
Abstract
Fibrothecomas are mostly benign ovarian tumors. We describe a rare case of fibrothecoma in a 59-year-old woman with a history of recurrent massive ascites and postmenopausal bleeding. Over 2 years she has undergone more than 50 paracenteses with 8–11 L withdrawn each time. She presented with a newly diagnosed pelvic mass and bilateral hydrosalpinges demonstrated on ultrasound and were confirmed with computed tomography. The pelvic magnetic resonance imaging showed a large complex cystic mass arising from the left ovary measuring 16.6 × 12.1 × 8.6 cm3 with an area of irregular mural enhancement. The patient underwent left salpingo-oophorectomy with benign frozen section results. The final pathology was consistent with cystic degeneration of fibrothecoma
Introduction
Ovarian fibromas and fibrothecomas are rare ovarian sex cord-stromal tumors. They account for 1% to 4.7% of ovarian tumors. 1 Fibromas and fibrothecomas are considered the most common solid primary tumors of the ovary. 2 The thecoma-fibroma group is a spectrum of benign ovarian tumors including fibroma, fibroma-thecoma, and thecoma, depending on the relative proportion of fibroblasts and theca cells. 3 An accurate preoperative diagnosis is often difficult because of its uncommon occurrence. Fibrothecomas are stromal tumors containing lipid-laden cells similar to those of theca-interna and may have some degree of fibroblasts. If the tumors cannot be differentiated between fibroma and thecoma, they are named as fibrothecoma. 4 An ovarian fibrothecoma can be associated with ascites and hydrothorax, known as Meigs’ syndrome. 1 Fibrothecomas are hormonally active ovarian neoplasms. A high level of estrogen, menstrual disorders, and vaginal bleeding are observed in patients with fibrothecoma. 3 The treatment is surgery and the follow-up is a must until full recovery. 5 Here we present an unusual presentation of the case of middle-aged females presented with a lower abdominal mass and postmenopausal bleeding associated with recurrent massive ascites.
Case report
The patient is a 59-year-old female G3P3003 who presented with postmenopausal bleeding, increased abdominal fullness, as well as massive ascites that required over 50 paracenteses with 8–11 L withdrawn every other week over 19 months before her presentation. The patient was followed at that time by surgery then was referred to gynecology team after she had postmenopausal bleeding. The patient had a computed tomography (CT) imaging at the time of the first presentation with ascites followed by magnetic resonance imaging (MRI) and another CT, all reveled only mild hepatomegaly and ascites and no mass at the time. The fluid cytology from the paracenteses was always benign. Her previous surgical history includes three cesarean sections, bilateral tubal ligation, three exploratory laparotomies, and two liver biopsies. She also underwent a transjugular intrahepatic portosystemic shunt (TIPS) procedure about a year before presentation. The gynecology team was not involved in the management of the patient until the latest presentation before the procedure.
Physical examination at the time of presentation is normal. She underwent a workup including (1) ultrasound which revealed a large cystic left ovarian mass and bilateral hydrosalpinges (Figure 1); (2) endometrial biopsy was done and the pathology results were benign; (3) pelvic CT confirmed a large pelvic mass; and (4) a pelvic and abdominal MRI with and without contrast that showed a large complex cystic mass arising from the left ovary measuring 16.6 × 12.1 × 8.6 cm3 with an area of irregular mural enhancement concerning for malignancy and bilateral hydrosalpinges. There was no evidence of abdominopelvic lymphadenopathy (Figure 2).
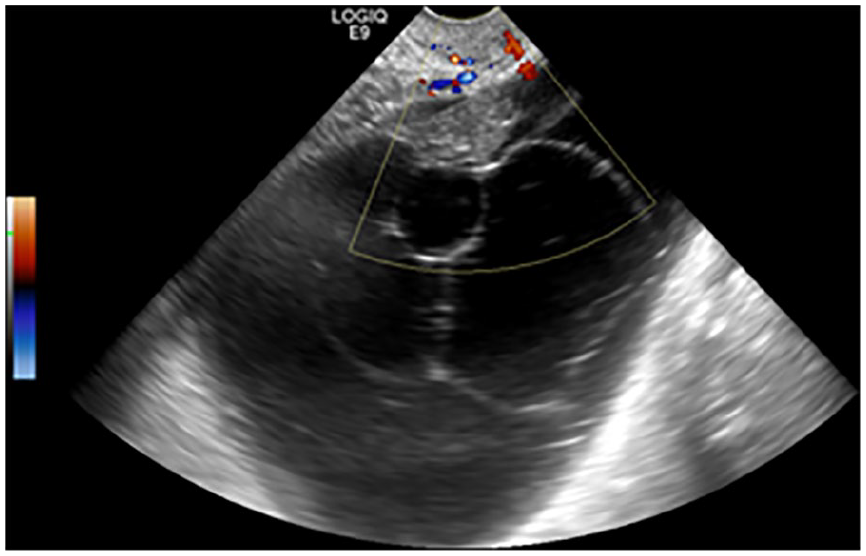
Pelvic ultrasound showing large complex left adnexal cystic mass.

(a) MRI showing large complex cystic left ovarian mass (blue arrow) and fibroid uterus with submucosal fibroids (red arrow). (b) MRI showing left hydrosalpinx (green arrow). (c) MRI sagittal view of the mass and uterus.
Prior the surgery, Carcinoembryonic Antigen (CEA) was 2.21 ng/mL (<2.5 ng/mL) and CA-125 was 20.7 kU/L (0–35 kU/L). The assessment of the consulted gyn-oncology team concerned the risk of malignancy low and deemed on standby is sufficient. The size of the mass was quite large and since the diagnosis (benign vs malignant) was not secured, preference was to remove the mass intact and avoid any spillage into the peritoneal cavity in case it is malignant. The patient underwent a dilation, curettage, and exploratory laparotomy with left salpingo-oophorectomy and right salpingectomy. Ascites were noted and washings were taken and sent to pathology for permanent section. The intraoperative finding was large cystic adnexal mass involving the left fallopian tube and ovary. The peritoneum was noted to be thick. A frozen section revealed fibrothecoma. Gyn-oncology service was consulted and agreed to proceed with excision and frozen section pathology assessment. They were on standby if the intraoperative pathology consultation reveals malignant diagnosis.
Final pathologic diagnosis revealed the following: endometrial curetting consisted of a block with fragments of benign squamous epithelium, endocervical glands, and stromal fragments, and no evidence of malignancy; the right fallopian tube was dilated with hydrosalpinx; and left ovarian mass presented with fibroatheroma with a benign associated cyst, most consistent with cystic degeneration of fibrothecoma. On gross inspection, the excised left ovary consisted of a tan/red large cyst measuring 18 × 13 × 7.3 cm3 and weighs 882 g. The external surface was smooth and the section reveals rubbery, tan-yellow, solid area measuring 7 × 2.5 × 1.8 cm3. The cyst was filled with clear yellow fluid. The right fallopian tube appeared dilated measuring 3.0 cm in length and 1.5 cm in maximal diameter. A portion of the fallopian tube was filled with a tan-yellow gelatinous substance.
The patient had an uneventful post-operation course and met all discharge criteria on post-operative day 2. In the most recent follow-up, 3 years postsurgical, the patient did not have any recurrent ascites since she had the surgery. The CT scan at the time did not show any abnormal findings.
Discussion
Ovarian fibromas and fibrothecomas are rare ovarian tumors of gonadal stromal cell origin. They account for 1% to 4.7% of ovarian tumors. 1 These tumors are unilateral in about 90% of the cases and rarely malignant. 6 They may be pure and non-secreting or associated with thecoma elements (fibrothecoma), sometimes responsible for estrogen secretion. 5 They are composed of spindle, oval, or round cells forming variable amounts of collagen. Because of these intersecting bundles of spindle cells, collagen, and hyalinized tissue, 6 the tumor has a white whorled appearance resembling uterine leiomyoma on gross examination. The tumor may be spherical or lobulated and is covered by intact ovarian mucosa. 7 Fibrothecomas are more common in older postmenopausal women. 8 They may be associated with Meigs’ syndrome, consisting of hydrothorax and ascites. 7 In a recent publication, the authors reported a patient’s ascites reversed few months after the removal of the ovaries for the suspicion of atypical Meigs’ syndrome, even though they concluded that the problem is not clear. 9 The tumor markers (CA-125 serum levels) are usually normal. However, high serum levels may be initially detected, and they become normal after tumor removal. 10 In the case, presented here, we believe that the early imaging has missed the developing ovarian cyst at the time of early diagnosis and it has not been repeated until the latest presentation before the procedure which showed the left ovarian mass. Hence, we conclude the fibrothecoma should be investigated as a differential for this presentation.
Conclusion
Fibrothecoma should be investigated and excluded from the differential diagnosis of recurrent ascites in postmenopausal women. Women with chronic ascites the ovaries should be continuously investigated as they can be initially normal at image and gynecological examination and a slow-growing fibrothecoma is part of the differential diagnosis. Early diagnosis and treatment can improve clinical outcomes, prevent exposure to multiple paracentesis procedures, and avoid long-term complications.
Footnotes
Author contributions
A.E. contributed to clinical data collection, and drafting and writing of the manuscript; S.B. contributed to clinical data collection and manuscript editing; H.E. contributed to review of literature preparation and manuscript editing; and A.A-H. performed the surgery and manuscript review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.