
Abstract
Sclerosing stromal tumor of the ovary (SSTO) is a rare benign neoplasm of the ovary, accounting for about 6% of all sex cord stromal ovarian tumors. Only 17 cases of SSTO occurring during pregnancy have been reported to date. We report a case of SSTO occurring during pregnancy and review the existing literature. A 32-year-old pregnant woman was found to have a 10-cm solid mass in the right adnexa, and a large volume of ascites fluid was detected by ultrasound examination in the second trimester. The patient underwent abdominal puncture to relieve her symptoms in the second trimester, and a partial right oophorectomy and cesarean section were performed at 39 weeks of gestation. Final pathology confirmed the diagnosis of SSTO. Both the mother and baby were well at 6 months of postpartum follow-up. Clinical symptoms, and hormone and imaging examinations are all helpful in making a differential diagnosis of SSTO, but the unique histopathological and immunohistochemistry findings remain the main diagnostic features. Pregnant women with SSTO usually undergo enucleation or unilateral oophorectomy, which generally does not have adverse pregnancy outcomes.
Keywords
Background
Sclerosing stromal tumor of the ovary (SSTO) is a distinctive benign ovarian stromal neoplasm that was first described in 1973 by Chalvardjian and Scully. 1 It usually occurs in women in the second or third decades of life, with about 70% of reported cases occurring between 14 and 29 years of age. 2 Its occurrence is very rare, with fewer than 300 cases described in the literature to date. In addition, only 15 of the 208 SSTO cases reported between 2003 and 2014 occurred during pregnancy. 3 The condition is usually hormonally inactive, but tumors are occasionally either estrogenic or androgenic and virilization usually occurs during pregnancy.4–6 However, the exact pathogenesis of SSTO remains poorly understood.
Case presentation
A 32-year-old pregnant woman, gravida 1 para 0, presented at 16 weeks and 4 days of gestation with a 2-week history of progressive abdominal fullness and intermittent chest tightness. No pelvic tumor had been detected by pelvic sonography performed at 12 weeks of pregnancy, and there was no supporting information in the patient’s medical history or in her family history. A physical examination revealed a swollen abdomen with shifting dullness. Certain signs suggestive of virilization were detected, including acne, excessive hair growth, and a masculine voice. Tumor markers including cancer antigen (CA) 125 (9.10 U/mL, reference level <30.2 U/mL), CA199 (5.53 U/mL, reference level <37 U/mL), human epididymis protein 4 (27.32 pmol/L, reference level <140 pmol/mL), carcinoembryonic antigen (<0.50 ng/mL, reference level <5 ng/mL), squamous cell carcinoma (1.43 ng/mL, reference level <2.50 ng/mL), neuron-specific enolase (0.73 ng/mL, reference level <16.3 ng/mL), alpha fetoprotein (36.20 IU/mL, reference level <6.7 IU/mL), and other laboratory indicators including estradiol 2 (>3000.0 ng/L) showed no obvious abnormalities. Ultrasound examination revealed an intrauterine pregnancy at 16 gestational weeks and a large volume of ascites fluid. A solid mass measuring 10.3 × 9.2 × 7.1 cm with a central cyst was found inside in the right adnexa, and low-velocity and low-resistance blood-flow signals were identified around the mass. There were no obvious abnormalities in the uterus or the left ovary.
Because of progressive ascites and an enlarged right ovary, the patient received hypervolemic treatment for a few days, considering a possible diagnosis of ovarian hyperstimulation syndrome. However, her clinical symptoms failed to improve. She then underwent percutaneous peritoneal drainage and pathological examination, but no obvious malignant tumor cells were found in the ascites fluid. The immunohistochemical results of the ascites fluid are shown in Table 1. Ascites fluid was drained every day until the daily drainage was minimal. The total volume of drained ascites was about 5000 mL. Regular check-ups showed no tumor enlargement and no return of ascites. Notably, there was a slight transient elevation of serum CA125 levels to 35.66 U/mL during weeks 27 to 29 of gestation.
Immunohistochemical results for ascites and right ovary in the patient with sclerosing stromal tumor of the ovary.

CR, human calretinin; PR, progesterone receptor; CD, cluster of differentiation; SMA, smooth muscle actin; WT1, Wilms tumor protein-1; AE1/AE3, cytokeratin AE1/AE3; MPO, myeloperoxidase; CgA, chromogranin; MC, mesothelial cells; L, lymphocytes; H, histiocytes; P, partial; n, nuclei; c, cytoplasm.
Pelvic ultrasound at 39 weeks of pregnancy revealed a cystic-solid mass measuring 10.3 × 7.8 × 7.9 cm in the right adnexa with honeycomb-like cyst cavities (Figure 1a). Exploratory laparotomy and cesarean section were suggested and were accepted by the patient because of a suspected ovarian malignancy. A uniformly enlarged cystic-solid right ovary with no other abnormalities was identified (Figure 1b). Pathological examination of a frozen section suggested a benign ovarian tumor (luteoma of pregnancy or microcystic stromal tumor). Cesarean section and partial right oophorectomy were therefore performed at 39 weeks and 4 days of pregnancy because of the high possibility of a benign tumor and the strong desire of family members to retain the remaining ovarian tissue. The remaining mass is shown in Figure 1c. A healthy male baby was born, and the surgical specimen was submitted for further pathological evaluation.

Ultrasound, gross images, and diagram of sclerosing stromal tumor of the ovary (SSTO) presenting in pregnancy. (a) Ultrasound showed a 10.3 × 7.8 × 7.9-cm solid mass in the right adnexa with multi-cystic structure in the wall and center. Sparse blood-flow signals were observed around the ovary. (b) Exploratory laparotomy view of a solid mass in the right adnexa (rhombus) and the uterus (triangle). (c) The remaining mass after partial right oophorectomy (outline by arrows). Star indicates the cystic space. (d) Gross examination of SSTO revealing a primarily solid tumor with grayish-white or grayish-yellow areas with local multi-cystic changes and (e) Diagram of SSTO presenting in pregnancy.
The patient showed elevated serum testosterone levels (>15 ng/mL, reference level: 0.09–0.48 ng/mL) after the operation. Pathological diagnosis based on paraffin sections revealed a sclerosing stromal tumor of the right ovary. Examination of the removed mass showed a tumor measuring 10.5 × 10.0 × 3.0 cm, and the cut surface had a locally grayish-white, grayish-yellow, medium-quality, granular, and multi-locular cystic appearance (Figure 1d). A schematic of the SSTO presenting in pregnancy is shown in Figure 1e. The right ovary was uniformly enlarged with an uneven surface and the tumor could not be completely distinguished from normal ovarian tissue. A large cavity inside the right ovary contained clear serous fluid. On microscopic examination, the tumor had pseudo-lobular structures of different sizes and irregular shapes, with hypercellular areas separated by edema-like hypocellular areas. The lobular architecture of the tumor was separated by loose edematous regions, alternating with hypocellular and hypercellular areas. Round and short spindle cells were predominant within the hypercellular areas. Some of the tumor cells were rich in eosinophilic cytoplasm or contained vacuoles, with the appearance of “signet-ring-like” cells, and the nuclei were oval, centered, or deviated from their usual morphology. No cytologic atypia was observed, although low levels of mitotic activity were noted. The background stroma, especially in the hypocellular areas, contained abundant collagen and blood vessels, some with “staghorn” (branching) morphology scattered throughout the tumor (Figure 2). The immunohistochemical assay findings are shown in Table 1, and the results of immunochemical staining of tumor tissue are shown in Figure 3.
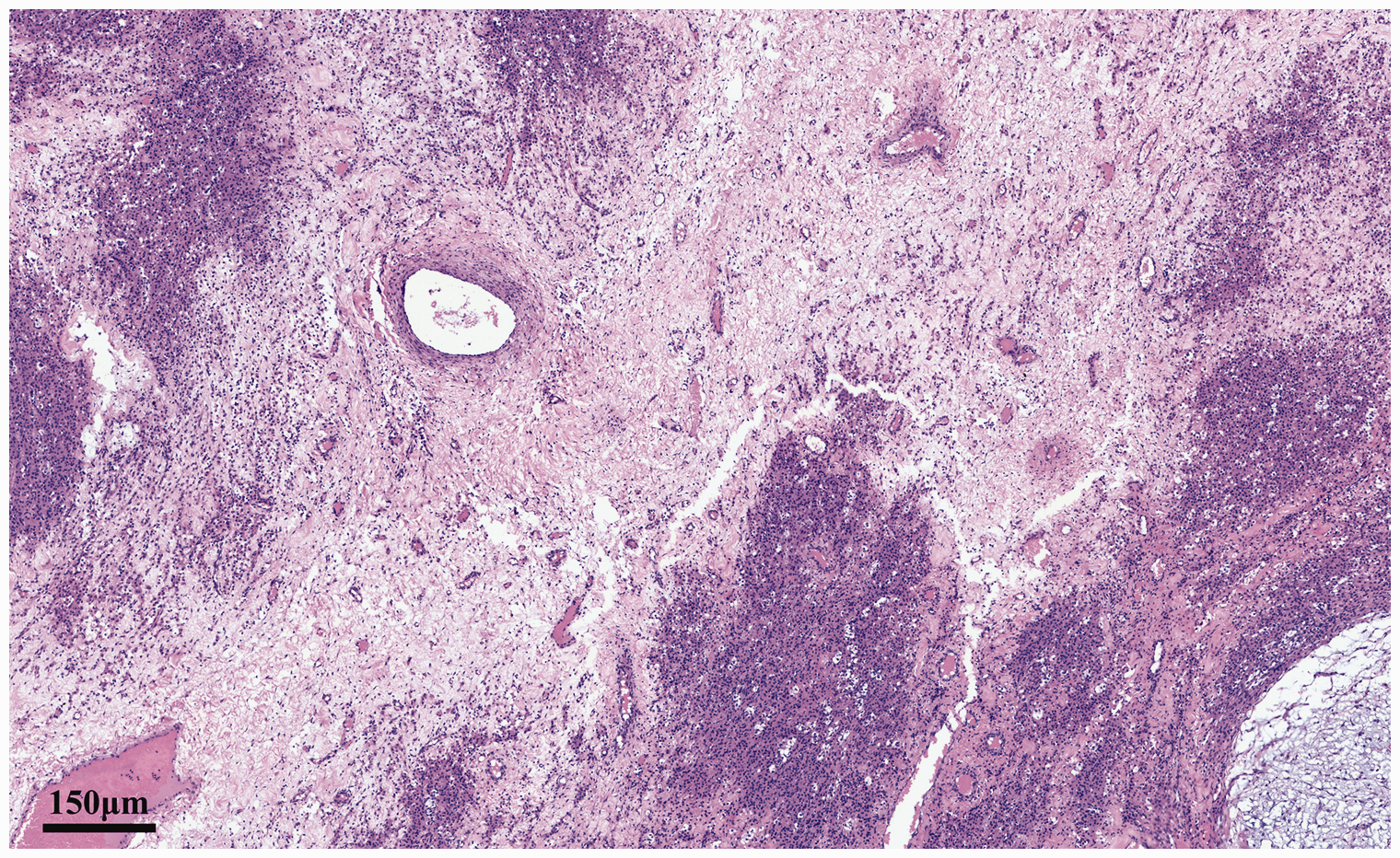
The tumor had pseudo-lobular structures of different sizes and irregular shapes, and hypercellular areas were separated by edema-like hypocellular areas. (Hematoxylin and eosin staining; magnification ×40).
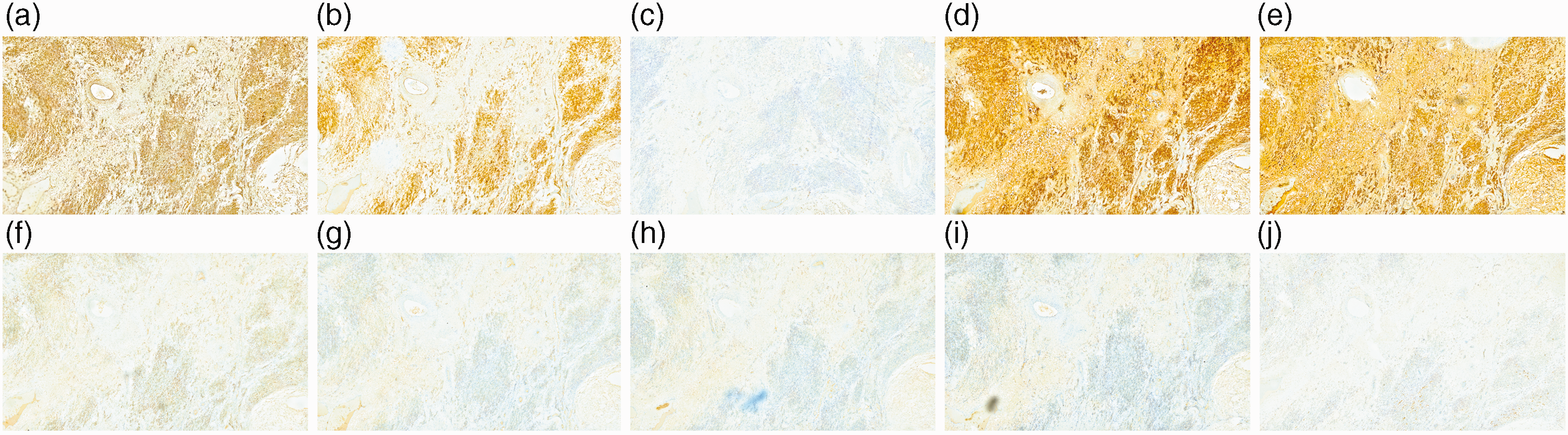
Immunohistochemical results of sclerosing stromal tumor of the ovary. Tumor cells were positive for vimentin (a), β-catenin (b), cyclin D1 (c), inhibin-a (d), human calretinin (e), progesterone receptor (f), smooth muscle actin (g), Ki-67 (h), and Wilms tumor protein-1 (i), and negative for CD10 (j). (All images magnification ×40).
The patient did well postoperatively. Pelvic ultrasound at 3 days after surgery revealed a 9.6 × 6.4 × 4.8-cm solid mass in the right adnexa and pelvic fluid with a maximum depth of 2.8 cm, and an 8.0 × 5.0 ×3.1-cm solid mass, but no ascites at 42 days after surgery (Figure 4). Virilization, including excessive hair growth and a masculine voice, was significantly reduced at telephone follow-up 6 months after the operation. Both mother and baby were doing well.

Ultrasound showed a 9.6 × 6.4 × 4.8-cm solid mass in the right adnexa with multi-cystic structure (outlined by plus signs). Triangle indicates the uterus.
The reporting of this study confirms to CARE guidelines. 7
Discussion
SSTO is a rare benign subtype of ovarian sex cord stromal tumor accounting for <5% of all cases of sex cord stromal tumors. SSTO frequently occurs in patients in their 20 s and 30 s, whereas other stromal tumors of the ovaries typically occur in patients in their 50 s and 60 s.8,9 The common clinical symptoms of SSTO include menstrual irregularity, pelvic pain, and non-specific symptoms associated with the ovarian mass, and the vast majority of cases occur unilaterally.8,9
SSTO is usually hormonally inactive, but some cases of SSTOs with hormone activity (predominantly estrogen effects; rarely androgenic effects) have been reported, which resolved following surgery.3,8,10 Dehydroepiandrosterone produced by active tumors causes menstrual irregularity, amenorrhea, infertility, precocious puberty, and virilization, 3 with virilization even noted in some pregnant women.4,5,11–13 Cases of ascites and elevated CA125 also have been reported.2,3 The observed symptoms in some patients may be complicated by the presence of Gorlin–Goltz syndrome or Meig’s syndrome. 11 Our patient presented with ascites fluid and virilization, and although raised testosterone levels were only measured after surgery, the patient’s masculine signs suggested that they had also been elevated prior to the operation. The mechanism underlying the clinical features of SSTO, including virilization and ascites, has yet to be fully elucidated, although several researchers have discovered some important details. For example, the hormone production might be associated with the stimulation of stromal lutein cells by human chorionic gonadotropin during pregnancy,14,15 while the production of ascites and CA125 could be associated with the stimulation of mesenchymal cells.16,17 Additionally, Samanth et al. suggested that the mechanism of peritoneal effusion formation might be the same as that for fibroma, given that SSTO comprises a subgroup of thecoma-fibromas. 18 The most likely pathogenesis of ascites might ascribe the fluid formation to the filtration of interstitial fluid in the peritoneum through the tumor capsule, which does not have the capability of resorption, while the hormonal milieu created by steroid production during pregnancy might aggravate this transudative mechanism.
Although some studies documented the development of a steroid-producing SSTO following clomiphene treatment for infertility in a patient whose ovaries had been laparoscopically normal prior to treatment,19,20 many patients with SSTO had no history of clomiphene treatment. In addition, there is a lack of evidence suggesting that the progression of SSTO is related to pregnancy. The pathogenesis of SSTO thus remains a mystery.
We performed a literature search of the PubMed and Medline databases (search performed on 5 September 2021) using the keywords “sclerosing stromal tumor” and “pregnancy” to identify relevant studies, and extended the search to studies in the reference lists of the identified articles. The characteristics of 17 cases reported between 1979 and 2019 are summarized in Table 2.3–6,13,21–29
Sclerosing stromal tumor of the ovary cases occurring during pregnancy in the literature.
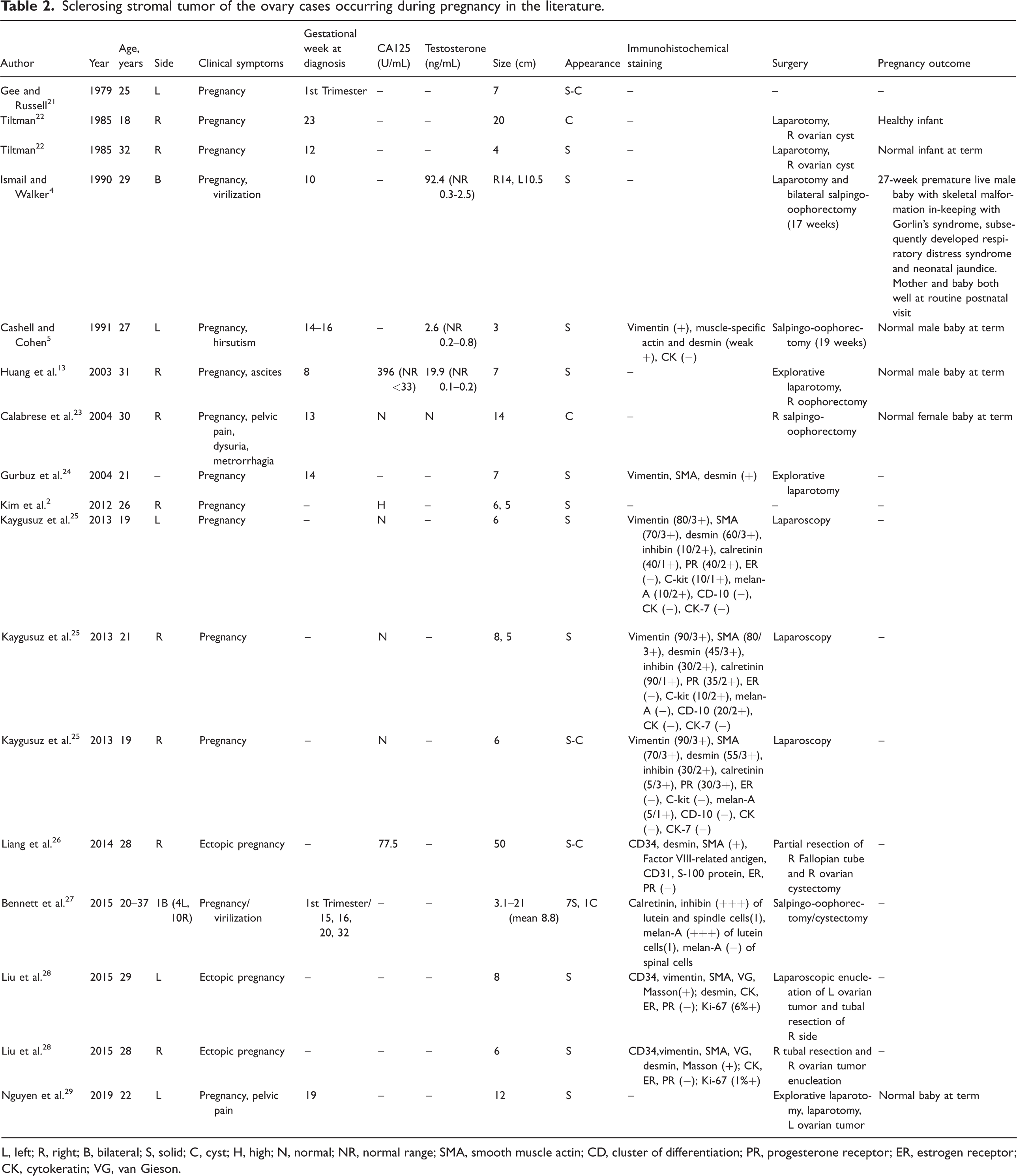
L, left; R, right; B, bilateral; S, solid; C, cyst; H, high; N, normal; NR, normal range; SMA, smooth muscle actin; CD, cluster of differentiation; PR, progesterone receptor; ER, estrogen receptor; CK, cytokeratin; VG, van Gieson.
The presence of SSTO cannot be predicted preoperatively based on clinical symptoms and ultrasonographic findings alone, and it is difficult to distinguish SSTO consisting of solid and cystic areas from ovarian malignancies based on radiological and macroscopic examinations. In addition, SSTOs occasionally appear to be highly vascular, making the differential diagnosis more difficult. Computed tomography and magnetic resonance imaging can be helpful in the diagnosis of SSTO,30,31 but pathological features remain the main factors contributing towards a diagnosis of SSTO. SSTOs typically present as a solid or cystic mass with an intact membrane. Tumors can vary greatly in size, may be single, multi-cystic, or have a honeycomb-like structure, and usually have a smooth surface. Tumor sections are generally mostly solid and grayish-white, with focal yellow areas and areas of edema. One characteristic histological finding of SSTO is the pseudo-lobular pattern consisting of cellular nodules separated from each other by hypocellular, edematous, and collagenous stroma. Cellular areas are characterized by hemangiopericytoma-pattern-like, dilated vascular structures, whereas hypercellular areas are typically characterized by luteinized theca-like cells with vacuolized cytoplasm and fusiform fibroblast-like structures. 32 The characteristic pathological findings of SSTO were observed both macroscopically and microscopically in all the cases reported in the literature.3–6,13,21–29 In addition, focal calcification in the interlobular areas, dense eosinophilic infiltrate, signet-ring cells, and hyalinization were also seen in some cases of SSTO during pregnancy.23,25,27,29
Most cases of SSTO can be diagnosed correctly based on the clinical context and recognition of characteristic histological features, while immunohistochemical staining can also be used in difficult cases. Several immunohistochemical markers of sex-cord stromal tumors have been studied in SSTO, and immunohistochemical analyses of formalin-fixed and paraffin-embedded materials for inhibin, smooth muscle actin, vimentin, and estrogen and progesterone receptors revealed predominant positivity for smooth muscle actin, consistent positivity for inhibin and vimentin, and negativity for S-100 protein and epithelial markers, suggesting a stromal origin of SSTO. 32 In addition, inhibin, the melanocytic differentiation marker melan-A, calretinin, CD34, alpha glutathione S-transferase, Müllerian-inhibiting substance, Wilms tumor protein-1, and CD99 have all been reported to be useful for differentiating SSTOs from thecomas, fibromas, and other sex cord stromal tumors.4,32
In addition, clinicians who encounter ovarian tumors with hyperandrogenemia are more likely to consider the possibility of steroid cell tumor (SCT). SCT is another rare sex cord-stromal tumor, mostly solid, which can also appear during pregnancy and is difficult to distinguish from SSTO. 33 However, SCTs are generally composed of granular eosinophilic or vacuolated cytoplasm, which is often positive for fat stains. Staining for inhibin and calretinin are generally high, 34 while SCTs are mostly negative for epithelial membrane antigen. 35
Because SSTOs may be accompanied by ascites and virilizing symptoms, they are difficult to differentiate from fibromas, thecomas, Krukenberg tumors, and other ovarian sex cord-stromal tumors with sclerosis. 36 Surgery is therefore usually performed after diagnosis. Unilateral salpingo-oophorectomy with peritoneal surgical staging is a safe alternative to radical treatment in non-pregnant patients who desire to preserve fertility. 37 All the reported SSTOs in pregnant patients were diagnosed in the first or second trimester, and enucleation or unilateral oophorectomy was usually performed (Table 2). Seven of the fifteen patients underwent laparoscopic surgery and the rest underwent open surgery, and almost all the pregnant women who were followed up delivered normal healthy babies.5,13,21–23,29,38 Most studies suggested that abdominal surgery during pregnancy was better performed during the second trimester, and that laparoscopic surgery itself did not increase pregnancy complications. The effect of appropriate laparoscopic surgery on the fetus was not significantly different from that of open surgery, and may even be preferable to open surgery, given that laparoscopic surgery has the advantages of less trauma, fast recovery, and less disturbance to the intestine and uterus.39–41 However, pregnancy may increase the incidence of some surgical complications regardless of the type of surgery, such as hernia, skin infection, bleeding, and visceral injury. 42 In addition, appropriate drugs should be used to prevent abortion and premature birth after surgery.
Given that SSTO has been reported to have a low risk of recurrence, and because the family members in the present case strongly requested preservation of the remaining ovarian tissue, the patient underwent ovary-sparing surgery, with a favorable clinical outcome. Although the patient showed no clinical signs of residual tumor growth within 6 months after surgery, we will continue to follow her up. To the best of our knowledge, this case represents the first report of a partial right oophorectomy in a pregnant woman with SSTO. Although the patient refused an ultrasound re-examination, no obvious signs of recurrence were noted within 6 months of follow-up. This case suggests that ovary-sparing surgery may be suitable for young women with SSTO. In addition, bilateral SSTO, although very rare, is usually treated with bilateral salpingo-oophorectomy in patients with severe clinical symptoms, 4 and ovary-sparing surgery may also be attempted in these patients, although there is currently no literature to support this hypothesis.
In conclusion, SSTO is a very rare benign neoplasm of the ovary, with a small number of cases occurring during pregnancy. Clinical symptoms, tumor markers, and hormone, ultrasound, and imaging examinations are all helpful in terms of the differential diagnosis of SSTO, but its unique histopathological and immunohistochemistry findings remain the main diagnostic features. Intraoperative frozen sections can be used to confirm the benign nature of the tumor, and ovary-sparing surgery may also be considered. In addition, neither SSTO itself nor its timely surgical treatment in pregnant patients generally result in adverse pregnancy outcomes.
Footnotes
Acknowledgements
The authors thank The Second Affiliated Hospital of Dalian Medical University, for their support of this work and the reviewers for allowing us to make improvements to the manuscript.
Author contributions
LXW conceived the study. LXW and XC performed the operation and follow-up of the patient. XZ and YW created the figures and tables. XC and XZ drafted the article and LXW revised it critically. All authors reviewed the manuscript and approved the version to be published.
Data availability statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
All treatments were carried out with written informed consent from the patient and her family members. The patient also signed informed consent for the publication of articles related to her medical records. The study protocol was approved by the Ethics Committee of The Second Affiliated Hospital of Dalian Medical University.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.