
Abstract
This narrative review explored the comprehensive clinical applications of anterior segment optical coherence tomography in cases of ocular trauma and emergencies, with a focus on its diagnostic, therapeutic, and future implications. A literature search was conducted via PubMed, Scopus, and Web of Science using relevant keywords, yielding 86 articles for inclusion. However, no formal systemic review or meta-analysis was performed. These studies highlight the role of anterior segment optical coherence tomography as a high-resolution, noncontact imaging modality that enables detailed assessment of anterior segment injuries, even in cases with compromised visualization due to corneal opacity or hyphema. Anterior segment optical coherence tomography facilitates accurate diagnosis of corneal lacerations, intraocular foreign bodies, traumatic cataracts, and angle abnormalities, contributing significantly to surgical planning. Moreover, anterior segment optical coherence tomography angiography provides novel insights into anterior segment vasculature; for instance, it helps detect limbal ischemia in chemical injuries. Despite its numerous benefits, anterior segment optical coherence tomography is limited by its inability to image structures posterior to the iris and its reliance on patient cooperation for accurate imaging. Overall, anterior segment optical coherence tomography has transformed the evaluation and management of ocular emergencies by enhancing structural visualization and improving clinical decision-making. Future innovations, including enhanced penetration depth and integration of artificial intelligence, are expected to further expand its diagnostic and therapeutic potential.
Keywords
Introduction
Ocular trauma is the leading cause of preventable monocular blindness and vision impairment. 1 It may occur following a wide range of events, including sports injuries, occupational hazards, and accidental trauma. 1 Trauma causes monocular vision impairment in more than 19 million people worldwide, with some of them becoming permanently blind. 1 In the United States, 2.0–2.4 million cases of ocular trauma occur annually, with approximately 40,000 resulting in blindness or major vision impairment.1,2 Vision impairment following ocular trauma can further affect the patients’ quality of life, mental well-being, and financial security. 3 Additionally, infectious keratitis is a significant ocular disorder and a primary cause of corneal blindness globally.4,5 Infectious keratitis is the leading cause of nontrachomatous corneal opacity and accounts for approximately 3.5% of all global blindness cases.4,6–8 The prevalence of this disease decreased from 1.6 million in 1990 to 1.3 million in 2015. 9 Timely diagnosis and appropriate treatment are crucial for preventing irreversible complications in patients with ocular trauma and infectious keratitis.
Anterior segment optical coherence tomography (AS-OCT) has transformed anterior segment evaluation through its unparalleled depth and clarity in imaging. 10 This sophisticated imaging technique offers both qualitative and quantitative evaluations of the anterior segment, allowing a thorough evaluation of structures that are typically difficult or impossible to view using conventional diagnostic tools. 10
One of the key advantages of AS-OCT is its ability to perform imaging without direct contact with the eye. It can generate high-resolution cross-sectional images that minimize patient discomfort, which is particularly useful in trauma cases. 11 Other diagnostic methods such as slit-lamp examination, ultrasound biomicroscopy (UBM), gonioscopy, and specular microscopy have significant limitations. Compared with AS-OCT, UBM offers lower resolution images of the anterior segment due to its shorter wavelength, resulting in increased scatter and signal loss. 12 Moreover, it requires direct contact with the eye, which is particularly uncomfortable for trauma patients. 13 Gonioscopy and slit-lamp examinations are operator dependent and limited by corneal clarity and patient cooperation. 14 Finally, the most significant limitation of specular microscopy is its inability to fully visualize the anterior segment. 15 In contrast, AS-OCT excels in detecting subtle structural changes. 16 It is particularly useful when corneal edema, opacities, or hyphema obstruct the view, allowing clear evaluation of the underlying pathology. 16 AS-OCT has become an important instrument in the evaluation of anterior segment anomalies, overcoming the aforementioned limitations and improving diagnosis and treatment outcomes.11–18
There have been significant technological advancements in the field of AS-OCT. The earliest form of AS-OCT was time-domain OCT (TD-OCT), which used a moving reference mirror to create images. 19 Although it is currently uncommon in clinical practice due to its lower resolution and acquisition speeds, TD-OCT was the predecessor to the newer devices being used today. 19 Spectral-domain OCT (SD-OCT) replaced this moving mirror with a stationary spectrometer. This change allowed visibility of the anterior and posterior segments, with improved axial resolution and faster image acquisition. 19 The most advanced form of AS-OCT is swept-source OCT (SS-OCT). SS-OCT uses a tunable laser source that enables deeper tissue penetration due to its longer wavelength and faster scanning speeds than SD-OCT.19,20 It is particularly useful for clearly visualizing the entire anterior segment and deeper anatomic structures. 21
As a consequence of these technological advancements, AS-OCT has demonstrated diagnostic utility in various ocular conditions. However, its application in ocular emergencies, particularly ocular trauma and infectious keratitis, has not been comprehensively reviewed. This narrative review aimed to provide an overview of the diagnostic and clinical utility of AS-OCT in these cases. A literature search was conducted using the PubMed, Scopus, and Web of Science databases, with a focus on studies related to AS-OCT use in acute anterior segment pathologies. No specific quality assessment of the studies was performed.
Methods
A narrative literature review was conducted to evaluate the clinical applications of AS-OCT in ocular trauma and emergencies. No formalized reporting guideline or protocol was followed for this review. A comprehensive search was performed via the PubMed, Scopus, and Web of Science databases using a combination of keywords, including “Anterior Segment Optical Coherence Tomography,” “AS-OCT,” “ocular trauma,” “corneal laceration,” “foreign body,” “traumatic cataract,” “angle recession,” “hyphema,” “infectious keratitis,” “limbal ischemia,” “chemical burn and injury,” “posterior capsular rupture,” “extraocular muscle injury,” and “keratitis.” Studies published in English were considered, with no restrictions on publication year. After removing duplicates, H.A. and K.D. reviewed the abstracts for relevance. Full-text articles were screened for suitability based on their discussion regarding the role of AS-OCT in diagnosing and managing ocular injuries and infectious keratitis. However, given the narrative review framework, no specific quality assessment of the studies was performed. In total, 86 articles published from February 1997 to February 2025 were included. Their findings were summarized to highlight the advantages, limitations, and future directions of AS-OCT use in ocular trauma and emergency settings. The images included in the article were sourced from patients treated at Farabi Eye Hospital and used to illustrate the clinical application of AS-OCT in real-world settings.z
Results
Corneal injuries
Corneal lacerations
AS-OCT can be used as an adjunct to slit-lamp biomicroscopy in ocular trauma cases, specifically in cases of corneal lacerations, traumatic corneal edema, and corneal blood staining. 16 In post-traumatic corneal edema, AS-OCT can help diagnose traumatic Descemet membrane detachment, which may be missed using slit-lamp biomicroscopy in the presence of corneal edema.11,22 When hyphema is present, AS-OCT can show corneal blood staining. Red blood cells and their products are visible as hyperreflective areas in the posterior stroma. In addition, AS-OCT can reveal other pathological findings that occur in association with hyphema but are not visible using slit-lamp biomicroscopy, such as pupillary block and secondary angle-closure glaucoma concurrent with hyphema.11,22
In corneal lacerations, AS-OCT has been useful in distinguishing full-thickness corneal lacerations from lamellar lacerations, subsequently playing an important role in guiding treatment decisions and surgical approaches. It is also helpful in determining the healing response after the surgical repair of lacerations.23,24 Several parameters have been measured after primary repair, including the height of the steps, width of the wound gap, and maximal corneal thickness. Higher wound steps early after primary repair are associated with more severe scar formation and lower edge alignment.23,25
Epithelial ingrowth is a rare but serious complication following trauma and primary repair, often posing diagnostic challenges. AS-OCT is a valuable diagnostic tool in such cases, with a reported sensitivity of 78% and specificity of 26% in identifying hyperreflective structures indicative of epithelial invasion. 26
Chemical injuries
In cases of chemical eye burns, AS-OCT has been utilized for initial diagnosis, damage assessment, treatment response evaluation, and intervention planning. A key prognostic factor in these cases is limbal ischemia, whose clinical assessment is challenging because of its subjective nature. 27 AS-OCT angiography (AS-OCTA) enables objective and precise evaluation of limbal ischemia and its extent in acute chemical injuries.28–30 Comparisons between clinical examination and AS-OCTA have indicated that clinical assessments tend to underestimate the extent of ischemia. Additionally, AS-OCTA effectively monitors the revascularization process. 31
AS-OCT effectively visualizes structural pathologies in the cornea and anterior chamber (AC) following chemical burns, even in the presence of corneal opacity. These changes include epithelial defects, corneal edema, opacification, neovascularization, stromal disintegration, stromal cyst formation, Descemet’s membrane detachment, bulla formation, AC inflammation, anterior synechiae, and potential angle-closure glaucoma.32–34 Consequently, AS-OCT plays a crucial role in staging chemical burns, monitoring wound healing, and guiding both the initial treatment plan and the assessment of treatment success.34,35
AS-OCT provides valuable data for monitoring the response to various topical and surgical treatments for ocular burns. It is particularly useful in assessing the postoperative anatomical stability of keratoprostheses, which are occasionally used for managing advanced chemical burns. 36
Foreign bodies
Corneal foreign bodies are the second most common cause of ocular trauma after corneal epithelial defects. 37 AS-OCT is a noninvasive and effective tool for identifying, localizing, and monitoring intrastromal foreign bodies. 38 In many cases, slit-lamp examination alone cannot accurately determine the type of deep corneal foreign body; however, this information is crucial for planning its removal. AS-OCT has been used to differentiate specific materials based on their characteristics. 39 Opaque objects, such as metal, wood, and pencil graphite, appear hyperreflective at the anterior border; however, their posterior border is obscured due to shadowing. A mirroring effect, seen as an inverted chain of signals, is characteristic of metal and pencil graphite. Transparent objects display distinct hyperreflective borders when surrounded by air or fluid but appear differently when embedded in the corneal stroma. However, organic foreign bodies do not exhibit specific AS-OCT features.40,41
Determining the depth of an intrastromal foreign body can be challenging using slit-lamp biomicroscopy. If a foreign body has fully penetrated the cornea and remains undetected before removal, an extraction attempt may cause open globe injury. 42 However, AS-OCT accurately delineates the borders of an intrastromal foreign body, clearly determining whether it has reached the Descemet’s membrane and entered the AC.42–46 This makes AS-OCT a valuable tool for clinicians when deciding between surgical and outpatient management of fully embedded corneal foreign bodies.42,43,47,48 Additionally, AS-OCT can assess corneal wound depth and width following foreign body removal, 47 allowing clinicians to predict the corneal scar size.49,50
AS-OCT is also valuable in the diagnosis and management of post–laser-assisted in situ keratomileusis (LASIK) corneal foreign bodies. In these cases, careful evaluation for flap-related complications is essential. AS-OCT provides detailed visualization of both foreign body and flap characteristics, making it a crucial imaging tool in such scenarios. 51
In cases of intrascleral foreign bodies, AS-OCT has been used to detect objects concealed behind subconjunctival hemorrhage or granuloma. Although UBM remains the gold standard, AS-OCT offers a less invasive and more accessible alternative, enabling effective visualization of foreign bodies within the sclera. 52 Additionally, AS-OCT has been utilized to assess deeper structures. For instance, it is used for detecting foreign bodies within the crystalline lens in suspected patients, particularly when slit-lamp examination cannot provide accurate results due to the presence of traumatic cataract.
Traumatic cataracts
Traumatic cataract is a significant cause of vision loss following ocular trauma, with a high estimated prevalence of 65%. 53 Both blunt and penetrating traumas can lead to the development of traumatic cataracts.53–55 AS-OCT plays a crucial role in visualizing subtle anatomical and pathological lenticular changes, both preoperatively and intraoperatively.56–58 It provides an objective grading of immature cataracts and detailed imaging of intralenticular structures, the posterior capsule, and zonular integrity in various types of cataracts, including traumatic and mature cataracts.59–62
The detection of anterior lens capsule defects is a key predictor of future traumatic cataract development. However, identifying these defects using slit-lamp examination can be challenging, especially when the cornea is damaged. In such cases, AS-OCT proves to be an invaluable diagnostic tool. 11 It enables the objective assessment of lens opacity, which may directly impact vision loss, particularly in cases where corneal edema limits the effectiveness of slit-lamp biomicroscopy. Furthermore, AS-OCT allows the evaluation of the posterior capsule and zonular integrity, which is essential for aiding surgical planning, predicting intraoperative challenges, and determining the feasibility and type of intraocular lens (IOL) implantation.56,63,64 Without ancillary imaging techniques such as AS-OCT, it may not be possible to detect a posterior capsule tear behind an opacified lens (Figure 1).65,66 Nonetheless, it is noteworthy that slit-lamp examination remains a more accessible, cost-effective, and dynamic assessment tool than AS-OCT. 67

Traumatic cataract in two patients with a history of trauma and decreased vision. (a) AS-OCT showing an intact posterior capsule and (b) AS-OCT demonstrating posterior capsule rupture, indicated by the yellow arrows. AS-OCT: anterior segment optical coherence tomography.
Our previous study demonstrated that SS-OCT is a valuable tool for preoperative assessment of posterior capsule integrity in traumatic cataracts, showing superior sensitivity (96.8%) and accuracy (82%) compared with UBM. 62 Given its noncontact nature and high-resolution imaging, SS-OCT enhances surgical planning (Figure 2). 62 However, UBM remains superior in its ability to visualize structures behind the iris and through opaque media. 62 UBM is also capable of visualizing small posterior capsular tears with high accuracy. 62

UBM and SS-OCT imaging in a patient with a history of repaired penetrating injury in the left eye. (a) UBM showing the lens boundaries, with an apparent intact posterior capsule and (b) SS-OCT of the same eye revealing rupture of the posterior capsule. UBM: ultrasound biomicroscopy; SS-OCT: swept-source optical coherence tomography.
Intraocular foreign body (IOFB) is one of the most common diagnoses in eye trauma centers. 68 Over the past decade, the incidence of IOFB has increased. Intralenticular foreign bodies account for 5%–10% of all IOFB cases. 69 AS-OCT is a valuable diagnostic tool, typically revealing a hyperreflective area extending through the entire corneal thickness, a tear in the anterior lens capsule, and the presence of a foreign body within the crystalline lens (Figure 3).70,71 In rare cases, an intralenticular foreign body may be associated with intralenticular abscess formation, which is well visualized on AS-OCT. 72

Clinical examination of a patient with a history of trauma and decreased vision showing evidence of traumatic cataract. However, AS-OCT revealed additional findings of intralenticular foreign body (yellow arrow), characterized by a hyper-reflective lesion and posterior shadowing (indicated by the orange arrow).
In summary, traumatic cataract evaluation begins with the classification of the trauma as blunt or penetrating. Slit-lamp biomicroscopy remains the preferred method for initial examination. If slit-lamp examination is limited by media opacity such as corneal edema, hyphema, or dense cataract, AS-OCT can evaluate the posterior capsule and zonular integrity, guiding IOL selection. SS-OCT assessment can help guide diagnosis and surgical planning by identifying posterior capsule tears and anterior segment disruptions, locating intralenticular foreign bodies, and detecting abscess formation. In contrast, UBM is recommended for viewing structures through opaque media. A summary of these findings is presented in Table 1.
Summary of AS-OCT applications for traumatic cataracts.

AS-OCT: anterior segment optical coherence tomography; SS-OCT: swept-source optical coherence tomography; UBM: ultrasound biomicroscopy; IOL: intraocular lens; OCT: optical coherence tomography.
Traumatic extraocular muscle injury
AS-OCT has been primarily used for strabismus reoperation to visualize and access extraocular muscles.73,74 However, recent case reports have successfully employed AS-OCT to assess extraocular muscle injuries resulting from ocular trauma. 73 In these cases, AS-OCT proved valuable in delineating the morphology and insertions of extraocular muscles following trauma. 73 It has also been used to characterize intra-orbital foreign bodies based on their reflectivity patterns. In one case, AS-OCT identified a hyperreflective foreign body near the inferior rectus tendon, which was later confirmed using computed tomography (CT). Its removal corrected the “reverse leash effect” observed in that patient. 73
A previous study investigated the ability of AS-OCT to complement other imaging techniques such as CT and magnetic resonance imaging (MRI) in diagnosing traumatic extraocular muscle injuries. 75 Although CT and MRI are preferred for assessing posterior muscle injuries, AS-OCT has proven useful in visualizing insertions and scleral paths.73,75 This multimodal approach can improve the detection of partial muscle lacerations and allow personalized treatment. 75
In strabismus reoperations, AS-OCT is used for preoperative planning, wherein it facilitates the identification of muscle insertions and previously operated muscles. 74 Research has shown that 78.7% of muscles were correctly measured within a distance of ±1 mm, with a mean discrepancy of only 0.3 ± 0.89 mm from intraoperative values. 74 The same study reported that AS-OCT identified operated muscles in 97.8% of the cases, outperforming clinical examinations, and revealed features such as increased insertion distance, undulating scleral coats, hyperreflectivity, and overlying cysts, thus leading to a change in surgical plans in 39.2% of the patients in this study. 74
Despite its numerous applications, AS-OCT is limited by its cost and availability. Furthermore, it is less effective in patients with severe mobility restrictions or early postoperative inflammation. 74 Finally, AS-OCT may fail to detect some organic foreign bodies. 74
Traumatic angle and ciliary body abnormalities
AS-OCT is a pivotal diagnostic tool that offers high-resolution imaging of the AC and angle structures, including the scleral spur, ciliary body, angle recess, and iris root. Several studies have reported the concordance between AS-OCT findings and UBM parameters in identifying abnormalities of the iridocorneal angle, including measurements such as angle opening distance (AOD), angle recession area, trabecular-iris space area (TISA), and trabecular-iris contact length.76–78 Li et al. indicated that AS-OCT showed excellent repeatability and reproducibility in AOD and TISA measurements (intraclass correlation coefficient = 0.95–0.98 and 0.89–0.95, respectively). 79 This surpassed the more moderate reproducibility of UBM in angle measurements, as reported in previous studies. 80 However, in a previous study, unlike UBM, AS-OCT could not visualize structures behind the iris, which poses a challenge in cases of plateau iris and angle closure due to ciliary cysts (Figure 4). 81

AS-OCT image demonstrating an iris cyst obscuring the underlying posterior structures. AS-OCT: anterior segment optical coherence tomography.
In blunt trauma cases, detecting a cyclodialysis cleft and ciliary body detachment is crucial, considering the potential for severe ocular complications such as hypotony and vision loss. 82 Hyphema, opacity, and hypotonia can lead to the underestimation or omission of cyclodialysis cleft examination during slit-lamp gonioscopy, 83 while AS-OCT offers a panoramic and circumferential perspective of the entire extent of the cleft. 84 Moreover, AS-OCT has shown potential beyond its diagnostic role by offering a valuable means to track the resolution of cyclodialysis cleft extent and maximal effusion height.85,86 Furthermore, in cases of traumatic iridodialysis with corneal edema, conventional methods such as gonioscopy may not provide a clear evaluation of the AC. In a previous study, AS-OCT enabled precise visualization of iridodialysis, facilitating meticulous surgical planning and effective postoperative assessment. 87
Despite the significant advantages of AS-OCT, gonioscopy remains the clinical gold standard. Recent studies using deep learning models have reported a strong agreement between gonioscopy and AS-OCT images (CASIA, Tomey Corporation in Nagoya, Japan).88–90 However, SS-OCT often classifies a greater proportion of angles as narrow or occludable, suggesting a higher sensitivity in detecting angle closure.91–93 This highlights the importance of cautiously interpreting AS-OCT findings, keeping in mind its potential limitations.
In traumatic iritis, inflammatory cell precipitates may obstruct the trabecular meshwork and lead to secondary glaucoma. The quantitative evaluation of AC inflammation using AS-OCT holds significant clinical importance for both monitoring and prognosis assessment.94,95 In a previous study, the hyperreflective spots on AS-OCT, reflecting cell counts, aligned well with the clinical grading obtained using slit-lamp biomicroscopy, indicating that AS-OCT is a valuable tool for managing traumatic iritis. 96
Posterolateral forces of the aqueous humor as well as tearing between the longitudinal and circular fibers of the ciliary body lead to angle recession, iris root tearing, and subsequent hyphema formation. This insult can precipitate the development of angle recession glaucoma (ARG) within the first year 97 or up to a decade later. 98 Recession of angles >180° carries an approximate 5% risk of ARG. AS-OCT provides precise measurement of angle recession and widening of the ciliary body band as well as detection of associated conditions such as hyphema and peripheral anterior synechiae; it can be a useful tool for monitoring the progression of angle recession and development to ARG.99–101
In a case series of topiramate-induced angle-closure crisis, AS-OCT revealed anterior displacement of the iris, accompanied with ciliochoroidal detachment and anterior rotation of the ciliary body.102,103 These changes led to the shallowing of the AC and significant narrowing or closure of the iridocorneal angle, which prompted appropriate treatment intervention. Employing AS-OCT to assess the angle width, AC volume, and depth after medical control of intraocular pressure enables clinicians to monitor the treatment response.102,103
Either blunt or penetrating traumas can precipitate angle-closure glaucoma by lens displacement and subsequent pupillary block (Figure 5). AS-OCT is emerging as a pivotal diagnostic modality in identifying iris corneal adhesion and assessing the AC depth. Moreover, it enables precise monitoring of AC deepening and resolution of iridocorneal touch after laser peripheral iridotomy.22,87

Anterior capsule rupture of the crystalline lens and pupillary block in a patient with a history of repaired penetrating injury (red arrow) and traumatic cataract.
Several studies have developed automated systems based on deep learning to detect angle closure in AS-OCT images. Xu et al. developed deep learning classifiers based on convolutional neural networks that achieved high accuracy in detecting gonioscopic angle closure (area under the curve (AUC): 0.933 in cross-validation and 0.928 in test) and primary angle-closure disease (AUC: 0.964–0.952 in test) using automated analysis of AS-OCT images. 88 Fu et al. compared a deep learning approach for automated detection of angle closure using AS-OCT images with a quantitative feature-based system using AC parameters from AS-OCT. 104 The deep learning approach and quantitative feature-based system demonstrated AUC values of 0.96 and 0.90, respectively. 104 Thus, compared with AS-OCT alone, automated deep learning systems using AS-OCT images provide a more accurate and efficient diagnostic tool for evaluating iridocorneal pathologies.
Although many artificial intelligence models are trained using AS-OCT images to aid ocular diagnoses, they possess inherent limitations. For instance, these models are constrained by the inherent limitations of AS-OCT. 105 The quality of the images and diversity of the datasets also limit the efficacy of these models; if the models are not trained on diverse datasets, it introduces bias into the diagnostic tool. 105 Moreover, many ethical and legal concerns remain regarding the application of artificial intelligence in the clinical context. 106 A summary of traumatic angle and ciliary body abnormalities is presented in Table 2.
Summary of AS-OCT applications for traumatic angle abnormalities.

AS-OCT: anterior segment optical coherence tomography; SS-OCT: swept-source optical coherence tomography; UBM: ultrasound biomicroscopy; CNN: convolutional neural network; AI: artificial intelligence; AOD: angle opening distance; ARA: angle recession area; TISA: trabecular-iris space area; TICL: trabecular-iris contact length; ICC: intraclass correlation coefficient; PAS: peripheral anterior synechiae; IOP: intraocular pressure; AC: anterior chamber; LPI: laser peripheral iridotomy; AUC: area under the curve; DL: deep learning.
Infectious keratitis
AS-OCT, a noncontact, high-resolution imaging modality, has the ability to precisely detect the depth and extent of corneal infiltrations (Figures 6 and 7). Although slit lamps solely identify the site and size of the corneal pathologies, in cases where significant stromal necrosis masks the underlying tissue, cross-sectional AS-OCT images enable quantitative and qualitative assessment of corneal pathology, facilitating disease progression monitoring and treatment response evaluation.107–109

AS-OCT in a patient with keratitis. (a) AS-OCT showing epithelial irregularity (red arrow) and hyperreflectivity corresponding to the site of a corneal ulcer and (b) measurement of stromal infiltration depth observed on AS-OCT. AS-OCT: anterior segment optical coherence tomography.

Corneal ulcer scarring in two different patients. (a) AS-OCT showing a healed corneal ulcer with a superficial scar and (b) AS-OCT showing a deeper and thicker corneal scar in the second patient. AS-OCT: anterior segment optical coherence tomography.
In a previous study, AS-OCT enabled the precise detection of stromal infiltration thickness and corneal thickness, accurately assessing the risk of perforation, particularly prior to clinical deterioration, even when it was not apparent on slit-lamp examination. 110 Meticulous evaluation of corneal thickness is imperative for mitigating the progression to severe thinning conditions such as corneal melting observed during slit-lamp examinations. 111 Tawfeek et al. reported that AS-OCT outperformed slit-lamp examination in monitoring the healing process of corneal epithelium, stroma, scar formation, and the layers which cannot be tracked using slit-lamp examination. 112
In cases of Acanthamoeba keratitis (AK), AS-OCT images reveal a distinctive feature termed “radial keratoneuritis,” characterized by hyperreflective bands spanning variable depths, from the subepithelial stroma to the mid-stroma, with widths ranging between 20 and 200 µm. Notably, these features often subside with appropriate treatment. Unlike in vivo confocal microscopy, AS-OCT cannot detect cysts or trophozoites due to limited resolution. 113
Herpetic epithelial keratitis (HEK) and AK can present with similar clinical features, making their differentiation challenging in certain patients. Although HEK and AK share some characteristic features on AS-OCT imaging, the hyperreflective bands seen in HEK are confined to the subepithelial area and do not extend into the stroma. Additionally, HEK may present with corneal epithelial irregularity in some patients, unlike AK. 114 Given that deep stromal involvement is indicative of poor visual outcomes in AK, cross-sectional AS-OCT images may facilitate the assessment of prognosis in AK patients. 115
Soliman et al. delineated a comprehensive range of features evident in AS-OCT images of HEK. 116 They described herpetic corneal infiltrates as diffuse or localized hyperreflective spindle-shaped areas. They further noted the presence of post-herpetic neurotrophic ulcers, identified by stromal thinning and hyperreflectivity, accompanied with an epithelial defect. Additionally, they characterized post-herpetic scars as hyperreflective stroma with an intact epithelium. Although the proposed spectrum of HEK features lacked pathognomonic specificity for HEK diagnosis, they can serve as valuable tools in treatment management. 116 In a study involving two patients with disciform keratitis, Hixson et al. assessed treatment response by pinpointing microcystic edema and keratic precipitates (KPs) on AS-OCT images. 117 The resolution of corneal edema and KPs in conjunction with therapeutic interventions underscored the utility of AS-OCT in monitoring HEK patients. 117
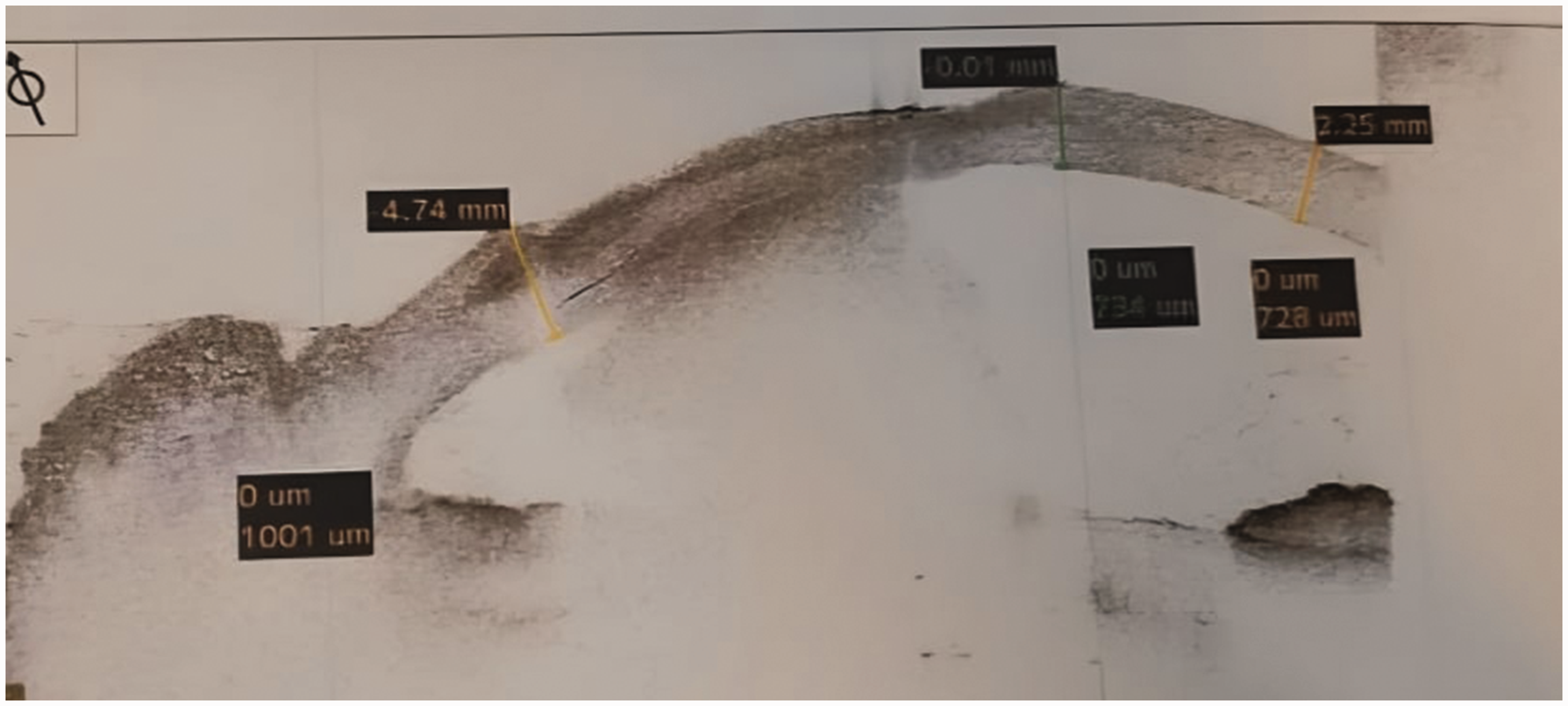
Khalil et al. developed a predictive model for the detection of Pseudomonas aeruginosa keratitis utilizing three AS-OCT parameters, including infiltrate thickness, infiltrate diameter, and tissue gain/loss. 118 This predictive model demonstrated a relatively high sensitivity of 85.7%, high specificity of 91.7%, and AUC of 0.929, indicating excellent overall accuracy in discriminating Pseudomonas keratitis from other conditions. Assessment of tissue gain using AS-OCT images, which reflects initial inflammatory response and corneal edema, is crucial for establishing a diagnosis. 118 Elevated levels, surpassing 30%, were indicative of Pseudomonas keratitis, while lower values, approximately 15%, were commonly associated with gram-positive bacterial keratitis (BK). 118
In AS-OCT imaging of fungal keratitis, the presence of localized or full-thickness cystic spaces of varying sizes, indicative of stromal necrosis, is a notable observation. 119 However, this feature is commonly associated with fungal keratitis and potentially with severe stages of BK. 120 Hyperreflective inflammatory plaques attached to the corneal endothelium, known as retro-corneal plaques, can be detected in viral, bacterial, and fungal keratitis. In bacterial and viral keratitis, retro-corneal plaques typically exhibit clear boundaries with the endothelial corneal surface, occasionally with a space between the plaque and endothelium, and tend to resolve with treatment (Figure 8). However, in fungal keratitis, the boundaries of these plaques are often unclear, necessitating surgical intervention for resolution.121,122
AS-OCT image of bacterial keratitis showing a well-defined retro-corneal plaque with sharp boundaries. AS-OCT: anterior segment optical coherence tomography.
Konstantopoulos et al. 123 showed a significant correlation between corneal morphological properties and the level of inflammation in BK. They concluded that higher corneal and infiltrate thickness in gram-negative BK compared with that in gram-positive BK corresponded to greater levels of inflammatory cytokines. Although confirmatory diagnosis and determination of the causative organism in BK require microbiological smear and culture, such findings in AS-OCT can provide valuable guidance in predicting the possible causative pathogen. 123
In cases of interface infectious keratitis following lamellar keratoplasty, femtosecond LASIK (Femto LASIK), or small incision lenticule extraction, AS-OCT images can precisely detect the location of deep-seated infections as hyperreflective areas at the graft–host interface. However, these infiltrations are not diagnostic for the causative agent, and the hyperreflective infiltrates may typically resolve with intensive medical or surgical interventions.110,124–126
Patients with infectious keratitis commonly exhibit significant irregularity on the anterior and posterior surface of the cornea, as detected via AS-OCT. The measurement of corneal higher-order aberrations using three-dimensional reconstruction of AS-OCT images can offer an objective method for assessing visual outcomes in these patients.127,128 Ichikawa et al. reported that quantitative measurement of corneal densitometry using AS-OCT can provide a comprehensive evaluation of corneal scarring and astigmatism following the treatment of infectious keratitis. 129 They demonstrated a notable rise in corneal densitometry for all types of infectious keratitis. The increase in corneal thickness was more substantial in cases of fungal keratitis and AK than in cases of bacterial and herpetic infections. 129 A detailed summary of AS-OCT findings for infectious keratitis is presented in Table 3.
Summary of AS-OCT applications for infectious keratitis.
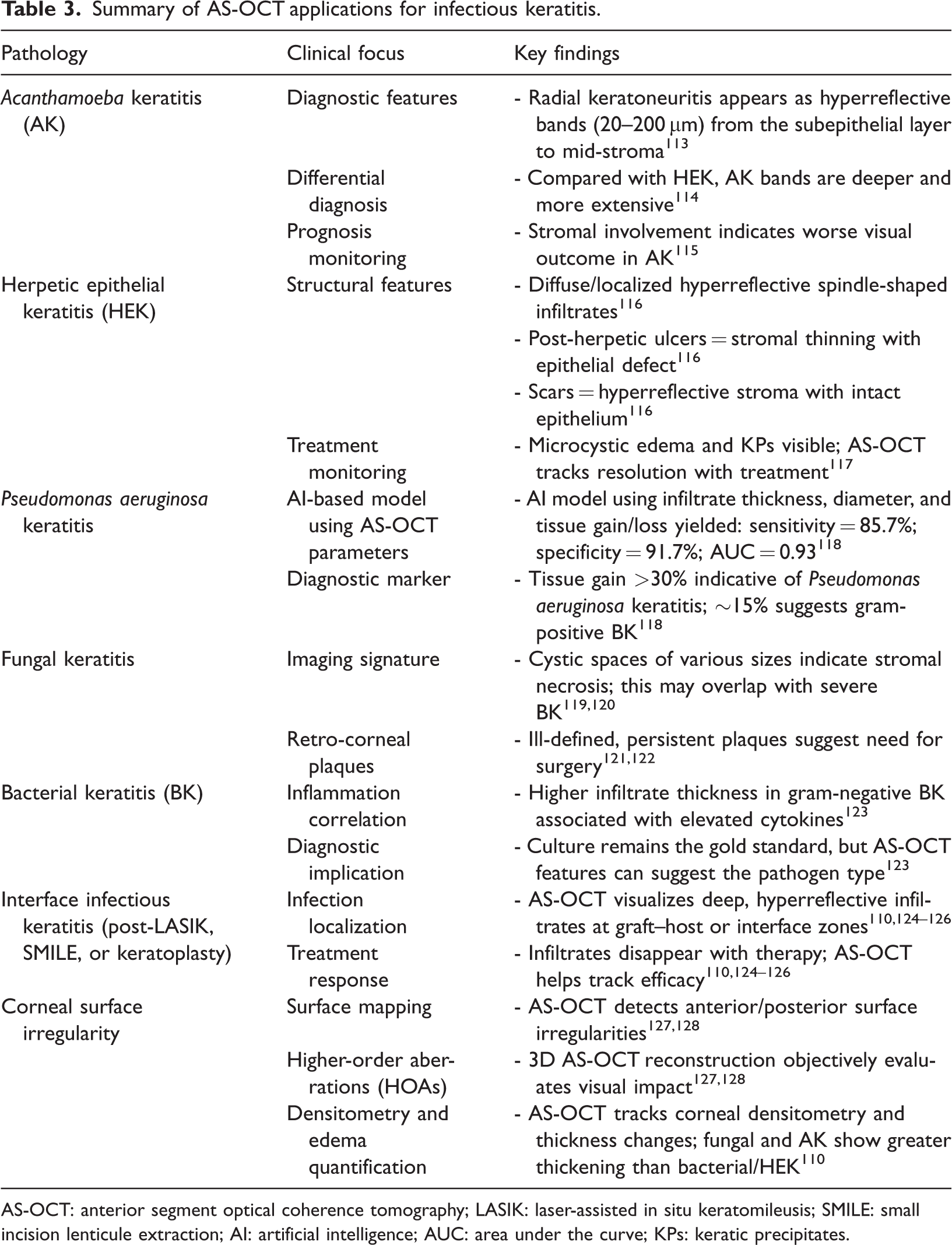
AS-OCT: anterior segment optical coherence tomography; LASIK: laser-assisted in situ keratomileusis; SMILE: small incision lenticule extraction; AI: artificial intelligence; AUC: area under the curve; KPs: keratic precipitates.
Implications and limitations
A review by Han et al. revealed that AS-OCT served as a useful tool for evaluating the depth of injury from ocular trauma, emphasizing its ability to evaluate anterior structural damage without any contact with the affected eye. 130 Chong et al. also discussed the ability of AS-OCT to differentiate between types of infectious keratitis and corneal foreign bodies through characteristic imaging findings. 110
Several literature reviews, such as those mentioned above, have briefly discussed the use of AS-OCT within a broader context. However, to the best of our knowledge, none of them have comprehensively focused on the application of AS-OCT in ocular emergencies. By consolidating this information, we provide clinicians with a starting point for future research and clinical decision-making.
Although this review encompasses a broad range of ocular emergencies, it is limited by its narrative structure. It does not follow any formalized guideline, registered screening protocol, or structured bias assessment for the articles included in the study. Studies included in this review were restricted to manuscripts published in English in major databases (PubMed, Scopus, and Web of Science). Finally, some key anterior segment ocular emergencies may have been overlooked.
Conclusion
AS-OCT has revolutionized the evaluation and management of ocular trauma and emergencies by enabling high-resolution, noncontact imaging of the anterior segment. Its ability to detect subtle structural abnormalities, even in cases where corneal opacity or hyphema obstructs clinical examination, makes it an invaluable tool for timely diagnosis and treatment planning. AS-OCT enhances the assessment of corneal injuries, foreign bodies, traumatic cataracts, extraocular muscle injuries, and angle abnormalities, offering detailed insights that improve surgical decision-making and long-term patient outcomes. Moreover, the advent of AS-OCTA has further expanded its role in assessing vascular changes, such as limbal ischemia in chemical burns. Despite its advantages, AS-OCT has limitations, including its inability to penetrate beyond the iris and its reliance on patient cooperation. Future advancements in imaging resolution, penetration depth, and integration with artificial intelligence may further refine its diagnostic and prognostic applications. Overall, AS-OCT has been established as a crucial modality in emergency and trauma care settings, significantly enhancing clinicians’ ability to manage complex anterior segment injuries and improve visual outcomes.
Footnotes
Acknowledgments
Not applicable.
Author contributions
H.A. conceptualized and designed the study, supervised the research process, and contributed to data interpretation. A.M., K.D., H.E., and A.R. contributed to data collection and analysis. H.Es. and P.A. provided critical revisions and guidance on methodology. G.G. assisted in manuscript drafting and final review. O.N. contributed significantly to the revisions of this manuscript. M.S. played a pivotal role in overseeing the study’s execution, ensuring methodological rigor, and coordinating manuscript preparation. All authors reviewed and approved the final version of the manuscript.
Data availability
Not applicable.
Declaration of conflicting interests
The authors declare no conflicts of interest related to this study.
Ethics approval
This review did not involve original research with human participants. Anonymized patient AS-OCT images were used for illustration, in accordance with the Declaration of Helsinki.
Funding
No external funding was received for this study.
Informed consent
All patient images used in this study were obtained with informed consent, ensuring anonymity and compliance with ethical guidelines.