
Abstract
We describe a technique for metallic intralenticular foreign body (ILFB) removal in a patient in whom there was no or minimal cataract formation or other complications. This technique required creating two corneal small incisions around the ILFB for inserting iris retractors to expose the ILFB. At the foreign body position, a clear corneal incision was made, and then the ILFB was removed with minimal manipulation by an intraocular magnet without complications. Because most occupational traumas occur in young people, this technique avoids the adverse outcomes of lens extraction in this age group.
Introduction
Intralenticular foreign bodies (ILFBs) account for approximately 10% of intraocular foreign bodies. 1 Different types of ILFBs, such as metallic objects, vegetable materials, cilia, glass, stone, and coal, have been reported. 2 The appropriate management option for ILFBs is usually selected on the basis of the patient’s characteristics, type of foreign body, its complications, and physicians’ preferences. 2 The main management options for these bodies include conservative management and observation, or surgical foreign body removal with phacoemulsification or extracapsular cataract extraction. 1 Metallic iron foreign bodies can cause siderosis, and in cases in which conservative management is chosen, regular follow-up including an electroretinogram should be performed. Foreign bodies should be removed if any sign of siderosis is detected. 1 The main indication for performing surgery is siderosis. 3 The most popular surgery in recent years is phacoemulsification with intraocular lens implantation if there is no major posterior injury. 3 However, most occupational ocular traumas occur in young patients, and lens removal in this age group is not without adverse effects. The loss of active accommodation, especially in children, and retinal detachment are among the major concerns. 4
We describe a technique of metallic ILFB removal using an intraocular magnet technique through an anterior lens capsule defect. The crystalline lens remained clear in this method during our 2-year follow-up.
Case report
A 27-year-old man presented to our ophthalmic emergency room with the chief complaint of redness and a burning sensation in his left eye after hammering a metallic object. His past medical history was unremarkable. On examination, his uncorrected visual acuity (UCVA) was 20/20 in both eyes. Intraocular pressure of the right and left eyes was 14 and 13 mmHg, respectively. A slit lamp examination of the left eye showed a self-sealed, full-thickness, corneal wound and a round full-thickness defect in the iris at the 11 o’clock position (Figure 1a, c). The Seidel test was negative. The anterior chamber was deep and clear. After dilation, a defect in the anterior lens capsule behind the corneal and iris wounds was noted. There was no sign of lens opacity, except for a small opacity under the anterior capsule defect. A dilated fundus examination was normal. Anterior segment optical coherence tomography was useful to localize the ILFB (Figure 1b). An orbital computed tomography scan showed no other foreign body. An examination of the right eye was normal.
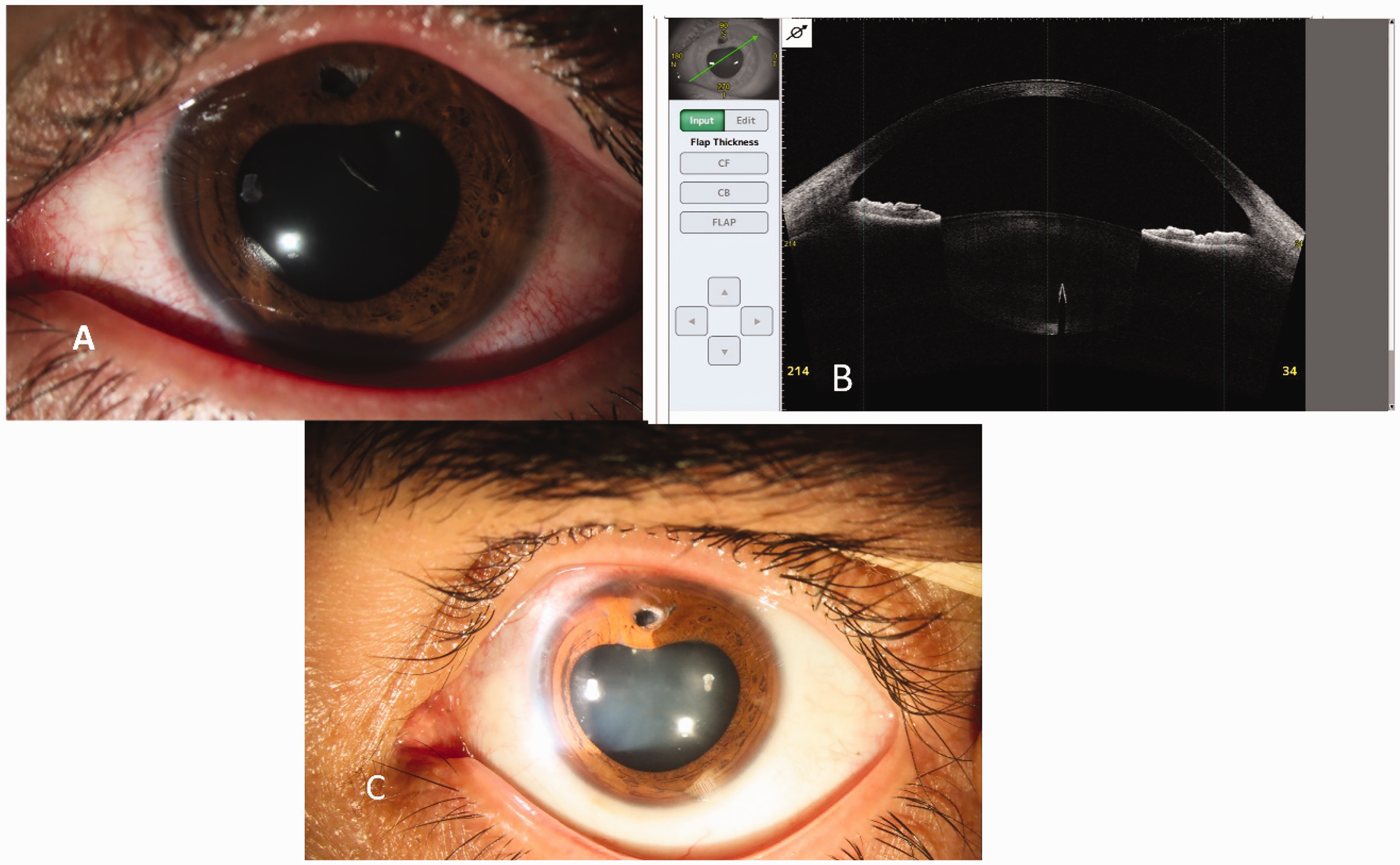
(a) Preoperative slit photograph of the intralenticular foreign body. (b) Anterior segment optical coherence tomography shows the exact position of the intralenticular foreign body and (c) Postoperative slit photograph shows the clear crystalline lens after 2 years.
On the basis of the patient’s history and examinations, an ILFB was diagnosed. Because of his 20/20 visual acuity and clear lens, he was scheduled for surgical removal of the foreign body without crystalline lens extraction. The ILFB was removed as described in the Surgical technique section below. The other parts of the crystalline lens remained clear. On postoperative day 1, the UCVA of the left eye was 20/20, and no lens opacity was observed in the visual axis. At his 2-year follow-up visit, UCVA of the left eye was still 20/20, and the lens remained clear in the visual axis. Postoperatively, the patient had no complications, and his UCVA was preserved at 20/20. The reporting of this study conforms to the CARE guidelines. 5
Surgical technique
Under topical anesthesia, two corneal small stab incisions were made at 10 and 2 o’clock (around the foreign body). Two iris retractors were then inserted, and the pupillary margin was engaged and dilated locally (Figure 2a, b). An ophthalmic viscosurgical device was injected to maintain the anterior chamber. The adhesions of the iris around the rupture site on the anterior capsule of the lens were broken with the ophthalmic viscosurgical device. A clear corneal incision was made at the position of the foreign body. Careful manipulation of the capsular flap was performed, and an intraocular magnet was then inserted (Figure 2c). The metallic ILFB was removed from the lens through the anterior capsule defect (Figure 2d). Finally, the ophthalmic viscosurgical device was removed from the anterior chamber with irrigation and aspiration (Video 1).

Surgical removal of a metallic intralenticular foreign body using an intraocular magnet without crystalline lens extraction. (a) A self-sealed, full-thickness, corneal laceration and iris hole at the 11 o’clock position of the left eye. (b) Iris retractors are placed to pull the iris away and viscoelastic is injected into the anterior chamber. (c) An intraocular magnet is inserted through the corneal incision and (d) The metallic intralenticular foreign body is removed through the defect in the anterior lens capsule.
Discussion
ILFBs have a low incidence among intraocular foreign bodies, but can cause serious complications, such as cataract formation, uveitis, glaucoma, lens subluxation, ocular siderosis, and endophthalmitis. 6 Choosing the best management option is based on many factors, such as the characteristics of foreign bodies (type and size), complications, associated ocular traumas, and the patient’s desire. 6 In cases managed by observation, follow-ups including an electroretinogram are required to identify early signs of siderosis, which necessitate the removal of foreign bodies. 1
Lin et al. reviewed 28 cases of ILFBs between 1985 and 2014. 6 All patients were managed surgically by combined foreign body removal, lens extraction (either with phacoemulsification, extracapsular cataract extraction, or lens aspiration), and intraocular lens implantation. Indications for surgery varied. Most indications were due to total or localized cataract formation. Some patients developed lens subluxation, uveitis, or glaucoma. Two patients underwent surgical lens removal because of a copper containing foreign body and an organic foreign body to avoid risks of inciting severe inflammation and infection respectively. The inability for follow-up at frequent intervals and patient’s visual demand were other mentioned reasons for surgery. Foreign bodies were removed using a magnet, forceps, and viscoelastics first or along with the whole lens. 6
The removal of ILFBs using a magnet along with lens extraction has been reported.7,8 However, in a detailed search, we found only two reports of surgical removal of ILFBs with preservation of the crystalline lens. In 2003, Luo et al. reported 15 cases of ILFBs ranging from 0.3 mm to 3 mm in diameter with a transparent lens in the Chinese literature, and they were removed by using intraocular magnets without lens extraction. 9 Follow-up for 4 years showed transparency of the lenses and stable visual acuity. However, a detailed technique was not established. Recently, Xue et al. reported a case of a 35-year-old man with an ILFB in which the patient had tried to remove the foreign body by himself using a magnet. 10 The foreign body was drawn to the lens equator. Surgery was performed, and the foreign body was removed through a capsular wound using a magnet. Most of the lens remained clear after a 3-month follow-up.
Our patient was a young man with a small metallic ILFB with no associated cataract or signs of ocular inflammation. We had access to the foreign body using iris retractors and viscoelastics, and successfully removed it by a magnet with minimum manipulation of the crystalline lens. The lens remained clear during our follow-up visits with preservation of his UCVA to 20/20.
Surgeons should consider different factors while choosing the best method of surgery in their patients. The characteristics of foreign bodies (size, site, and metallic versus nonmetallic), the presence or absence of cataract and the degree of cataract, other associated ocular complications, such as uveitis, glaucoma, and endophthalmitis, and the patient’s age and visual needs are important parameters for consideration. To the best of our knowledge, this is the first report of removal of an ILFB in a patient with no major traumatic cataract using an intraocular magnet. This is a safe method that can preserve the patient’s crystalline lens with the least trauma to ocular structures. Complications of lens extraction and intraocular lens implantation can be avoided, especially in young patients and children who have the power of accommodation. The main limitation of this technique is that it is only applicable to metallic foreign bodies with no other associated complications. Long-term studies are warranted to determine the efficacy of this technique.
Footnotes
Author contributions
FA wrote the original draft. BM reviewed and edited the manuscript. SAT reviewed the manuscript. AAH interpreted the patient data. AG created the figures. SH interpreted the patient’s data. MS reviewed and edited the manuscript and supervised the project. All authors read and approved the final manuscript.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
This study was conducted according to the World Medical Association Declaration of Helsinki. Ethics approval was not required because of the nature of this study (case report). The patient provided written consent to publish his disease process and related images.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.