
Abstract
Primary tracheobronchial schwannoma is extremely rare. A woman in her early 60 s was admitted to our department with a 2-month history of cough and expectoration. Chest computed tomography (CT) revealed a high-density nodule at the opening of the right main bronchus, accompanied by atelectasis in the middle and lower lobes. Flexible bronchoscopy revealed a tumor at the opening of the bronchus of the right middle lung lobe, which protruded into the main bronchus. A high-frequency electrosurgical snare, endobronchial cryosurgery, and argon plasma coagulation (APC) were used under rigid bronchoscopy. Histopathological examination diagnosed the tumor as schwannoma. The patient’s symptoms resolved after the operation. Follow-up chest CT showed that the right main bronchus was unobstructed, and the bronchus of the lower lobe was open. Bronchoscopic interventional therapy is an alternative treatment for tracheobronchial schwannoma.
Keywords
Introduction
Schwannomas are benign neoplasms that arise from Schwann cells. These tumors can develop in peripheral nerves, mediastinum, retroperitoneum, posterior spinal nerve roots, and cerebellopontine angle. 1 Schwannomas in the respiratory system usually involve the chest wall and posterior mediastinum. 1 Primary tracheobronchial schwannoma is extremely rare; only approximately 0.2% of all bronchopulmonary tumors are tracheobronchial schwannomas. 2 In this report, we describe a case of bronchial schwannoma in an adult.
Case report
A woman in her early 60 s presented with chief complaints of cough and expectoration of approximately 2 months’ duration. Her body temperature was normal on examination. Her medical history included type 2 diabetes mellitus, and blood glucose control was acceptable. She had no history of smoking. Lung sounds were decreased on auscultation of the right lung; other general physical examination findings were normal. The erythrocyte sedimentation rate (ESR) was 95 mm/h, and the levels of inflammatory biomarkers and tumor markers were within normal limits.
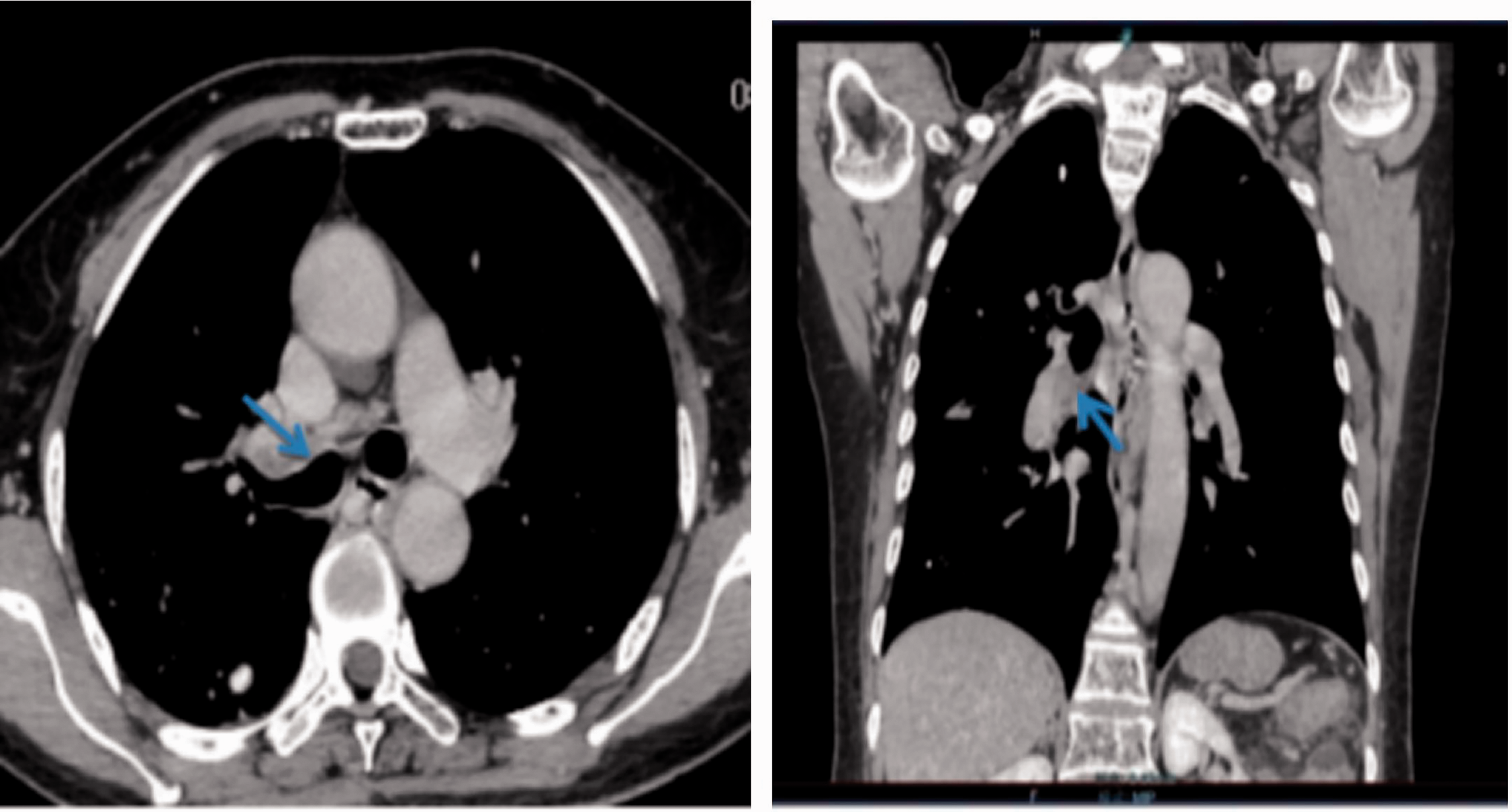
Chest computed tomography (CT) revealed a high-density nodule at the opening of the right main bronchus, accompanied by atelectasis in the middle and lower lung lobes (Figure 1). Flexible bronchoscopy was performed and revealed that the opening of the bronchus of the right middle lung lobe was covered and obstructed with a white soft tissue mass. The tissue protruded into the right main bronchus and resulted in stenosis of the right main bronchial lumen (Figure 2). Biopsy of the soft tissue mass was performed, and histopathological examination revealed chronic inflammation of the bronchial mucosa. No malignant cells were seen.

Chest computed tomography images showing a high-density nodule in the right main bronchus, accompanied by atelectasis in the middle and lower lung lobes (left image: axial view; right image: coronal view).

Flexible bronchoscopic images showing that the opening of the bronchus of the right middle lung lobe is covered and obstructed with a white soft tissue mass. The mass protruded into the right main bronchus and resulted in stenosis of the right main bronchial lumen (left image). A high-frequency electrosurgical snare, endobronchial cryosurgery, and APC were used with under rigid bronchoscopy (right image).
With the initial histopathological results and the patient's consent, we performed bronchoscopic interventional therapy. A high-frequency electrosurgical snare, endobronchial cryosurgery, and argon plasma coagulation (APC) were used under rigid bronchoscopy. The tumor was debulked, and the opening of the bronchus of the right lower lung lobe was clear after treatment; however, the opening of the bronchus of the middle lobe was still partially obstructed. On macroscopic evaluation, the tumor capsule was complete, and the tumor measured approximately 4 × 2 × 1 cm. Postoperative pathology revealed that the tumor was composed mainly of cell-dense Antoni A tissue arranged in a palisade, with Verocay body-like structures. Focal Antoni B areas were seen, with few cells and a disordered arrangement. Immunohistochemistry was positive for S-100 and SOX10 (Figure 3) and negative for smooth muscle actin (SMA) protein antibody. These histological and immunophenotypical features were consistent with schwannoma.

Postoperative histopathology showing that the tumor is composed mainly of cell-dense Antoni A tissue arranged in a palisade, with Verocay body-like structures. Focal Antoni B areas are seen, with few cells and a disordered arrangement (left image; HE stain, ×400). Immunohistochemistry was positive for S-100 (central image; ×100) and SOX10 (right image; ×100).
The patient’s clinical symptoms resolved after the operation. Follow-up chest CT showed that the right main bronchus was unobstructed, and the opening of the bronchus of the right lower lung lobe was open. A high-density shadow was seen in the right middle lung lobe bronchus, accompanied by atelectasis (Figure 4). Follow-up flexible bronchoscopy 10 days after treatment revealed that the opening of the bronchus of the right lower lung lobe was clear, the right main bronchus was unobstructed, and the opening of the bronchus of the right middle lobe was still obstructed. No new mass was identified in the right lower lobe (Figure 5).
Follow-up computed tomography images after the operation showing that the right main bronchus is unobstructed, and the bronchus of the lower right lung lobe is open. A high-density shadow is visible in the right middle lung lobe bronchus, accompanied by atelectasis (left image: axial view; right image: coronal view).

Bronchoscopic images showing that the right main bronchus is unobstructed (left image). The opening of the bronchus of the right lower lung lobe is exposed, and the opening of the bronchus of the right middle lung lobe is still obstructed after bronchoscopic interventional surgery (right image).
Discussion
Primary tracheal tumors originate most often from the mucosal epithelium and glands at the junction between the membranous wall and cartilage. 2 These tumors are rare and generally malignant. 2 Squamous cell carcinoma and adenoid cystic carcinoma account for the majority of primary tracheal tumors. 2 Benign tumors account for approximately 0.5% of all intratracheal tumors.2,3 Among the benign tumors, neurogenic tumors are even rarer and include neurofibromas and schwannomas. 3
The first case of bronchial schwannoma was reported in 1951 as a single tumor with a smooth capsule and nodular shape. 4 Bronchial schwannomas grow slowly and rarely become malignant.4,5 Primary tracheal schwannoma is common in adults, and occurs mostly in Asian populations, with a slightly higher incidence in women.2,5 Tracheal schwannoma can occur in any area of the tracheobronchial tree, with intraluminal or extraluminal extensions.1,6 The clinical symptoms are nonspecific, with most patients presenting with progressive dry cough, dyspnea, fever, and signs of obstructive inflammation.2,6 Symptoms are associated with the size and location of the tumor and the presence or absence of airway obstruction. 6 Symptoms are absent in the early stage and appear only when the tumor obstructs the bronchial lumen. 7 Tracheobronchial schwannoma has no specific symptoms or findings with tracheoscopy, and the diagnosis cannot be made on clinical presentation alone.6,7 These tumors are easy to misdiagnose as asthma or carcinoma, as well as benign lesions, such as tuberculosis (TB), inflammatory pseudotumor, and leiomyoma. 7 Further differential diagnosis is needed. In our case, we found a soft tissue mass in the lumen of the main bronchus, accompanied by luminal stenosis and atelectasis of the middle and lower lobes of the right lung. However, without tissue biopsy, we could not differentiate tracheobronchial schwannoma from other endobronchial tumors.
Currently, there are no treatment guidelines for tracheobronchial schwannomas; therefore, choosing the best treatment is difficult. Surgery may be the first choice; however, interventional therapy under bronchoscopy has been used in benign tracheobronchial tumors and has been proven safe and effective.8,9 Tracheobronchial schwannomas grow slowly, have a low probability of recurrence after resection, and can be treated bronchoscopically.1,4 However, studies of bronchoscopic interventional therapy to remove schwannomas are limited. 10 Ge et al. 1 reviewed 51 cases of primary tracheal schwannoma from 1950 to 2013; 19 patients underwent endoscopic resection and 29 underwent surgical resection. Four cases underwent a second surgery after bronchoscopy. Among the seven cases of bronchial schwannoma reported by Jung et al., 11 five cases were treated under tracheoscopy, and the tumors were completely removed without recurrence. Bronchoscopy has proven to be a very effective tool for the treatment of schwannoma.9,12 Flexible bronchoscopy is often used to identify the location and size of the tumor, and the degree of obstruction of the bronchial lumen. 13 Rigid bronchoscopy is an approach for both benign and inoperable malignant central airway tumors. In the present case, rigid bronchoscopy permitted curative therapy. The main advantages of rigid bronchoscopy are the possibility of manipulating multiple instruments, good safety profile, and the possibility of sustained ventilation. 14 Rigid bronchoscopy alone or in conjugation with a high-frequency electrosurgical snare, endobronchial cryosurgery, and APC is effective, quick, and safe for central airway tumor therapy. 14
The choice of conservative vs surgical treatment for tracheobronchial schwannomas is complex. Some studies report that if the lesion is large, centrally located, and complicated by obvious pneumonia, lobectomy may be necessary; normally with favorable outcomes. 15 In our case, no signs of malignancy were found in the histology of the initial biopsy, and the primary site was intraluminal, with growth into the bronchus of the middle lung lobe. Considering these findings, a high-frequency electrosurgical snare, endobronchial cryosurgery, and APC were used under rigid bronchoscopy. The patient’s clinical symptoms resolved after treatment, and the opening of the bronchus of the lower right lung lobe was clear. However, the right middle lung bronchus was still obstructed 10 days after the operation. We planned to treat the remaining obstruction by tracheoscopy after the patient recovered from the first surgery; however, owing to economic concerns and because her clinical symptoms had resolved, the patient refused follow-up chest CT and bronchoscopy. She is still under follow-up, with no symptoms.
In conclusion, tracheobronchial schwannoma is rare. If the patient's respiratory symptoms worsen, chest CT and bronchoscopy should be performed as this approach is helpful for early diagnosis. Bronchoscopic interventional therapy is an alternative treatment for tracheobronchial schwannoma.
Footnotes
Acknowledgement
We acknowledge the technical assistance of Wang Ying.
Author contributions
Guo Lina and Hou Pengguo provided the full data for this case report. Guo Lina and Sun Junping took responsibility for the integrity and accuracy of the data analysis. Xiao Zhihua and Sun Junping performed the bronchoscopic examination. Bai Baoqin performed the pathological analysis. Guo Lina, Sun Junping, Zhang Mingyue, and Wang Jianxin performed the literature review. All authors provided final approval of the manuscript.
Data availability statement
All data in this study are included in the article. Further enquiries can be directed to the corresponding author.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statements
The reporting of this study conforms to the CARE guidelines. 16 This case report contains no details regarding the patient's identity; we obtained the patient's written consent for treatment. Ethical approval was not required for this study, in accordance with national guidelines.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.