
Abstract
Pulmonary nodules are usually considered to be associated with malignant tumors and benign lesions, such as granuloma, pulmonary lymph nodes, fibrosis, and inflammatory lesions. Clinical cases of pulmonary nodules associated with hemophagocytic lymphohistiocytosis have rarely been reported. Therefore, when patients develop pulmonary nodules, the possibility of developing hemophagocytic lymphohistiocytosis is often not considered. We report the first case of familial hemophagocytic lymphohistiocytosis with recurrent pulmonary nodules as the first symptom. Our findings will hopefully provide new ideas for the diagnosis and treatment of pulmonary nodules in the future.
Keywords
Introduction
With the increasing development of imaging technology and attention paid to lung cancer, the detection rate of pulmonary nodules is increasing. Pulmonary nodules are lesions with a round diameter (<30 mm) in the lungs, with clear or blurred edges. 1 Pulmonary nodules are divided into ground glass nodules, confounding nodules, and solid nodules according to the density. 2 The formation of nodules can be influenced by various factors. Generally, inflammation, tuberculosis, and bleeding lead to benign nodules. Malignant nodules are formed by lung metastasis of primary lung cancer or malignant tumors. 1 However, few clinical cases associated with hemophagocytic lymphohistiocytosis (HLH) have been reported. 3 As a type of HLH, familial hemophagocytic lymphohistiocytosis (FHL) is a rare autosomal recessive inherited hematological disorder. 4 Patients with FHL show extra-hematological involvement that commonly involves the nervous and hepatobiliary system, and rarely involves the respiratory system (except for co-infections). 5 We report the first case of adult FHL with recurrent pulmonary nodules as the first symptom. We hope that this report can provide some new insight into the diagnosis and treatment of pulmonary nodules and FHL.
Case Report
We report a case of a female patient in her early 30 s who was clinically healthy. She had wandering nodules and patchy exudation as shown by chest computed tomography (CT) for 2 years, accompanied by chest pain and respiratory difficulties.
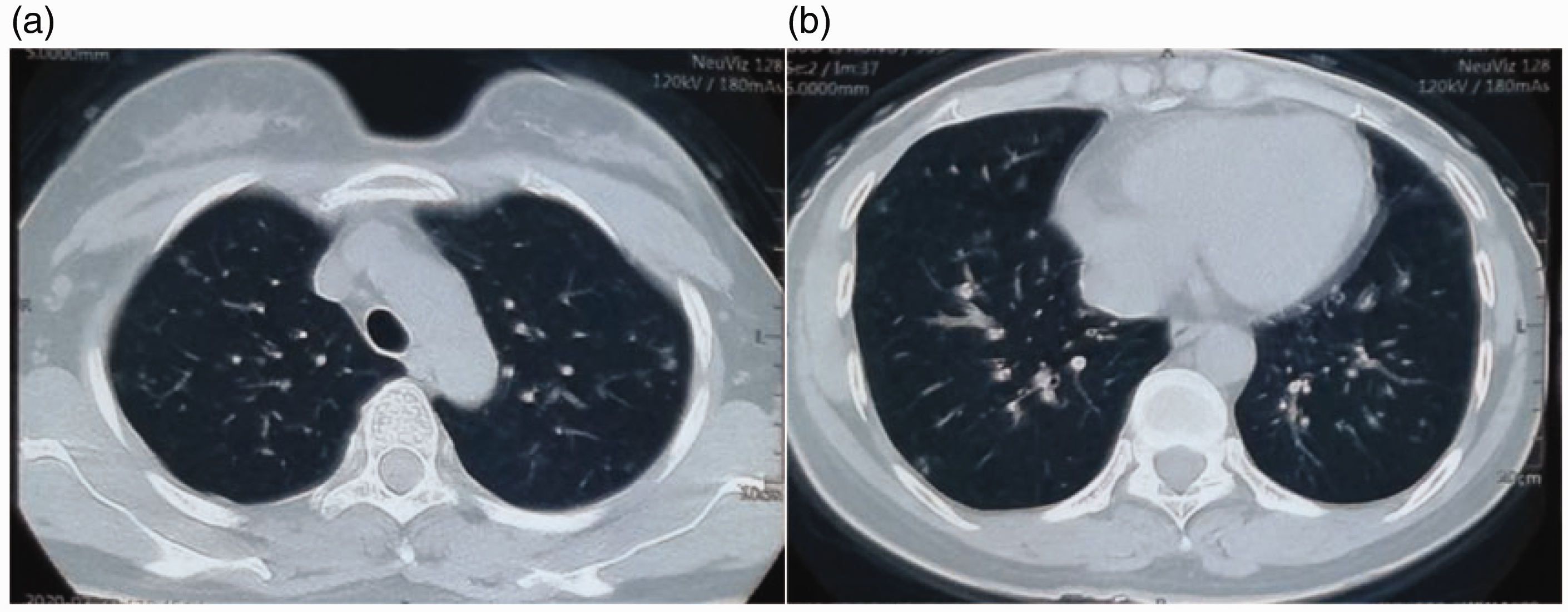
In January 2020, the patient was admitted to our hospital with chest pain and respiratory difficulties, which had occurred for 1 month. A comprehensive in-patient evaluation showed an elevated immunoglobulin M rheumatoid actor concentration (22.7 U/mL, normal: 0–18 U/mL), abnormal chest CT findings (multiple nodules and patchy exudations) (Figure 1), and other results were negative. She received anti-infective treatment, but the treatment failed (Figure 2). The patient did not undergo a percutaneous lung biopsy because her family refused an invasive puncture. Combined with her elevated immunoglobulin M rheumatoid actor concentration, we considered a possible combination of immune-related lung injury. Therefore, we started treatment with prednisone. This therapy was effective (Figures 3, 4), but her symptoms recurred after withdrawal (Figure 5).

Chest computed tomography shows the first appearance of symptoms in the patient. Multiple nodules and patchy exudates can be seen.

Chest computed tomography shows no absorption of the nodules after using empirical antibiotics.
Computed tomography shows that the patient has enlarged lesions after she decided to stop taking prednisone for the first time.

Chest computed tomography shows some absorption of the lesions after the first prednisone therapy.

Computed tomography shows a reduced lesion volume after prednisone therapy.
One month after her second spontaneous withdrawal of prednisone (March 2021), a chest CT (Figure 6) showed multiple high-density shadows, nodular shadows, and mediastinal lymph nodes again. A culture and next-generation sequencing of the alveolar lavage fluid showed Aspergillus fumigatus growth. Various factors suggesting an immunity imbalance were observed, such as elevated cytokines and imbalanced lymphocyte subpopulations (Table 1). After antifungal therapy with voriconazole, absorption of the lesions on chest CT lesions was not obvious (Figure 7). The patient was treated again with prednisone, and her chest CT findings improved (Figures 8–10).

Computed tomography shows an increased volume of multiple nodules and plaque exudates after the second discontinuation of prednisone therapy.
Levels of cytokines and lymphocyte subsets before and after the familial hemophagocytic lymphohistiocytosis outbreak.

IL, interleukin; TNF, tumor necrosis factor; NK, natural killer.

Computed tomography does not show considerable absorption of the lesions after switching to antifungal therapy.

Computed tomography shows absorption of the lesions in the patient after using prednisone therapy combined with antifungal therapy.

Computed tomography shows an improvement in the lesions compared with a few months previously because of taking regular medication

Computed tomography shows absorption of the lesions after continuous treatment
On 30 December 2021, the patient had a persistent fever (temperature: 38.5°C) with myalgia. She was treated with the antibiotics with no symptomatic relief. A physical examination showed a 6-cm palpable enlarged spleen below the costal margin and bilateral cervical lymph nodes. Laboratory examination results were abnormal, including pancytopenia and elevated liver enzymes ect. (Tables 1 and 2). Chest CT showed that the nodules were increased again (Figure 11). A bone marrow biopsy showed a small amount of hemophagocytosis and poorly differentiated histocytes (Figure 12). She also had low natural killer cell activity (1.30%). The diagnosis of HLH was made, and the patient was transferred to the Hematology Department for supportive treatment with HLH-2004 chemotherapy. After 2 weeks, the patient's symptoms had resolved (Figure 13). We found that the patient had mutations in PRF1 by genetic testing (Table 3). After investigating the physical condition of her family, we found that her brother had died of hematological disease (unknown). Her final diagnosis was FHL2.
Trend in related laboratory indicators since the onset of familial hemophagocytic lymphohistiocytosis.

ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALP, alkaline phosphatase; GGT, gamma-glutamyl transferase.

Computed tomography shows that the range of imaging lesions has expanded and increased in density after symptoms of persistent fever, muscle soreness, and pancytopenia.

Results of a bone marrow examination.

Computed tomography shows that the lesions have absorbed in the patient after treatment with the HLH-2004 regimen.
Gene sequencing results of the index case.

The patient had a homozygous mutation of the PRF1 gene.
dbSNP, Single Nucleotide Polymorphism Database; AR, autosomal recessive; FHL2, familial hemophagocytic lymphohistiocytosis 2.
We obtained consent for treatment and written informed consent for publication from the patient. The study was approved by the Ethics Committee of the Second Hospital of Shanxi Medical University (batch number: 2022, no. (157) YX). The reporting of this study conforms to the CARE guidelines. 6
Discussion
The definition of a pulmonary nodule is pulmonary opacity up to 30 mm in diameter. Pulmonary nodules are a common finding in routine clinical practice in performing chest imaging tests. These tests include radiographs or CT for any reason. Approximately 80% to 90% of these nodules are benign, and only a small proportion (approximately 10%–20%) are malignant. 7
Lung nodules with recurrent lung shadows do not belong to the imaging-specific manifestations of a certain category of diseases, which include lung infections, autoimmune diseases, and other lung diseases. Because of the lack of specificity, the diagnosis of this disease cannot be made according to the time and the extent of the nature of the lesion. Patients with signs of wandering shadows in the lungs should have pathogen infection excluded. In the long-term diagnosis of patients with an unclear diagnosis, a lung puncture biopsy is necessary for defining the nature of wandering nodules in the lung. 8
Our patient had an auxiliary examination performed, which did not show any pathogenic bacteria. The anti-infection treatment effect was not effective in the patient, and there was an immune imbalance. Therefore, we considered that she had an immune-related lung injury. We performed glucocorticoid therapy on the basis of immune-related lung injury because a percutaneous lung biopsy was not performed to determine the nature of the lesion. The patient's clinical symptoms gradually improved after this therapy and the pulmonary nodules were gradually absorbed. However, because recurrent infections with Aspergillus led to the colonization of Aspergillus, the patient had an aggravated immune imbalance, which eventually led to the outbreak of FHL.
HLH is a group of diseases belonging to histiocytosis syndrome. HLH is defined as a condition involving a sustained immune/inflammatory reaction, also known as a “cytokine storm”. 9 HLH is triggered by inborn errors of metabolism, infections, or malignancy.10–12 There are multiple diseases that can mimic the clinical manifestations of HLH, such as idiopathic multicentric Castleman’s disease. 13 The main clinical manifestations of HLH are unremitting high fever, pancytopenia, liver/splenomegaly, and other types of organomegaly, liver dysfunction, coagulopathy, and elevation of typical HLH biomarkers. The diagnosis of HLH is based mainly on clinical and laboratory criteria, specifically HLH-2004 criteria, which are available and primarily applied in practice. 14 FHL is a genetically heterogeneous disorder caused by mutations in genes involved in the secretory lysosome-dependent exocytosis pathway. 15 FHL subtypes include FHL1 to FHL5, but the pathogenic genes for FHL1 remain unknown. The genes specific for types 2 to 5 are PRF1, UNC13D, STX11, and STXBP2. 16 PRF1 encodes a cytolytic effector perforin expressed by T cells and natural killer cells. 17 Perforin is essential for the cytotoxicity of natural killer cells, CD8+ cells, γδ+ cells, and regulatory T lymphocytes, and perforin can induce apoptotic cell death in response to granzyme. Perforin/granzyme is the main pathway of cytotoxicity to control infection and transform cells. Interruption of this pathway leads to persistent inflammation, chronic antigen presentation, and the release of inflammatory mediators. 18
Glucocorticoids are steroid hormones produced by the adrenal cortex, which broadly regulates inflammatory, metabolic, and stress responses. In the treatment of immune disorders, glucocorticoids regulate anti-inflammatory and immune regulation effects by inhibiting the function of various inflammatory cells and inflammatory mediators.19,20 After our patient decided to discontinue prednisone, her symptoms recurred, which were relieved after adding prednisone. A. fumigatus is a fungal pathogen that can cause devastating pulmonary infections in individuals suffering from an immune imbalance or underlying lung conditions. 21 Aspergillus infection can also cause or aggravate the immune imbalance. 22
We believe that, because of mutation of the PRF1 gene in our patient, she had a genetic immune response disorder. Persistent chronic inflammation and repeated stimulation of inflammatory mediators caused immune-related damage in her lungs. Conventional anti-infection treatment could not improve her symptoms. Therefore, prednisone was administered to regulate the absorption of lesions. A. fumigatus in alveolar lavage fluid with next-generation sequencing and culture was found in the patient during the second hospitalization. We also suspected that the patient’s lung lesions might have been caused by a fungal infection. Therefore, we attempted to stop prednisone therapy and switch to antifungal therapy. Unfortunately, the lung disease was not alleviated (Figure 7). When prednisone was added again, the nodules greatly shrank (Figure 8). Therefore, the persistent immune imbalance in the patient led to the Aspergillus infection, which also aggravated the immune imbalance in the patient, ultimately leading to the outbreak of FHL. After receiving chemotherapy with the HLH-2004 regimen, she showed improvement in her clinical and imaging findings. To cure the FHL clinically, the patient has been preparing for hematopoietic stem cell transplantation from the human leukocyte antigen to match her sister.
Our patient, who had a long course of disease, presented with recurrent, multiple, nodular lesions of the lungs before presenting with definite clinical manifestations of FHL2. The lung shadows were absorbed after prednisone treatment. Because of disorder of the genetic immune response, patients with FHL may initially show clinical manifestations of immune damage in other parts outside of the blood circulation. Therefore, in patients with recurrent pulmonary nodules, not only factors such as infection and a tumor should be considered, but we also should pay attention to the possibility of immune-related diseases. Especially in high-risk patients (a family history of disease), physicians should be aware of immune-related diseases, strengthen regular testing, and improve genetic screening. In this manner, the diagnosis of FHL can be made in time to avoid a delay in treating the patient’s condition.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231199019 - Supplemental material for Repeated pulmonary nodules as the primary symptom of familial hemophagocytic lymphohistiocytosis in adults: a case report and review
Supplemental material, sj-pdf-1-imr-10.1177_03000605231199019 for Repeated pulmonary nodules as the primary symptom of familial hemophagocytic lymphohistiocytosis in adults: a case report and review by Lulu Zhang, Chuanchuan Dong, Qiannan Wu, Yupeng Li, Liting Feng, Yanqing Xing, Yangdou Dong, Le Liu, Xiaohui Li, Rujie Huo, Yanting Dong, Erjing Cheng, Xiaoyan Ge and Tian Xinrui in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231199019 - Supplemental material for Repeated pulmonary nodules as the primary symptom of familial hemophagocytic lymphohistiocytosis in adults: a case report and review
Supplemental material, sj-pdf-2-imr-10.1177_03000605231199019 for Repeated pulmonary nodules as the primary symptom of familial hemophagocytic lymphohistiocytosis in adults: a case report and review by Lulu Zhang, Chuanchuan Dong, Qiannan Wu, Yupeng Li, Liting Feng, Yanqing Xing, Yangdou Dong, Le Liu, Xiaohui Li, Rujie Huo, Yanting Dong, Erjing Cheng, Xiaoyan Ge and Tian Xinrui in Journal of International Medical Research
Footnotes
Acknowledgements
We thank the patient for her participation and her consent to publish this report. we would also present my thankness towards Li Yaoyao, who has polished the essay and contributed to the accuracy in English.
Author contributions
Lulu Zhang was responsible for writing the manuscript and translation. Chuanchuan Dong, Qiannan Wu, Yupeng Li, Liting Feng, Rujie Huo, Yangdou Dong, and Yanqing Xing were responsible for the retrieval of relevant cases and information. Le Liu, Xiaohui Li, Yanting Dong, Erjing Cheng, and Xiaoyan Ge were responsible for collecting the patient’s data. Xinrui Tian helped write the manuscript and provided academic guidance. All authors contributed to writing of the manuscript.
Data availability statement
Data for this study are available from the corresponding author.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was funded by the Key Research and Development Project of Shanxi Province (201903D421066) and by the Basic Research Project of Shanxi Province (202203021211029).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.