
Abstract
Wernicke encephalopathy (WE) is an acute life-threatening neurological condition caused by thiamine (vitamin B1) deficiency. Patients with WE often present with a triad of symptoms consisting of ophthalmoplegia, gait ataxia, and mental confusion. If WE is not treated in a timely manner, it can lead to serious complications such as confusion, coma, or death. Although alcohol abuse is the most commonly reported cause of WE, nonalcoholic causes—although rare—do exist. Herein, we present the case of a nonalcoholic woman with medullary infarctions who presented with intractable vomiting. Her clinical state subsequently progressed to include ophthalmoplegia and gait ataxia. A diagnosis of WE was suspected based on her clinical presentation; this was confirmed by brain magnetic resonance imaging (MRI) and the finding of decreased serum thiamine levels. Brain magnetic resonance imaging demonstrated the complete resolution of abnormal hyperintensities during a follow-up visit, 6 months after treatment.
Keywords
Introduction
Wernicke’s encephalopathy (WE) is a rare neurological condition that is associated with severe thiamine deficiency. It is usually characterized by the presence of ophthalmoplegia, gait ataxia, and mental confusion. 1 The main cause of thiamine deficiency is alcohol intoxication; however, nonalcoholic causes (such as anorexia nervosa, dialysis, prolonged fasting, prolonged parenteral nutrition, or bariatric surgery) exist, although they are rare. 2 Vomiting is another possible cause of thiamine deficiency. The treatment of WE is relatively simple and effective. Nonetheless, if WE is not treated in a timely manner, it can lead to irreversible cognitive impairment and may be fatal. A diagnosis of WE can be made based on clinical presentations, brain magnetic resonance imaging (MRI) findings, and decreased plasma thiamine levels. Notably, however, a major barrier to early diagnosis is the low index of WE suspicion in nonalcoholic patients, who may not have the complete classic triad of symptoms at presentation.
Here, we report the case of a patient with nonalcoholic WE with medullary infarctions who presented with intractable vomiting. Three weeks later, she developed double vision and blurred peripheral vision, and was subsequently diagnosed with WE.
Case presentation
A woman in her 50s with a past medical history of hypertension was admitted to hospital because of dizziness and vomiting. She was diagnosed with medullary infarctions. After receiving standardized antiplatelet and lipid-lowering therapies, her dizziness was relieved but her vomiting did not resolve. Three weeks later, she developed double vision and blurred peripheral vision, and was subsequently transferred to our hospital. Upon arrival, a physical examination revealed restricted abduction in both eyes, multidirectional horizontal and vertical nystagmus, and finger-to-nose ataxia. These findings did not correlate with her medullary infarction symptoms.
Subsequently, fluid-attenuated inversion recovery magnetic resonance imaging (MRI) of the brain was performed. This revealed symmetrical hyperintense signals within the bilateral walls of the third ventricle and mammillary bodies (Figure 1). Moreover, brain MRI revealed medullary infarctions on T2-weighted images (Figure 2). Magnetic resonance angiography demonstrated no occlusive lesions in the major intracranial cerebral artery (Figure 3). Laboratory test results, including of sodium, glucose, creatinine, lipase, amylase, and blood coagulation parameters, were within normal ranges. The patient was negative for antibodies against GQ1b ganglioside. However, her thiamine level was significantly low, at 49 nmol/L (reference range: 70–220 nmol/L). The patient had no history of alcohol abuse.
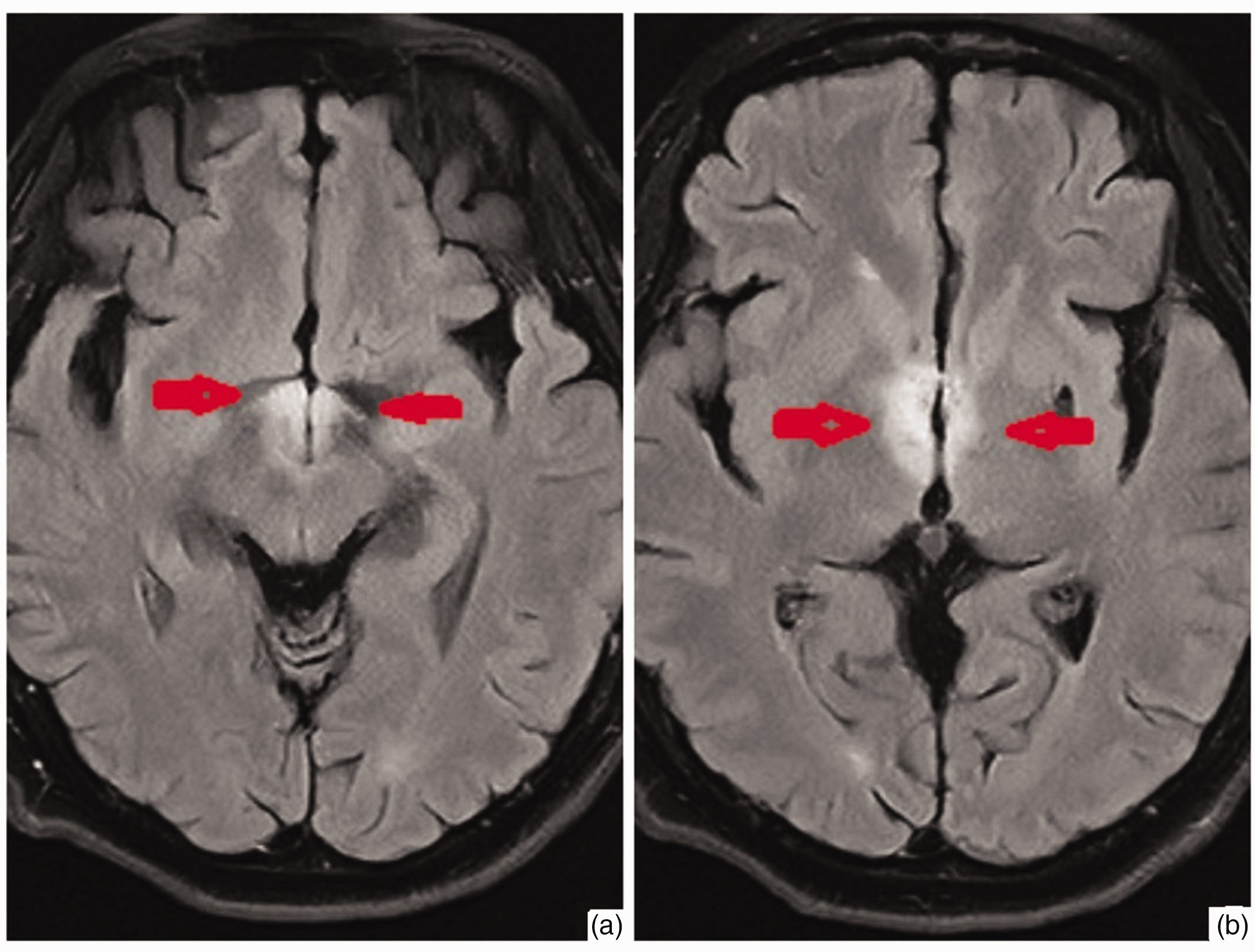
Brain magnetic resonance imaging showing hyperintense signals within the mammillary bodies (a) and the bilateral walls of the third ventricle and (b) on fluid-attenuated inversion recovery.

Brain magnetic resonance imaging showing medullary infarctions on T2-weighted images.

Brain magnetic resonance angiography showing no occlusive lesions in the major intracranial cerebral artery.
We diagnosed nonalcoholic WE and started immediate intravenous (IV) thiamine replacement therapy. The patient’s condition was managed with 40 mg IV pantoprazole daily as well as 4 mg IV ondansetron every 6 hours as needed for vomiting. An IV thiamine supplementation of 500 mg was administered thrice daily (TID) for 3 days, after which the IV dose was reduced to 250 mg TID for 3 days. The thiamine supplement was changed to an oral formulation at a dose of 100 mg TID for 2 weeks. The patient’s vomiting resolved, her symptoms of double vision and ataxia improved, and she was subsequently discharged. The oral thiamine supplement dose was changed to 100 mg daily for 6 to 8 weeks after discharge.
During the follow-up visit, 6 months later, the patient was noted to have normal neurological examination findings. Another MRI scan of the brain was performed, and the previously observed hyperintense signals within the bilateral walls of the third ventricle and mammillary bodies had disappeared (Figure 4).

Brain magnetic resonance imaging showing the disappearance of hyperintense signals within the mammillary bodies (a) and the bilateral walls of the third ventricle (b).
The reporting of this case conforms to the CARE guidelines (for CAse REports). 3
Discussion
WE was first reported in 1881 by Carl Wernicke, who noted a clinical symptom triad of ophthalmoplegia, gait ataxia, and mental confusion. However, fewer than 30% of all patients have this classic presentation. 4 Although nystagmus and ophthalmoplegia are very common, ataxia is present in 23% to 25% of patients, and mental confusion occurs in 34% to 82% of patients. 5 It is therefore very difficult to diagnose WE.
WE is an acute neurological disorder that is caused by thiamine deficiency. Despite being traditionally associated with chronic alcoholism, multiple nonalcoholic etiologies of WE have been encountered in the clinic, such as nutritional imbalance, anorexia nervosa, prolonged IV feeding, hyperemesis, and malabsorption syndrome. In patients with nonalcoholic WE, the diagnosis of thiamine deficiency is often delayed.
Vomiting can be both a cause and a consequence of thiamine deficiency. 6 Furthermore, vomiting is a strong predictor of nonalcoholic WE in adults. 7 Thiamine is an essential vitamin and cofactor in numerous metabolic pathways, such as for the oxidative degradation of carbohydrates, fatty acids, and amino acids and for the production of adenosine triphosphate. 8 Thiamine triphosphate acts as a neurotransmitter. Without thiamine, pyruvate can be converted to lactic acid; however, lactic acid is unable to enter the tricarboxylic acid cycle, which can lead to lactic acid accumulation and cell death.
Here, we reported a patient with nonalcoholic WE with medullary infarctions. The patient presented with vomiting, and head MRI revealed lesions in the area postrema. Three weeks later, she developed double vision and blurred peripheral vision, and was subsequently diagnosed with WE. Nonetheless, she did not experience mental confusion throughout the course of the disease.
In brain MRI, thiamine deficiency-induced abnormalities can be visualized as hyperintense signals in the periventricular regions of the thalamus, hypothalamus, mammillary bodies, periaqueductal region, fourth ventricle, or midline cerebellum on both T2 and fluid-attenuated inversion recovery sequences. 9 These abnormalities are observed because these regions require more adenosine triphosphate for energy and to protect cells from reactive oxygen species damage, so that cells can maintain tissue integrity and function. Brain MRI may be used to support the clinical diagnosis of WE because it has a high specificity (93%); however, it has relatively poor sensitivity (53%) for WE diagnosis. 10 Furthermore, the abnormal hyperintensities in brain MRI can reverse. In our patient, MRI revealed symmetrical hyperintense signals within the bilateral walls of the third ventricle and mammillary bodies, thus confirming the diagnosis of WE. By 6 months after standard treatment, however, the abnormal brain MRI signals had disappeared.
One possible differential diagnosis for our patient was Miller–Fisher syndrome, which is associated with upper respiratory tract infections and manifests as ophthalmoplegia, ataxia, and areflexia. 11 However, our patient was negative for antibodies against GQ1b ganglioside, and her marked improvement in symptoms after thiamine treatment further ruled out this diagnosis. Another differential diagnosis was central pontine myelinolysis, which is mainly observed in alcoholic patients; symptoms include oculomotor nerve palsy, dysphagia, altered tendon reflexes, dysarthria, weakness in the extremities, and confusion. 12 Nevertheless, this diagnosis was excluded because our patient had normal plasma sodium concentrations.
Another differential diagnosis for WE includes Bickerstaff brainstem encephalitis, which occurs after a previous infection (mainly respiratory or gastroenteric). After apparent remission, affected individuals begin to exhibit the main features of the syndrome: loss of consciousness, ophthalmoplegia, and ataxia. The standard treatment for Bickerstaff brainstem encephalitis involves IV immunoglobulin or steroids, which is very different from that of WE (i.e., IV thiamine). 13 Once WE is diagnosed or suspected, it is therefore critical to immediately begin thiamine replacement therapy to avoid progression. 14 The prompt IV administration of thiamine can alleviate neurological symptoms, cognitive dysfunction, and brain imaging lesions associated with WE. 15 In the present case, our patient received IV thiamine followed by oral thiamine, which led to substantial improvements in visual acuity and ataxia.
Conclusions
WE is a medical emergency that is underrecognized, especially in nonalcoholic patients. The present case highlights the critical importance of the timely recognition and treatment of WE. The diagnosis of WE in our patient in the absence of the classic triad of symptoms underscores the need for a thorough clinical history and imaging, particularly in patients with vomiting. This case report will therefore contribute to increasing awareness among clinical physicians in terms of the potential risks and complications associated with thiamine deficiency.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241274570 - Supplemental material for Wernicke encephalopathy in a patient with medullary infarctions: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605241274570 for Wernicke encephalopathy in a patient with medullary infarctions: a case report by Lu Wang, Guan-jie Song and Hong-jun Su in Journal of International Medical Research
Footnotes
Author contributions
Lu Wang wrote the manuscript, Hong-jun Su performed the data analysis, and Guan-jie Song performed the formal analysis and validation.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Ethics statement
This study was approved by the Ethics Committee of Tianjin Baodi Hospital (approval number lunli2498). The patient provided their written informed consent for the dissemination of the findings for educational and research purposes.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.