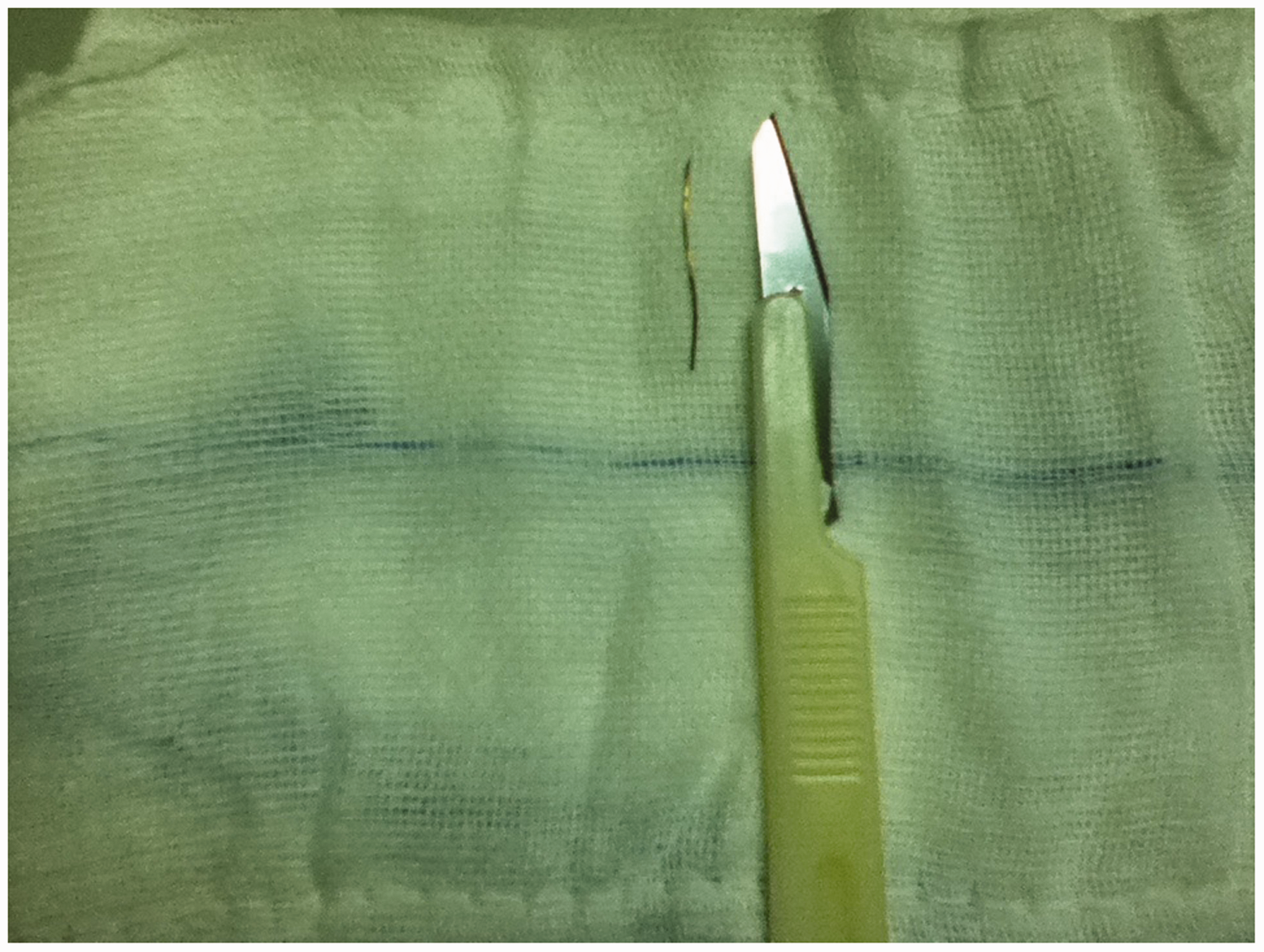
Metal foreign body removed from the thyroid gland (0.1 cm diameter, 2.0 cm long).
This study was approved by the Ethics Committee of the First Affiliated Hospital of Shaoxing University, Shaoxing People’s Hospital. The patient provided written consent for publication of this report.
Discussion
Cases of MFBs entering and remaining in the body are uncommon, and are mainly associated with trauma, medical accidents, medical implants, and ingestion. 4 In the current study, we present the first reported case of an MFB in the thyroid.
The neck contains important organs, including blood vessels, the recurrent laryngeal nerve, throat, trachea, esophagus, and mediastinum. 5 Entry of a needle into these organs may thus be extremely dangerous, resulting in potential infections, tracheal dysfunction, and even major bleeding.
Accurate preoperative localization of the needle was key to success in the current case. Various methods can be used to locate needles, such as X-ray examination and CT scans. X-ray examination is the most common method for locating MFBs, and is simple, practical, convenient, and economical, and CT scans can accurately locate MFBs, reconstruct the three-dimensional structure in the region, evaluate the risk of surgery, and thus provide a reliable basis for subsequent surgery. In the present case, X-ray examination and CT scanning were both used for preoperative evaluation of the three-dimensional structure of the foreign body.
Cases of foreign bodies entering the thyroid gland via the esophagus are rare. In this case, the patient had been eating fish and we suspected that a foreign body might have entered the esophagus, and investigated this possibility by routine laryngoscopy and esophagoscopy in the Emergency Department. However, surgery unexpectedly revealed a foreign body in the thyroid gland. This case highlights some issues regarding the diagnosis and treatment of this condition. Notably, swallowing fish bones is a very common incident, but if the fish bone is hard and sharp, it may pierce the esophagus wall and enter other tissues. The fish bone must be removed promptly because repeated swallowing of vegetables or rice balls may cause the foreign body to puncture deeper tissues or organs. In the case of a patient with symptoms of fish bone incarceration but normal laryngoscopy and esophagoscopy findings, it should be highly suspected that the foreign body has entered other tissues, and X-ray and CT examinations are required to determine the exact location of the foreign body. During the surgical removal of a foreign body, it is necessary to repeatedly touch the target organ by hand, especially if there is an ulcer on the surface, because the foreign body may be located below the ulcer.
Conclusion
The entry of MFBs into the thyroid gland via the esophagus is a rare occurrence, and should be treated in accordance with the general principles for treating foreign bodies in the neck. Adequate preoperative assessment using a combination of X-rays and CT scanning might be helpful. Surgery is likely to be necessary, and the surgeon should repeatedly touch the target organ, especially if there is an ulcer on the surface, to detect foreign bodies below the ulcer.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethical approval and consent to participate
This study was approved by the Ethics Committee of the First Affiliated Hospital of Shaoxing University, Shaoxing People’s Hospital. The patient provided written consent for publication of this report.
Funding
This study was supported by grants from the National Natural Science Foundation of China (grant no. 81341135), Shaoxing Bureau of Science and Technology (grant nos. 2017B70037 and 2017QN002).