
Abstract
We previously reported on two women with breast lesions in whom radiological examination could not exclude malignancy. In both cases, mastectomy was performed, and histological analyses revealed papillary lesions lined by fibrovascular stroma and nuclear inverse polarity. Hematoxylin–eosin, p63, and calponin staining indicated an absence of myoepithelial cells. However, it was concluded that the lesions had been non-malignant. These women have now been under long-term surveillance (74 months for one case and 62 months for the other) and have had no disease recurrence. Mucin (MUC)1, MUC2, MUC4, MUC5AC, MUC5B, and MUC6 immunostaining has also been performed in these women to investigate further whether their tumors were malignant or benign. In both cases, the tumors were only positive for MUC1 in apical luminal apical cells, as in normal breast tissue. MUC5B immunostaining, even when weak, can detect early breast cancer but was completely negative in our two cases. Therefore, both tumors were considered benign. Our findings in these cases suggest that nuclear inverse polarity papillary lesions lacking myoepithelial cells are benign. This knowledge should decrease the number of unnecessary operations performed for this tumor and their negative impact on patients’ quality of life.
Introduction
Breast papillary lesions show a variety of histological features, and determining whether they are benign or malignant is sometimes difficult. These lesions include benign intraductal papilloma, atypical ductal hyperplasia, and ductal carcinoma in situ.1,2
A report by Cserni in 2008 described benign apocrine papillary lesions that lacked myoepithelial cells. 3 Since then, Tramm et al. 4 and Seal et al. 5 have proposed that these lesions are benign. Tramm et al. investigated the relationship between luminal cells and myoepithelial cells in detail, 4 and their findings suggested that lack of myoepithelial cells was not always indicative of malignancy. Furthermore, Tajima et al. 6 described “non-apocrine papillary lesions”, which had typical histological features, including nuclear-inverse-polarity as well as complete lacking myoepithelial cells, and were found to be non-malignant. These lesions were subsequently defined as “nuclear inverse polarity papillary lesions lacking myoepithelial cells”. Tajima et al. also considered that a lack of myoepithelial cells was not indicative of malignancy. 6
Several studies have suggested that mucin (MUC) immunostaining status may have an important role in the diagnosis of breast tumors.6–8 The MUC immunostaining pattern is associated with both the prognosis and histological tumor-specific features and can reflect tumor behavior. Moreover, MUC immunostaining detects protein expression directly and easily and can provide more important tumor information than can other molecular biology methods.
Therefore, to clarify further the features of nuclear inverse polarity papillary lesions lacking myoepithelial cells, we performed immunostaining for MUC1, MUC2, MUC4, MUC5AC, MUC5B, and MUC6 in these two cases.
Clinical summary
Case 1
A 68-year-old woman was referred to us for further examination after a breast abnormality was detected. Ultrasonography revealed an intraductal papillary lesion measuring 2 cm. In view of the large size of the lesion, malignancy could not be excluded. Therefore, a partial mastectomy was performed. No further treatment was provided, and the patient has shown no evidence of disease recurrence during 62 months of follow-up.
Case 2
This case was a 44-year-old woman who presented after discovering a palpable breast mass. An intraductal lesion measuring 2.5 cm was detected on ultrasonography. A core needle biopsy could not rule out malignancy. Therefore, a total mastectomy was performed. After 74 months of follow-up with no further treatment, there has been no evidence of disease recurrence.
Pathological findings
Case 1
Hematoxylin–eosin-stained sections revealed epithelial papillary proliferation with inverse nuclear polarity but no nuclear atypia lined by fibrovascular stroma or myoepithelial cells. The luminal cells were round with ovoid nuclei and inconspicuous nucleoli and the myoepithelial cells were unclear. The tumor was revealed to be a well-circumscribed mass with no invasive growth pattern (Figure 1a). Tests for p63 and calponin were negative. There was weak-to-moderate positive MUC1 staining on the apical surface of the luminal cells (Figure 2a). Negative results were found for MUC5B (Figure 3a) and for MUC2, MUC4, MUC5AC, and MUC6 (not shown).
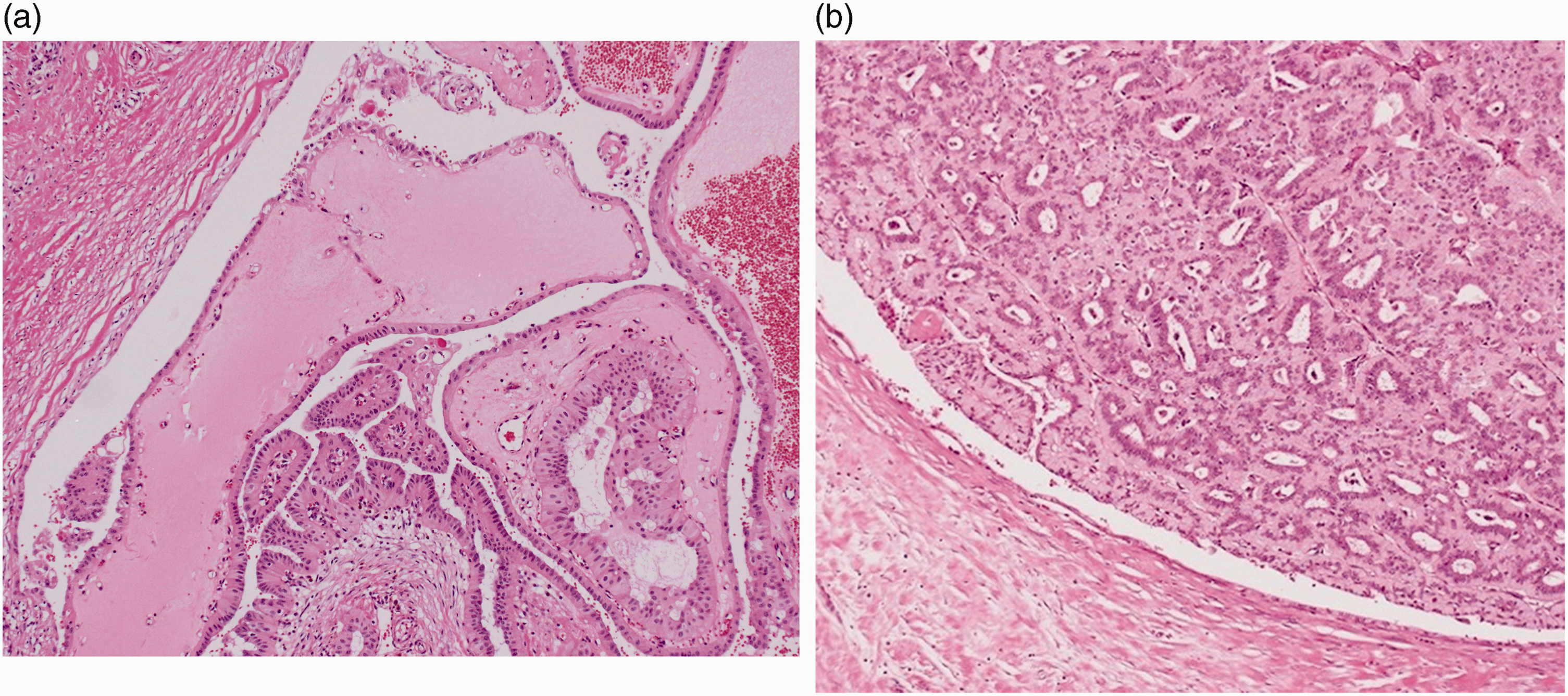
Histological findings. (a) Low-magnification view of a hematoxylin–eosin-stained specimen from case 1 showing epithelial papillary proliferation lined by fibrovascular stroma and an absence of myoepithelial cells. (Original magnification, ×40) and (b) Low-magnification view of a hematoxylin–eosin-stained specimen from case 2 reveals a papillary lesion with nuclear inverse polarity (nuclei are located on the luminal side and not the basal side) and a lack of myoepithelial cells. (Original magnification, ×40).

Immunostaining results for MUC1. (a) Immunostaining for MUC1 shows weak-to-moderate expression on the apical surface of the luminal epithelium without a stromal reaction in case 1. Allred score: PS5 + IS3 = 8 on the apical surface. (Original magnification, ×100) and (b) Immunostaining shows strong expression of MUC1 from the apical surface to the cell membrane on the luminal epithelium in case 2. Allred score: PS5 + IS3 = 8 on the apical surface. The cytoplasm shows slightly positive staining. This was thought to be an artifact because the staining pattern is non-uniform and all nuclei are negative for MUC1. (Original magnification, ×100).

Immunostaining results for MUC5B. (a) MUC5B is completely negative for case 1. Overall, these findings suggest that this lesion is benign. Annotation: nuclear inverse polarity is obvious. (Original magnification, ×100) and (b) MUC5B is also completely negative for case 2. The findings in this case suggest that this is a benign lesion. Annotation: nuclear inverse polarity is obvious. (Original magnification, ×100).
Case 2
Histological analysis revealed a papillary lesion similar to that seen in case 1 (Figure 1b). Strong positive staining for MUC1 was found from the apical surface to the cell membrane on luminal cells (Figure 2b). The results were negative for MUC5B (Figure 3b) and for MUC2, MUC4, MUC5AC, and MUC6 (not shown).
Discussion
Immunohistochemistry is used to detect the histological subtypes and features of breast tumors. Various types of epithelial cells are known to express mucins, which are a large family of glycoproteins that can be divided into two classes. One class includes MUC1, MUC3, and MUC4, which are membrane-bound mucins, and the other includes MUC2, MUC5AC, MUC5B, and MUC6, which are secreted mucins.7,9 We believe that the staining patterns for these mucins can indicate distinct histological features of these breast tumors.
In our first case of nuclear inverse-polarity papillary lesion lacking myoepithelial cells, staining for MUC-1 was moderately to strongly positive on the apical surface of luminal epithelial cells. In our second case, staining for MUC-1 was strongly positive from the apical surface to the cell membrane of luminal epithelial cells and weakly positive in the cytoplasm. Previous studies have found that MUC-1 is normally expressed on the apical surface of secretory epithelial cells.7,10 However, very strong positivity for MUC1 in not only the cell nucleus but also the cytoplasm could indicate detachment of tumor cells, invasion, and metastases and could be correlated with aggressive tumor behavior and a poor prognosis.7,11–13 In both our cases, MUC-1 staining of luminal epithelial cells was strongly positive at the apical surface but completely negative in the nuclei. Furthermore, there has been no tumor recurrence in either of these cases during at least 5 years of follow-up with no further treatment.
Previous reports indicate that mucinous carcinoma of the breast typically expresses MUC2 as the major secretory glycoprotein7,14 and that MUC2 may have an important role in prevention of tumor invasion.7,15 However, the results for MUC2 were completely negative in both our cases, suggesting no relationship with mucinous carcinoma and that the tumors were benign.
MUC5AC is found in the mucosal layer of the stomach and MUC6 in the pyloric glands.7,16,17 MUC5AC is not observed in normal breast tissue,7,18 and staining for this mucin was completely negative in both our cases. However, MUC6 expression is typically observed in mucinous carcinoma, and there have been reports suggesting that the presence of MUC-6 is indicative of a barrier to tumor invasion.7,19 Staining for MUC6 was negative in both our cases, indicating that the lesions were not mucinous carcinoma and more likely benign.
Epithelial cells in the breast have a protective layer of mucous that is provided by MUC4. The use of MUC-4 expression as an anti-adhesive and anti-recognition barrier could be a mechanism via which apoptosis is prevented and an indirect cause of increased tumor proliferation.7,20 Furthermore, MUC4 has been reported to be an important modulator of human epidermal growth factor receptor 2 (HER2).7,20,21 Our finding that MUC4 was negative in both our patients indicates lack of HER2 expression and that the lesions were probably benign.
Kim et al. have found some evidence of an association of strong MUC5B expression with aggressive tumor behavior and a poor prognosis in patients with breast cancer 22 and reported that weak staining for MUC5B is useful for detecting early breast cancer. MUC5B staining was completely negative in our two patients, which again suggests that the lesions were benign.
The pathological information gleaned in these two cases suggests that knowledge of MUC-mucins immunostaining status may reduce the number of unnecessary operations performed for breast cancer and their negative impact on patients’ quality of life. This research also provides a bridge between basic science and clinical medicine.
Conclusion
In both our cases, MUC immunostaining status and a long event-free duration of follow-up indicate that their breast lesions were benign despite a complete absence of myoepithelial cells. The term “nuclear inverse-polarity papillary lesion lacking myoepithelial cells” is long and cumbersome. Moreover, this type of breast lesion has been found to be extremely rare with a distinctive histology and unknown tumorigenesis. Therefore, we believe that this tumor should be given a shorter and more definitive name. We suggest that, in the future this lesion should be referred to as “Tajima’s tumor” in recognition of the original investigative work by Dr Shinya Tajima, who led the research group that provided the first detailed report on these tumors.
Footnotes
Acknowledgements
The authors are grateful to Junki Koike MD, PhD, St. Marianna University, for his helpful advice regarding this research. They also thank the laboratory technicians at National Hospital Organization Shizuoka, particularly Mr. Kouji Watanabe, Mr. Takashi Terai, and Mr. Masahiro Maeda for their technical assistance with this research.
Author contributions
Shinya Tajima was the main investigator in this research. Yoshio Aida and Akio Kazama contributed to providing the specimens and editing of the article. Keiko Kishimoto and Ichiro Maeda contributed to editing and revision of the article. Masayuki Takagi helped to supervise the writing of the article. All authors approved this manuscript for submission.
Declaration of conflicting interests
The authors declare no conflict of interest with respect to the research, authorship, or publication of this report.
Ethics statement
Patients are informed when they attend our institution that their case may be used for research purposes, and verbal consent is obtained at that time. Therefore, ethical approval to conduct this research and informed consent for publication was not required.
Funding
Authors received no financial support for this research, authorship, or publication of this article.