
Abstract
Objective
To evaluate the efficacy and safety of low-dose prourokinase (pro-UK) administration during primary percutaneous coronary intervention (PCI) for the treatment of acute ST-segment elevation myocardial infarction (STEMI) in patients with a high thrombus burden.
Methods
A prospective, randomized controlled trial was conducted at the Inner Mongolia People’s Hospital, China. Patients with STEMI and a high thrombus burden who underwent thrombus aspiration and primary PCI were randomly allocated to pro-UK administration or control groups. The primary endpoint was corrected thrombolysis in myocardial infarction (TIMI) frame count (CTFC).
Results
There were no significant differences in the baseline demographics or clinical characteristics of the two groups. The CTFC, tissue myocardial perfusion grade, ST-segment resolution, and myocardial blush grade of the pro-UK group were significantly better than those of the control group. In addition, after 30 days of follow-up, the pro-UK group had better cardiac function and perfusion than the control group. There were no differences in the clinical outcomes or incidence of hemorrhage.
Conclusions
Intracoronary low-dose pro-UK improves myocardial perfusion and cardiac function in patients with a high thrombus burden. Major hemorrhages still occur in patients administered pro-UK, but are no more frequent.
Keywords
Introduction
Ischemic heart disease secondary to atherosclerosis is the leading cause of global mortality 1 , having been responsible for 9.14 million deaths in 2019. 2 Rupture of coronary atherosclerotic plaques and the initiation of thrombosis result in acute myocardial infarction, of which acute ST-segment elevation myocardial infarction (STEMI) is the most life-threatening subtype. 3 Stevens et al. predicted that the annual number of cases of acute myocardial infarction may increase by 75 million as the prevalence of cardiovascular risk factors and the age of the population increase in China between 2016 and 2030. 4 STEMI accounts for more than 80% of the cases of acute myocardial infarction in China. 5
Primary percutaneous coronary intervention (PCI) is the preferred treatment strategy for patients with STEMI. 6 However, distal embolization caused by thrombus and plaque debris following PCI can impair myocardial perfusion and increase the incidences of mortality and major adverse cardiac events (MACEs), 7 especially in patients with a high thrombus burden. 8 Thrombus aspiration involves the direct extraction of the thrombus and plaque debris and has been proven to be an effective strategy to improve myocardial and epicardial perfusion. 8 In addition, intracoronary thrombolysis involves the dissolution of the residual thrombus and micro-emboli in microvessels, and promising results have been demonstrated in patients with STEMI during primary PCI.9,10 However, in those with a high thrombus burden, thrombus aspiration 11 or drug therapy alone 12 is less effective than a combination of the two.
Prourokinase (pro-UK) is a member of a new generation of thrombolytic drugs. It is a natural fibrin-specific plasminogen activator that selectively activates the binding of plasminogen to fibrin in thrombi, while having less of an effect on systemic fibrinolytic activity, thereby reducing the risk of hemorrhage. Therefore, pro-UK is expected to be an appropriate therapy for patients with STEMI and high thrombus burden. Previous studies have shown that a dose of 10 to 20 mg improves myocardial perfusion, 13 but the efficacy of low-dose pro-UK in patients with STEMI and a high thrombus burden is uncertain because of a lack of clinical evidence. Therefore, we designed a trial to evaluate the clinical efficacy of low-dose pro-UK in patients with STEMI and a high thrombus burden.
Methods
Trial design and participants
We performed a prospective, randomized controlled trial at the Inner Mongolia Autonomous People’s Hospital, China. We enrolled patients with STEMI and a high thrombus burden who were undergoing thrombus aspiration during primary PCI. The participants were randomly assigned to be administered either pro-UK or 0.9% sodium chloride at a 1:1 ratio. The inclusion criteria were as follows: age 18 to 80 years; onset of chest pain symptoms within 12 hours; electrocardiography (ECG) showing ST-segment elevation on two or more adjacent leads; and modified thrombolysis in myocardial infarction (TIMI) thrombus grades 4 (presence of well-defined thrombus, linear dimension ≥2 vessel diameters) or 5 (thrombosis leading to complete occlusion of a blood vessel). The exclusion criteria were: age >80 years or <18 years; urgent requirement for coronary artery bypass grafting; cardiogenic shock; presence of contraindications to pro-UK, aspirin, clopidogrel, or ticagrelor treatment; pregnancy; severe liver or renal failure; and inability to provide informed consent.
Written informed consent was obtained from all the participants. The study protocol was approved by the Ethics Committee for Clinical Investigations of the People’s Hospital of the Inner Mongolia Autonomous Region (No. BS201511) in July 2015. The study is registered with the Chinese Clinical Trial Registry (ChiCTR1900022290) and the reporting of the study conforms to the CONSORT guidelines. 14
Interventions
All the participants were administered aspirin 300 mg, clopidogrel 300 mg, or ticagrelor 180 mg orally prior to coronary angiography. Those who met the eligibility criteria were randomly assigned to take pro-UK or 0.9% sodium chloride. The right radial artery or right femoral artery approaches were typically used for the procedure. The thrombus in the target vessel was aspirated using a thrombus aspiration catheter following angiography in all the participants. After thrombus aspiration, the experimental group was administered pro-UK (10 mg dissolved in 10 mL 0.9% sodium chloride solution) through the thrombus aspiration catheter at the target site, and the control group was slowly administered 10 mL of 0.9% sodium chloride solution over 5 minutes, then PCI was performed. The necessity for stent placement or additional balloon dilatation was determined by the operator.
During PCI, nitroglycerin (200 μg) or sodium nitroprusside (100 μg) was administered. The standard therapy following PCI included aspirin, clopidogrel, or ticagrelor, in accordance with contemporary practice guidelines. 6
Endpoints
The primary endpoint was postprocedural CTFC, which was determined by two experienced senior interventional physicians. The secondary endpoints were tissue myocardial perfusion grade (TMPG); myocardial blush grade (MBG); ST-segment resolution (STR) after 2 hours; perfusion descending areas (PDAs); measures of heart function, including left ventricular ejection fraction (LVEF), ejection fraction on single-photon emission computed tomography (SPECT-EF), and the brain natriuretic peptide (BNP)/N-terminal-proBNP concentrations 30 days following PCI. The safety endpoint was the incidence of major adverse cardiac events (MACEs), including cardiac mortality, non-fatal myocardial reinfarction, and target vessel revascularization (TVR) and hemorrhagic events 30 days following PCI.
TIMI flow grade has been defined previously.15,16 CTFC was determined according to the method described by Gibson et al. 17 TMPG, reflecting myocardial perfusion, was defined in the report by Gibson et al. 18 LVEF, SPECT-EF, and the N-terminal-proBNP concentration were used to evaluate cardiac function and prognosis. LVEF was assessed using echocardiography, and SPECT-EF and PAD were assessed using single-photon emission computed tomography. Twelve-lead ECG was used to assess the level of STR 2 hours following PCI, and a ≥70% decrease in the total ST-segment elevation was defined as complete STR.
Randomization
We used simple randomized group allocation in the present study. The participants were randomly assigned to the groups by a statistician and envelopes were randomly assigned to the study site. Sequences were generated by computer and were concealed from the participants and clinical staff until the assignment. The participants, imaging staff, and specialists responsible for the assessment of adverse events during follow up were blinded to the grouping.
Statistics
SPSS v.24.0 (IBM, Inc., Armonk, NY, USA) was used for statistical analysis. Continuous data are expressed as mean ± SD and the two groups were compared using the independent samples t-test. Categorical data are summarized as frequencies/percentages and were compared using the chi-square test or Fisher’s exact test. The Mann–Whitney U test was used for ranked data. P < 0.05 was regarded as indicating statistical significance.
Results
Patient characteristics
A total of 1453 patients were diagnosed with STEMI during the period July 2015 to June 2018, 390 of whom met the eligibility criteria and were randomized to the pro-UK and control groups at a 1:1 ratio. Totals of 190 (97.4%) and 188 (96.4%) participants in the pro-UK and control groups, respectively, completed the 30-day follow-up period (Figure 1). There were no significant differences in the demographic characteristics of the two groups. The prevalences of participant-reported histories of hypertension, diabetes, dyslipidemia, smoking, and previous MI were comparable for the two groups. There were also no significant differences in the Killip class, culprit vessels, LVEF, TIMI flow grade, or TIMI thrombus grade (Table 1).
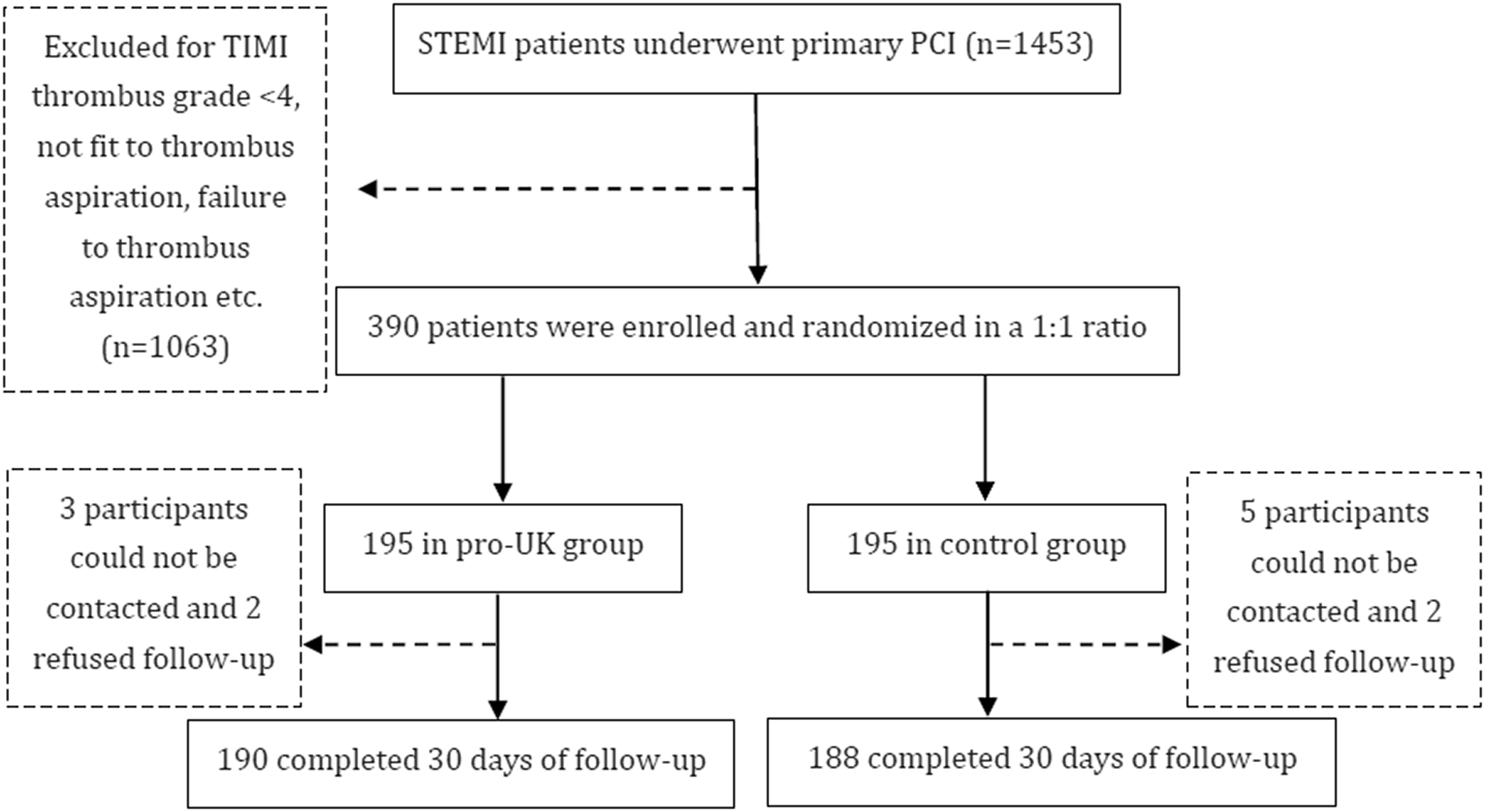
Flow diagram of the study.
Basic characteristics of the participants.
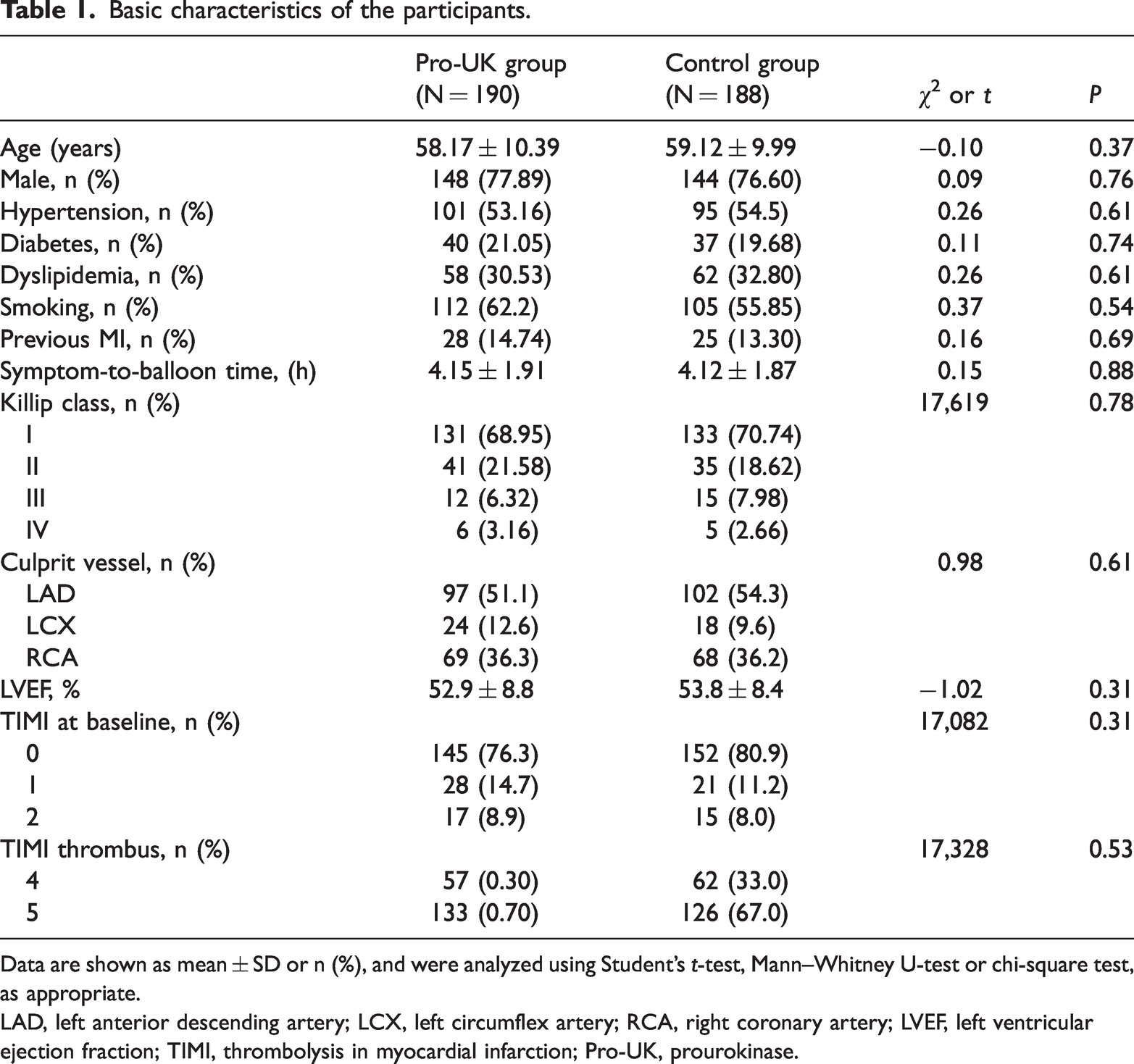
Data are shown as mean ± SD or n (%), and were analyzed using Student’s t-test, Mann–Whitney U-test or chi-square test, as appropriate.
LAD, left anterior descending artery; LCX, left circumflex artery; RCA, right coronary artery; LVEF, left ventricular ejection fraction; TIMI, thrombolysis in myocardial infarction; Pro-UK, prourokinase.
Myocardial reperfusion following PCI
The TIMI, CTFC, TMPG, and MBG, which are indices of the perfusion of the myocardium, were better in the pro-UK group than in the control group (P = 0.01, P < 0.01, P = 0.03, and P < 0.01, respectively). Participants in the pro-UK group had a higher prevalence of complete STR than those in the control group (71.05% vs. 59.04%, P = 0.01). As shown in Table 2, the concentrations of biochemical indices, including creatine kinase-myoglobin binding (CK-MB) and troponin 1 (Tn1), were lower in the pro-UK group than in the control group.
Myocardial reperfusion and indices of infarct size.

Data are shown as mean ± SD or n (%), and were analyzed using Student’s t-test, Mann–Whitney U-test or chi-square test, as appropriate.
TIMI, thrombolysis in myocardial infarction; CTFC, corrected thrombolysis in myocardial infarction frame count; TMPG, tissue myocardial perfusion grade; MBG, myocardial blush grade; CK-MB, creatine kinase-myoglobin binding; Tn1, troponin 1; Pro-UK, prourokinase.
Cardiac function
Both echocardiography (60.45 ± 5.28 vs. 57.00 ± 7.38, P < 0.01) and single-photon emission computed tomography (56.62 ± 4.35 vs. 51.27 ± 6.44, P < 0.01) showed that the pro-UK group had a higher LVEF. Participants in the pro-UK group also had a lower SPECT-PDA (12.35 ± 7.39 vs. 16.63 ± 4.46, P < 0.01) and a lower N-terminal-proBNP concentration (452.3 ± 259.4 vs. 632.7 ± 278.3, P < 0.01). The detailed results are shown in Table 3.
Cardiac function after 30 days of follow-up.

Data are shown as mean ± SD and were analyzed using Student’s t-test.
LVEF, left ventricular ejection fraction; SPECT-EF, single-photon emission computed tomography-ejection fraction; SPECT-PDA, single-photon emission computed tomography-perfusion descending area; NT-proBNP, N-terminal brain natriuretic peptide; Pro-UK, prourokinase.
Safety endpoints
As shown in Table 4, the incidence of MACE was comparable between the two groups (7.89% vs. 10.64). In addition, there were no significant differences in the incidences of components of MACE, including cardiac mortality (2.63% vs. 1.06%), non-fatal myocardial infarction (3.68% vs. 5.85%, P = 0.32), and urgent TVR (2.11% vs. 2.13%).
Endpoints after 30 days of follow-up.
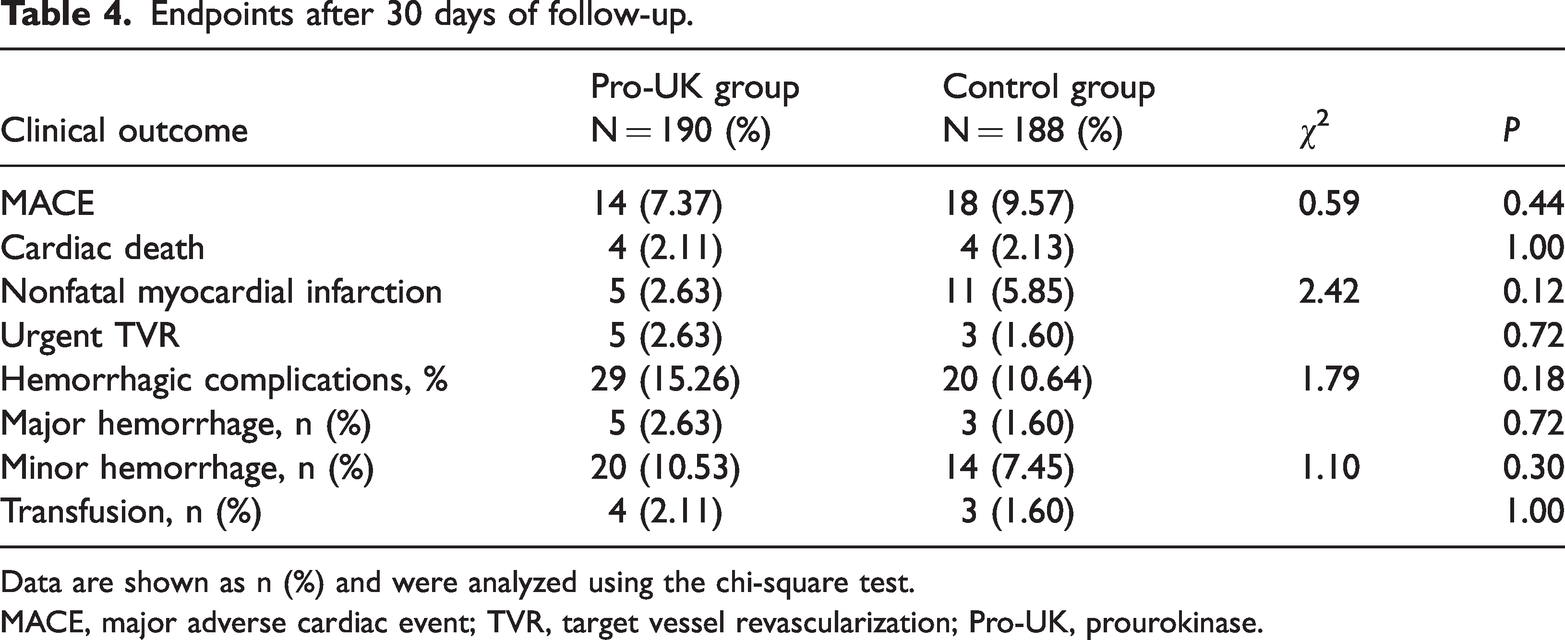
Data are shown as n (%) and were analyzed using the chi-square test.
MACE, major adverse cardiac event; TVR, target vessel revascularization; Pro-UK, prourokinase.
Discussion
Immediate reopening of the infarct-related artery (IRA) to prevent ischemic myocardium is the key aim of STEMI treatment. Previous studies have demonstrated that 30% to 50% of patients with STEMI fail to achieve effective myocardial reperfusion following PCI,19,20 which results in poorer clinical outcomes. 21 In particular, in patients with a high thrombus burden, multiple thrombosis and the downstream movement of severe thrombi contribute to the risk of distal embolization and lead to a deterioration of myocardial perfusion. Intracoronary thrombus aspiration is a commonly used treatment for a high thrombus burden; however, the resulting thrombus fragments and other micro-debris inevitably have effects on the myocardial microcirculation and perfusion.
Intracoronary administration has emerged as a useful alternative to mechanical aspiration, with potential for use in patients with STEMI and a high thrombus burden.13,21,22 Thrombolytic drugs now exist in three generations, which differ in their thrombolytic mechanisms. However, their thrombolytic effects and the incidences of associated complications are not ideal. Pro-UK is a member of a new generation of thrombolytic drugs that have intrinsic enzymatic activity. It is not readily activated and cannot activate plasminogen in the absence of thrombus, whereas plasminogen is converted to a fibrinolytic protein when it encounters a thrombus. Thus, pro-UK is converted to UK, which is a specific activator of free or bound plasminogen surrounding the thrombus and improves the efficiency of thrombolysis. 23 However, the thrombolytic effect of pro-UK is limited to the area surrounding the thrombus because pro-UK principally has its thrombolytic effect by activating plasminogen, which combines with the fibrinogen fragment Y/E. In vascular emboli, the concentration of the fragment Y/E is high, which renders thrombolysis by pro-UK specific. This facilitates the avoidance of serious adverse reactions, such as systemic hemorrhage caused by the activation of plasminogen in the blood during thrombolysis. 24 Wang et al. 25 previously evaluated the safety and efficacy of intracoronary pro-UK administration in patients with a high thrombus burden, but in the present study, we administered a lower dose (10 mg vs. 20 mg) and the thrombus burden was higher (grade ≥4 vs. grade ≥3). Geng et al. 21 also evaluated the efficacy and safety of the low-dose intracoronary administration of pro-UK during PCI in patients with STEMI, but they did not aspirate thrombus prior to the intracoronary administration. Thus, there is still a lack of clinical evidence regarding the efficacy and safety of low-dose intracoronary pro-UK administration following thrombus aspiration in patients with STEMI and a high thrombus burden.
The efficacy of pro-UK administration was evaluated by assessing myocardial perfusion and cardiac function. CTFC and the prevalence of complete STR were evaluated as indices of myocardial perfusion. We found that the pro-UK group had a better CTFC and higher prevalence of complete STR 2 hours following PCI, which is consistent with the results of previous studies.9,26 Compared with the prevalences of IRA opening associated with the administration of UK, 27 streptokinase, 28 or tissue-type plasminogen activator, 29 that associated with the administration of pro-UK was >70%, which was higher than that of the control group. The higher prevalence of complete STR associated with pro-UK administration implies than this treatment improves myocardial reperfusion. In addition, TMPG and MBG were used to evaluate myocardial perfusion, and superior results with respect to both of these indices were identified in the pro-UK group.
The peak CK-MB and Tn1 concentrations were used as indices of infarct size, and we found lower peak CK-MB and Tn1 concentrations following PCI in the pro-UK group. These results are consistent with those of Wang et al. 21 and demonstrate that pro-UK reduces infarct size. In addition, the prevalence of complete STR and the activities of cardiac enzymes indicated high levels of IRA opening and myocardial salvage associated with the administration of pro-UK. After 30 days of follow-up, we found that the pro-UK group had better cardiac function, indicated by the LVEF, left ventricular end-diastolic diameter, SPECT-PDA, and N-terminal-proBNP of the participants. The incidences of MACEs and hemorrhagic complications were low and comparable between the two groups. The characteristics (including the prevalences of diabetes, hypertension, and hyperlipidemia) of patients with a high thrombus burden have previously been shown to differ from those of patients with a low thrombus burden. 30 Therefore, the hemorrhagic outcomes of patients with a high thrombus burden might be expected to be worse than those of patients with a low burden. However, the incidences of hemorrhagic outcomes in the present study were comparable to that previously reported for patients with STEMI, 31 although the incidence tended to be higher in the pro-UK group than in the control group. Thus, the present results imply that the intracoronary administration of pro-UK during primary PCI for the treatment of patients with STEMI and a high thrombus burden improves their myocardial reperfusion and cardiac function without increasing the risk of MACEs.
Previous studies have shown that the administration of 10 to 20 mg pro-UK promotes thrombolysis and improves myocardial perfusion,13,21 and most of these involved a 20-mg dose. However, we used a dose of 10 mg in the present study, and found that this was effective, and so 10 mg may be recommended as an appropriate dose. In addition to the dose, the timing and location of intracoronary pro-UK administration remains controversial 31 and merit further research. Klaudel et al. 32 have demonstrated good performance of neurointerventional aspiration catheters in patients with acute myocardial infarction and a high thrombus burden, but this is still an off-label procedure with respect to coronary aspiration. Thus, more evidence is needed regarding the use of neurointerventional aspiration catheters. Finally, Lesiak et al. 33 reported that different forms of dual antiplatelet therapy (DAPT) may have different effects in patients following PCI. However, we did not study the influence of DAPT on outcomes in the present study. The type, timing, and dose of DAPT drugs are also worthy of study.
There were some limitations to the present study. First, the follow-up period was short; therefore, only the short-term safety and efficacy of the drug could be assessed, and longer-term follow-up studies should be performed in the future. Second, all the participants in the pro-UK group were administered 10 mg pro-UK; therefore, the effects cannot be directly compared with those of other doses, and future studies should aim to identify the most effective dose. Third, we did not perform a sample size calculation, and this may have affected the statistical significance of the results. However, we set the sample size according to the existing literature and the number of outpatients attending our hospital, and in comparison with other studies, the present sample was relatively large.
In conclusion, pro-UK improves myocardial perfusion and cardiac function in patients with STEMI and a high thrombus burden. Although pro-UK administration is associated with some major hemorrhagic events, we found that they were no more common than in patients who are not administered pro-UK.
Footnotes
Acknowledgements
The authors acknowledge all of the staff of the Catheter Laboratory of the Inner Mongolia People’s Hospital, China, for their technical support.
Author Contributions
HZ was responsible for the design of the trial. MC was responsible for data analysis and writing the article. ZW was responsible for the organization of the trial. XM, ZX, JG, WZ, and SY were responsible for the recruitment of the participants and the surgical procedures.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.