
Abstract
Plastic bronchitis (PB) is a rare and potentially fatal disease characterized by acute progressive dyspnea caused by bronchial casts in the bronchial tree. We analyzed two children with asthma and PB who presented with high fever, cough and dyspnea. Both cases showed acute onset and rapid disease progression. Laboratory examination revealed that both children were infected with influenza A virus. Emergency fiberoptic bronchoscopy was performed within 20 hours of admission. Immediately after removing the bronchial casts, their dyspnea symptoms improved significantly, and they recovered after comprehensive treatment with antiviral drugs, antibiotics and glucocorticoids. When children with asthma have acute progressive and difficult-to-relieve dyspnea after infection with influenza A virus, clinicians should be aware of the possibility of PB and perform bronchoscopy as soon as possible to facilitate early diagnosis and treatment and improve patient prognosis.
Introduction
Plastic bronchitis (PB) is an acute and serious disease in which endogenetic foreign bodies partially or extensively block bronchi and form branched mucinous bronchial casts, leading to partial or complete pulmonary ventilation dysfunction, dyspnea, respiratory failure and even death.1,2 With the popularization of bronchoscopy technology, the diagnosis and treatment rate of this disease have been improved. Infection is a common cause of PB, especially in children with basic diseases. The common pathogens reported include adenoviruses and mycoplasma.2,3 After the global influenza A outbreak in 2009, Chikako Terano first published a report on PB in children with a history of wheezing related to H1N1 influenza infection that same year. 4 Since then, there have been few reports on children with asthma infected with influenza A virus complicated with PB. Here, we report two cases of PB in children with asthma infected with influenza A virus in our hospital and share our diagnosis and treatment experiences.
Case 1
The reporting of this study conforms to CARE guidelines. 5
A 4-year-old boy was admitted to our hospital after a 1-day history of fever, cough and dyspnea. On the day of admission, he had a cough, wheezing, fever, shortness of breath, 94% oxygen saturation, decreased breath sounds of the left upper lung and moist rales. The white blood cell (WBC) count was 11.9 × 109/L, and the percentage of neutrophils was up to 90%. A chest radiograph showed atelectasis of the left upper lung (Figure 1a). The boy was previously diagnosed with bronchial asthma but was not receiving any regular treatment and was still experiencing intermittent wheezing attacks. He received supplemental oxygen and antimicrobial treatment on admission. The day after admission, fiberoptic bronchoscopy was performed. During the operation, the left upper bronchi were obstructed with yellow-white mucus casts, and plastic casts were removed (Figure 1b). The symptoms of dyspnea significantly improved, and his oxygen saturation increased to 98%. Pathological examination of plastic casts revealed inflammatory necrotic tissue with a large number of neutrophils, mononuclear phagocytes and a small number of eosinophils (Figure 1c). Multiple reverse transcription-polymerase chain reaction (RT-PCR) analyses of sputum and alveolar lavage fluid indicated positive influenza A virus H1. We added oseltamivir to the treatment regimen. On the 9th day after admission, his clinical symptoms were relieved. Routine blood examinations were normal, but a chest radiograph showed bronchitis (Figure 1d). The correct asthmatic treatment plan was given to the patient at discharge. The boy remained in good health and continued regular asthma treatments after 3 months and 6 months of follow-up.
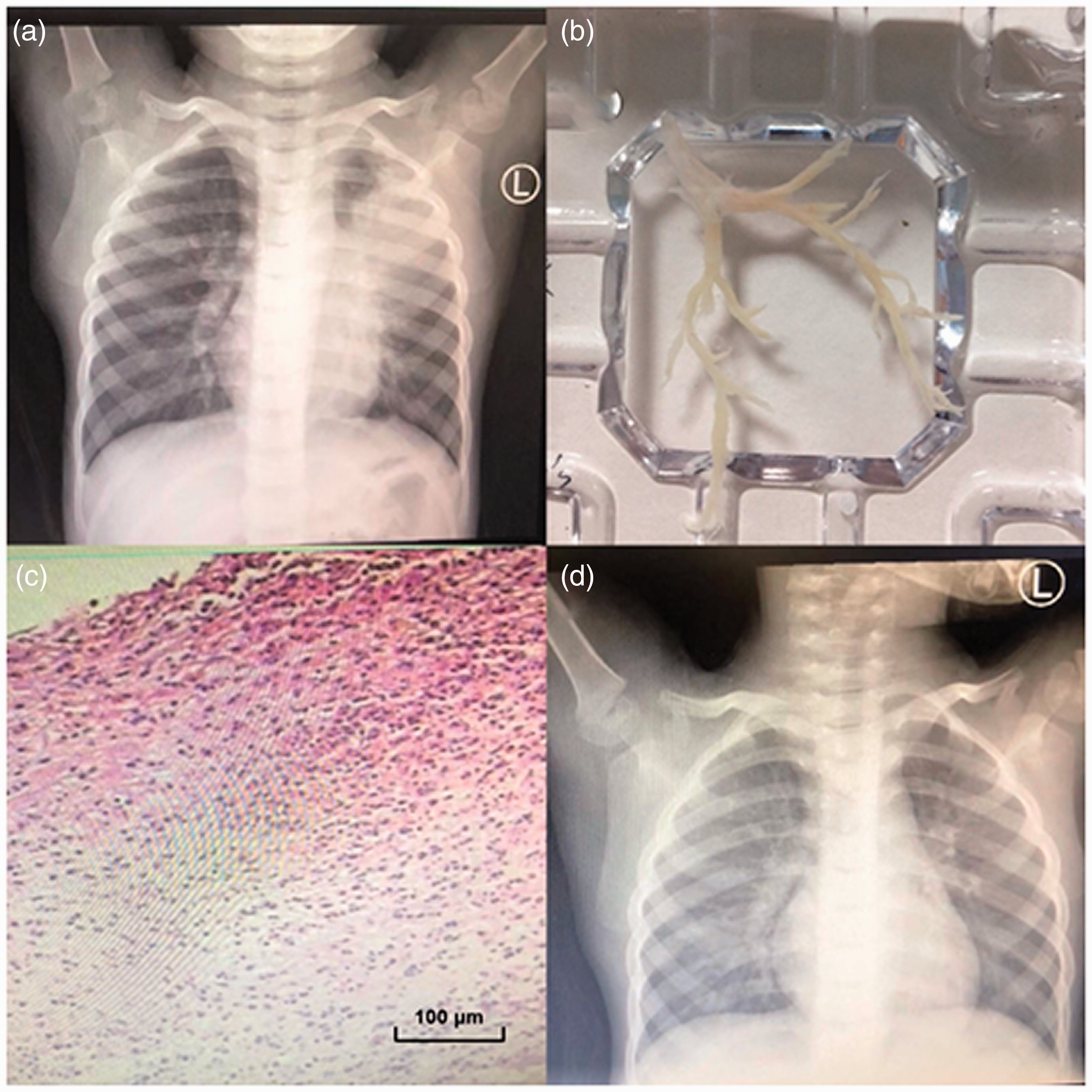
Clinical findings for the 4-year-old boy reported in case 1. (a) Chest radiograph on admission shows atelectasis of the left upper lung. (b) Cast removed from the left upper lung. (c) Hematoxylin and eosin examination of plastic casts showed inflammatory necrotic tissue with a large number of neutrophils, mononuclear phagocytes and a small number of eosinophils. Bar = 100 µm. (d) After treatment, the left pneumonia lesions had absorbed.
Case 2
An 8-year-old boy with a history of improper treatment for asthma presented to the hospital with a 1-day history of fever, cough and dyspnea. On arrival, he exhibited wheezing, fever, shortness of breath and 90% oxygen saturation. We administered 3 L of high-flow nasal cannula therapy. On physical examination, the breath sounds of his left lung had almost disappeared, and wheezing was heard in the right lung. The WBC count was 16.5 × 109/L, the percentage of neutrophils was 84%, and the C-reactive protein level was 34.22 mg/L. Chest computed tomography (CT) showed double pneumonia, obstruction of the left main bronchus, emphysema in the left upper lung and atelectasis in the lower lung (Figure 2a). The day after admission, fiberoptic bronchoscopy was performed. During the operation, a thick and tough plastic cast was removed from the left principal bronchus, and a dendritic plastic cast was removed from the middle lobe of the right lung (Figure 2b). Pathological examination of plastic casts revealed inflammatory necrotic tissue with a large number of eosinophils, mononuclear phagocytes and a small number of neutrophils (Figure 2c). Multiple RT-PCR analyses of sputum and alveolar lavage fluid indicated positive influenza A virus H1. Sputum culture indicated Haemophilus influenzae. We administered oseltamivir, antibiotics, glucocorticoids and other treatments. Although his symptoms improved significantly, the boy showed mucus casts when he coughed violently. On the 7th day after admission, bronchoscopy was performed again, and a plastic cast was removed from the left lingual lobe bronchus. On the 9th day after admission, the patient appeared clinically healthy. Routine blood examinations were normal. Chest CT showed pneumonia in the left upper lung, emphysema had been relieved, and the left lower lung atelectasis had recovered (Figure 2d). The correct asthmatic treatment plan was given to the patient at discharge. After 2 months, chest CT showed obvious improvement in lung inflammation, and his asthma was well controlled.

Clinical findings for the 8-year-old boy reported in case 2. (a) Chest computed tomography (CT) on admission shows emphysema in the left upper lung and atelectasis in the lower lung. (b) Cast removed from the left principal bronchus and the middle lobe of the right lung. (c) Hematoxylin and eosin examination of plastic casts showed inflammatory necrotic tissue with a large number of eosinophils, mononuclear phagocytes and a small number of neutrophils. Bar = 100 µm. (d) Chest CT showed pneumonia in the left upper lung, emphysema had been relieved, and the left lower lung atelectasis recovered.
Discussion
As seen in the two PB cases reported in this article, this disease is associated with serious clinical symptoms, as well as sudden onset and rapid progression, which may lead to acute respiratory failure and even death. Therefore, PB requires a timely diagnosis and active treatment by clinicians. However, the pathogenesis and risk factors of this acute and critical disease are poorly understood. Currently, the main theory is based on the classification system presented by Seear et al. 6 They separated bronchial casts into two well-defined groups. Type 1 (inflammatory casts) consists of casts mainly composed of fibrin with a large number of infiltrated eosinophils and neutrophils and is common in bronchial asthma, atelectasis and fibrosis. Type 2 (acellular casts) consists of casts mainly composed of mucin with little or no inflammatory cell infiltration and occurs in children with congenital cyanotic heart disease. In the classification scheme proposed by Madsen et al. in 2005, the classifications were combined to integrate information from cast histology and patient history. Patients were divided first based on comorbidities and then cast histology if no underlying disease was identified. 7 Based on their previous history of asthma combined with the pathological analysis of bronchial casts, the two cases reported in this article should be classified as type 1.
The two cases in our study were infected with influenza A virus H1. The high affinity of H1 for the lower respiratory tract has been reported and suggests the existence of virulence factors responsible for host-pathogen interactions. 8 These virulence factors may include eosinophils as the accumulation and activation of eosinophils lead to cytolysis in the airway and subsequent mucus plugging. Yoshida et al. demonstrated that extracellular traps, mainly from activated eosinophils, were involved in the pathogenesis of PB caused by influenza virus infection (Flu-PB) and suggested that patients with Flu-PB might experience an excessive, specific immune response to the influenza virus. 9 Patients with asthma are at high risk of influenza virus infection and have high eosinophil counts. 10 In addition, influenza virus induces an imbalance in epithelial cells and immune cells in the airway of patients with asthma, and the inherent immune response is abnormally activated. During the early stage of virus infection, several cytokines involved in the inflammatory storm can be released, causing mucus hypersecretion and prolonging the airway hyperresponsiveness time in children with asthma. Together, these mechanisms promote the formation of PB. Thus, the risk of PB is significantly increased in children with influenza complicated with asthma.11,12
In this paper, the two cases did not receive the correct treatment for asthma. Wheezing symptoms usually occur following exposure to allergens or infection, and when wheezing and dyspnea occur together, they are initially considered to indicate an acute asthma attack. However, when oxygen therapy, wheezing control and other treatments are ineffective, the possibility of PB should be highly considered, especially when sputum bolt is removed or the patient coughs up cord-like secretions. When unilateral or bilateral lung breath sounds decrease during lung auscultation, and chest imaging shows atelectasis, emphysema, trachea blockage and manifestations similar to intratracheal foreign bodies, bronchoscopy should be actively performed. The gold standard for diagnosing this disease is the identification of bronchial casts by bronchoscopy, and the only effective treatment at present is the removal of bronchial casts.
Antiviral drugs, such as oseltamivir, improve the outcome of severe respiratory failure caused by influenza, and the delayed administration of antiviral drugs may be related to aggravation of the disease. 13 However, the onset of PB usually progresses rapidly within 24 to 48 hours. Therefore, during the peak influenza season, we recommend the early administration of antiviral drugs, especially in children with underlying diseases when influenza virus infection is highly suspected, even if the etiology is unknown.
In case 2, sputum culture analysis revealed Haemophilus influenzae, and alveolar lavage fluid culture was negative. Compared with case 1, his clinical symptoms were more serious, the range of lesions involved was more extensive, and the treatment course and recovery time were longer. Approximately half of patients with influenza will be complicated with bacterial infection, and because of the uncertainty with bacterial culture, the proportion of co-infection may be higher. Co-infection aggravates disease progression, leading to the occurrence of critical illness and increasing the risk of death. 14 Therefore, combined with experimental evidence, antibiotics should be used to treat critically ill patients with influenza when necessary.
Whether PB will develop after influenza A virus infection in children with asthma who receive adequate treatment in a controlled setting remains unknown. Some studies have shown that mucus plugs can occur not only in children with severe asthma but also in those with asthma remission, and they obstruct small or large airways. 15 This will be addressed in our future study. In addition, because both cases in our study were boys, future studies with larger sample sizes are needed to determine whether the incidence of PB in boys is higher than that in girls.
Conclusion
When children with asthma have acute progressive and difficult-to-relieve dyspnea after influenza A virus infection, clinicians should be aware of the possibility of PB and perform bronchoscopy as soon as possible to facilitate early diagnosis and treatment and improve patient prognosis.
Footnotes
Acknowledgement
We thank Dr Weiran Dong from the Department of Respirology, Children’s Hospital of Hebei Province, for participation in the care of the patients.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
According to our hospital regulations, ethics approval was not required for this case report study. Informed written consent was obtained from the parents of the patient.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.