
Abstract
Intracranial epidermoid cysts, also known as epidermal cysts, grow slowly and may be occult. When small, epidermoid cysts are usually clinically unremarkable or cause no definitive symptoms. At typical sites, they are easily found through magnetic resonance imaging, which aids evaluation before surgery. However, in rare cases, epidermoid cysts are situated in unusual locations or transformed to malignancy, and preoperative misdiagnosis is possible. Here, the case of a 58-year-old male patient who presented with weakness in the left lower limb and was diagnosed with a malignant epidermoid cyst in the right frontoparietal lobe, right lateral ventricle, is reported. Surgery was performed to remove the tumour followed by radiotherapy, and the patient was reported to be living independently after approximately 11 months of follow-up.
Keywords
Introduction
An intracranial epidermoid cyst is a congenital slow-growing benign lesion with an overall prevalence of 0.2–1.8% amongst all intracranial tumours. The cyst may manifest as a cholesteatoma pearl, 1 and originates as an abnormal ectoderm cell, with histopathological manifestations of squamous epithelium. 2 It most often occurs as a subdural or epidural abscess, with the most common location being the cerebellopontine angle, followed by the parasellar region and middle fossa base. 3 Cysts may also appear more rarely in the skull or pineal region.4,5
Epidermoid cysts grow slowly, and may show no decipherable clinical manifestation. Malignant transformation, more commonly observed in women, may be suspected only when the enlarging tumour volume causes an effect related to the constricted space. 1 The malignant transformation of intracranial epidermoid cyst into squamous cell carcinoma is extremely rare, mostly occurring after surgery, however, the mechanism of transformation remains unclear. While the overall prognosis of intracranial primary squamous cell carcinoma is very poor, early detection and treatment may prolong patient survival.
Herein, a case of malignant epidermoid cyst in the right frontoparietal lobe, right lateral ventricle, is reported. All patient details have been deidentified and the report conforms to CARE (case report) guidelines. 6 Ethics committee approval was not deemed to be required as this is a case report. The patient’s legal proxy provided written informed consent to publish the case, and the patient and his legal proxies consented to all administered treatments.
Case report
A 58-year-old male patient presented to the Emergency Department of the People’s Hospital of Leshan, China, in January 2022, with weakness in the left lower limb, which had gradually worsened during the previous month. Physical examination revealed grade IV muscle strength (Lovett scale) of the left lower extremity. A head computed tomography (CT) scan (Figure 1) revealed a mass in the right frontoparietal lobe, right lateral ventricle. The mass displayed cystic changes and calcification, and a high-density image indicated a solid mass. Bleeding inside the mass seemed likely.

Head computed tomography images from a 58-year-old male patient with lower limb weakness and a mass in the right frontoparietal lobe, right lateral ventricle, showing the solid part of the tumour (red arrows), the cystic part of the tumour (white arrows), and calcification (black arrows).
The physician in the Emergency Department arranged to transfer the patient to the Neurosurgery Department, People’s Hospital of Leshan, where neurosurgeons promptly ordered magnetic resonance imaging (MRI; Philips Achieva 1.5T SE MR system). The MRI showed an irregular tumour signal (Figure 2). The T1-weighted signal was low, and the T2-weighted and fluid-attenuated inversion recovery signals were slightly higher or high. The cystic portion was diffusion-limited, and non-uniform reinforcement was observed in the reinforcement sequence (enhanced T1-weighted).

Magnetic resonance images from a 58-year-old male patient with lower limb weakness and a mass in the right frontoparietal lobe, right lateral ventricle, showing: (a) T1-weighted images; (b) T2-weighted images; (c) fluid-attenuated inversion recovery images; (d) diffusion-weighted images; and (e) enhanced T1-weighted images.
During magnetic resonance spectroscopy (MRS) imaging, the N-acetyl-aspartate (NAA) peak was low, the choline (Cho) peak was elevated, and the NAA/Cho ratio was 2.0 (Figure 3). These results combined with oedema around the tumour led to a suspicion of high-grade glioma. Surgery was then performed with the aim of removing the tumour.
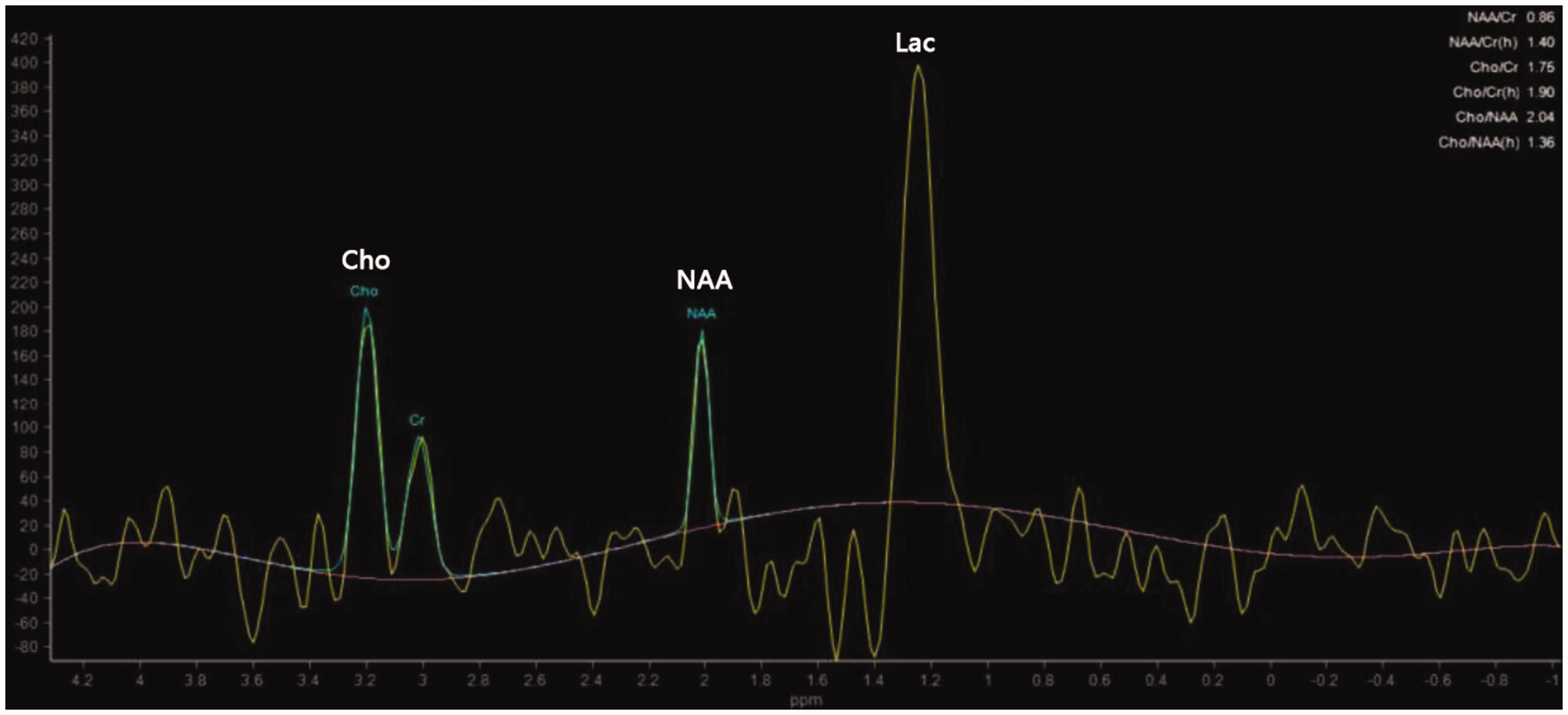
Results of magnetic resonance spectroscopy in a 58-year-old male patient with lower limb weakness and a mass in the right frontoparietal lobe, right lateral ventricle. The choline (Cho), N-acetyl-aspartate (NAA), and lactate (Lac) peaks supported a diagnosis of glioma.
During the surgery, the content of the capsule was found to be a pale yellow semi-solid slag-like substance, with no blood supply. The solid part of the tumour was grey-white and tough, with unclear boundary that was poorly differentiated from the brain tissue and rich in blood supply (Figure 4), which were features typical of epidermoid cysts. However, there were several solid masses that are not often present in general epidermoid cysts. The surgery duration was 5.5 h with approximately 200 ml of blood loss.

Intraoperative tumour images from a 58-year-old male patient with lower limb weakness and a mass in the right frontoparietal lobe, right lateral ventricle, showing: (a) capsule contents (red arrows); and (b) the solid tumour (white arrows).
Postoperative pathology confirmed that the epidermoid cyst had transformed into malignant squamous cell carcinoma (Figure 5). Refined examinations (chest and abdominal CT) were conducted to exclude the possibility of epidermoid carcinoma at other sites. Finally, with combined input from the People’s Hospital of Leshan, China and Lanzhou University Second Hospital, China, the patient was diagnosed with high-grade squamous cell carcinoma. The patient received radiotherapy (6000 cGy in 30 fractions of 200 cGy each), and no chemotherapy.

Postoperative pathology showing haematoxylin and eosin-stained tumour tissue sections from a 58-year-old male patient with lower limb weakness and a mass in the right frontoparietal lobe, right lateral ventricle, confirming malignant squamous cell carcinoma.
The tumour involved the central zone, and the left arm was found to be weaker after surgery than before surgery. Muscle strength of the left lower limb was normal. The weakness in arm strength was found to be unchanged at the 6-month and 11-month follow-up assessments. At approximately 1 year after the patient first presented at hospital, the patient was alive and living independently. The patient will continue to be followed-up in terms of survival.
Discussion
An intracranial epidermoid cyst may transform to squamous cell carcinoma, and clinical manifestations can progress rapidly. In these cases, or when an epidermoid cyst quickly recurs, carcinogenesis may be anticipated before surgery. 7 However, particularly in atypical sites, epidermoid cysts with malignant changes are rare and a correct diagnosis may be missed.
In the present case, the patient had developed left limb weakness within one month prior to hospital presentation that had gradually worsened, meeting the characteristics of malignancy. The MRS and reinforcement sequence led to a suspicion of glioma, but for the limited portion of the tumour. It was not clear whether glioma dispersion was restricted, although diffusion restriction may be present in gliomas. In the present case, the reader should note the limited diffusion of the clear cystic change zone.
Malignancy of intracranial epidermoid cyst is more common after simple epidermoid cyst surgery, with most malignant changes occurring within 5 years, 8 likely due to surgical stimulation or content overflow. 9 The cause of epidermoid cyst degeneration without a history of cranial brain surgery is unclear. There is no guide for the treatment of malignant epidermoid cyst, but the recommendation offered by the meta-analysis of Nagasawa et al. 10 favoured multimodal surgery, radiotherapy, and chemotherapy. 11 In the present case, highly differentiated squamous cell carcinoma was jointly determined by the Oncology Departments of the People’s Hospital of Leshan and Lanzhou University Second Hospital, China, and radiotherapy only was recommended, as is standard. Cases of epidermoid cysts with previous brain stem changes treated with radiotherapy have shown complete resolution by imaging. 12 The present patient has been followed for just under nearly 1 year, and a good prognosis is expected.
Conclusion
Epidermoid cyst must be considered whenever an intracranial diffusion with limited mass is encountered, even at atypical sites. A large epidermal cyst is abnormal, and combined with obvious enhancement and heavy oedema surrounding the tumour, a malignant change may be suspected. More evidence is needed to determine the optimal treatment of epidermoid cyst with malignant changes, but surgery and radiotherapy are widely applied.