
Abstract
Tissue banking programs fail to meet the demand for human organs and tissues for transplantation into patients with congenital defects, injuries, chronic diseases, and end-stage organ failure. Tendons and ligaments are among the most frequently ruptured and/or worn-out body tissues owing to their frequent use, especially in athletes and the elderly population. Surgical repair has remained the mainstay management approach, regardless of scarring and adhesion formation during healing, which then compromises the gliding motion of the joint and reduces the quality of life for patients. Tissue engineering and regenerative medicine approaches, such as tendon augmentation, are promising as they may provide superior outcomes by inducing host-tissue ingrowth and tendon regeneration during degradation, thereby decreasing failure rates and morbidity. However, to date, tendon tissue engineering and regeneration research has been limited and lacks the much-needed human clinical evidence to translate most laboratory augmentation approaches to therapeutics. This narrative review summarizes the current treatment options for various tendon pathologies, future of tendon augmentation, cell therapy, gene therapy, 3D/4D bioprinting, scaffolding, and cell signals.
Keywords
Introduction to tissue engineering and regenerative medicine (TERM)
In recent years, advances in biomedical research have produced significant milestones in new drug discovery, medical devices, and clinical procedures. One breakthrough of biomedical research advancements in the past three decades was the emergence of TERM. The intention of this field is based on the idea that tissue and organ reconstruction can restore patient’s normal lives after organ loss/injury. The terms tissue engineering (TE) and regenerative medicine (RM) are typically used separately and interchangeably to mean one thing (TERM), although there is a marked difference in the technicalities of the fields. TE focuses more on creating in vitro bio-artificial tissues or cellular products to repair tissues within the body and involves in vivo alteration of cell growth and function through the implantation of suitable cells isolated from donor tissue and biocompatible scaffold materials. 1 In contrast, RM focuses on endogenous tissue formation. 2 The three most important components of TERM are biomaterials, cells, and signals. 3
Although a well-defined field (TERM) has recently been developed, its foundation can be traced back to the year 300 BC in Indian writings that described skin grafting in Sanskrit texts. 4 TERM became recognized in the mid-1950s when the first kidney transplant between identical twin brothers was successfully performed. 5 The field aims to solve problems related to diverse backgrounds, such as acute or chronic degenerative diseases, trauma, aging, and congenital defects, and hence overlaps with other disciplines, including biomaterials, nanotechnology, stem cell biology, developmental biology, engineering, and medicine. 6 In the field of medicine, orthopedics has greatly benefited from the technological evolution of TERM. However, to date, tendon TE and regeneration research has been limited and lacks the much-needed human clinical evidence to translate most laboratory augmentation approaches to therapeutics. Previous review articles7–13 have also performed a similar review; however, the current study conducted an extensive review of current literature to help with the limited translation of tendon augmentation in clinical practice and provide a better understanding of tendon repair in TERM.
Search strategy
A review of published articles on tendon augmentation was performed. Scientific literature was searched in relevant databases (Google Scholar, Scopus, PubMed, and Web of Science) using the terms “(regenerative medicine) AND (tissue engineering) AND (tendon repair OR tendon augmentation) AND (bio-fabrication)”. The search was conducted with publication language restricted to English. The titles of articles were reviewed, followed by the abstracts and full texts. After the removal of duplicates and unrelated papers, 96 articles were used in this narrative review. This article does not contain any studies with human participants or animals performed by any of the authors. Therefore, ethical approval and informed patient consent were not required.
TE in tendon/ligament augmentation
TE research in tendon augmentation intensified in the early 1980s, resulting in the first commercial product Gore-Tex Cruciate Ligament prosthesis (WL Gore and Associates, Newark, DE, USA) being approved by the Food and Drug Administration (FDA) on 10 October 1986. 14 Since 1986, more commercial products have been approved, mostly in the USA by the FDA but also in Europe and across the world. Commercial augmentation products are being developed for the increased tendon injury burden from workplaces and age-related conditions, with approximately 30% to 50% of sports injuries involving tendon injuries. 15 Currently, surgical repair remains the gold standard treatment for tendon/ligament rupture. However, the healing process is naturally lengthy relative to that of other soft tissues.11,16 This is partly because tendons are tissues of high activity with a poor blood supply, supporting fundamental locomotion of the body. As a result, they are highly prone to healing failure, thereby increasing morbidity and additional treatment costs and placing an economic burden on patients and health systems.11,15,17
TERM approaches have been studied and proposed as promising alternatives to improve the quality of tendon healing.18,19 The fields of engineering, nanotechnology, molecular biology, and materials science are used alone or in combination with cells, scaffolds, and bioactive molecules in various TERM approaches. 15 Despite showing great potential, tendon argumentation suffers from limited evidence in the literature to support the clinical use of various scaffold biomaterials. 20 This is partly because there is a poor understanding of the basic biology of tendon development, signal transduction, mechanotransduction, and mechanisms underlying tendon pathogenesis and healing and limited translational animal models and well-designed preclinical studies, all because there are only a few researchers working in this area.21–25
Tendon development, histology, and physiology
Tendons together with muscle, muscle connective tissue, ligament, bone, nerves, and blood vessels are part of the musculoskeletal system, which is vital for structural support, locomotion, and movement.26,27 The main function of tendons is to join muscles to bones and transfer forces necessary for movement. 28 The embryological derivative of tendons is the ectoderm. 29 Tenocytes are mature tenoblasts found in the tendon that were previously thought to be the only resident cells before the discovery of tendon stem cells (TSCs). 30 Tenocytes and tenoblasts represent nearly 90% to 95% of the cells within the tendon, with the other 5% to 10% consisting of chondrocytes, synovial cells, and vascular cells. 31
Tenocytes and tenoblasts are specialized fibrocytes and fibroblasts, respectively, that secrete extracellular matrices, such as collagen, proteoglycans, and other proteins. 31 Tenocytes control the repair, maintenance, and turnover of the extracellular matrix in response to external stimuli and stress. 29 Tendons are mainly composed of collagen, which accounts for 70% to 80% of their dry weight, including 95% type 1 collagen and 5% type 3 collagen present in the epitenonium and endotenonium. 32 Tendons have collagen fibrils that bundle to make collagen fibers, forming fascicles, and bundles of fascicles from the fascicular matrix. Endotendon contains blood vessels, lymphatics, and nerves, and its outward continuation forms the epitenon, a synovial-like membrane that prevents adhesion of the tendon to other adjacent tissues. 33
TSCs are in some ways different from tenocytes, including differences in cell marker expression, proliferative and differentiation potential, and morphology. 30 TSCs differentiate into adipocytes, chondrocytes, and osteocytes in vitro and form tendon-, cartilage-, and bone-like tissues in vivo. 34 The study by Zhang J et al. showed that low mechanical stretching at 4% stimulated the differentiation of TSCs into tenocytes, whereas stretching at 8% induced the differentiation of a sub‐population of TSCs into adipogenic, chondrogenic, and osteogenic lineages. 34 Therefore, understanding the mechanobiology of TSCs can potentially improve the effective repair or regeneration of injured tendons.
The microstructure of tendons also comprises connective tissue tendon sheaths, fibrous sheaths, synovial sheaths, peritendon sheaths (paratenon), reflection pulleys, and tendon bursae. These structures are specialized to enhance tendon efficiency by improving the sliding motion of the tendon tissue, reducing friction with neighboring anatomical structures, and preventing the tendon from losing its course of action during muscle contraction. 35
Tendon pathologies and current approaches to management
A summary of the management of tendon pathologies is shown in Table 1. Tendon injuries remain a significant cause of both work-related and sport-related injuries. 15 The repair of tendon injuries is a lengthy process that frequently results in a poor structural, mechanical, and functional quality of the healed tissue. At present, the clinical options for treating tendon injuries are often unsatisfactory, especially in elderly populations. 35
Summary of the management of tendon pathologies.

Mesenchymal stem cells (MSC), tendon-derived stem cells (TDSCs), l-lactic acid-co-ε-caprolactone (poly(LLA-CL)/Col), collagenase clostridium histolyticum (CCH), platelet-rich plasma (PRP), non-steroidal anti-inflammatory drugs (NSAIDs), disease-modifying antirheumatic drugs (DMARDs).
Novel methods used in tendon augmentation
Gene therapy
In the TE of tendons, genetic vector transfer is used as a biological delivery system to deliver the encoded gene products to the site of pathology to promote the local repair and regeneration of damaged tissues.35,67–69 Identifying and transferring genes into a local cell, resulting in the translation of the gene into specific protein-like growth factors, is the basis of this approach. Growth factors, such as vascular endothelial growth factor (VEGF), growth differentiation factor-5, platelet-derived growth factor-b (PDGF-b), and insulin-like growth factor-1 (IFG-1), are among the previously studied growth factors, and their effects have been characterized in local tendon cells. 70 Localized gene transfer allows focal post-translational protein synthesis, which leads to greater biological activity and a reduced risk of activating immune reactions. 35 Because of poor blood supply to joint structures, such as tendons, it is difficult to deliver therapeutics intravenously, intramuscularly, and orally without exposing the body systemically to the therapeutic agent. Therefore, local delivery methods, such as gene transfer, prove to be more advantageous.71,72 An additional benefit of using a gene-therapy, tissue-engineered approach to affect tendon healing is that it allows the physician to select specific growth factors in the tendon-healing cascade from well-documented sources. 70
An alternative novel approach to using pure vectors is the application of gene-modified sutures, as demonstrated by Zhou et al. 73 Plasmids, such as pEGFP-bFGF, are loaded onto nanoparticles to form nanoparticle/plasmid complexes, and then the complexes are attached to the surface of polydopamine-modified sutures to prepare nanoparticle/plasmid complex-coated sutures, which are then used for tendon repair to promote tendon healing. The outcome of their study showed that gene-modified sutures (nanoparticle/pEGFP-bFGF and pEGFP-VEGFA complex-coated) improved tendon healing by increasing tendon healing strengths, enhancing gliding function, and inhibiting adhesion formation without adverse effects on host tissues. 73 Table 2 summarizes studies on novel methods applied in tendon management.
Novel methods applied in tendon management.
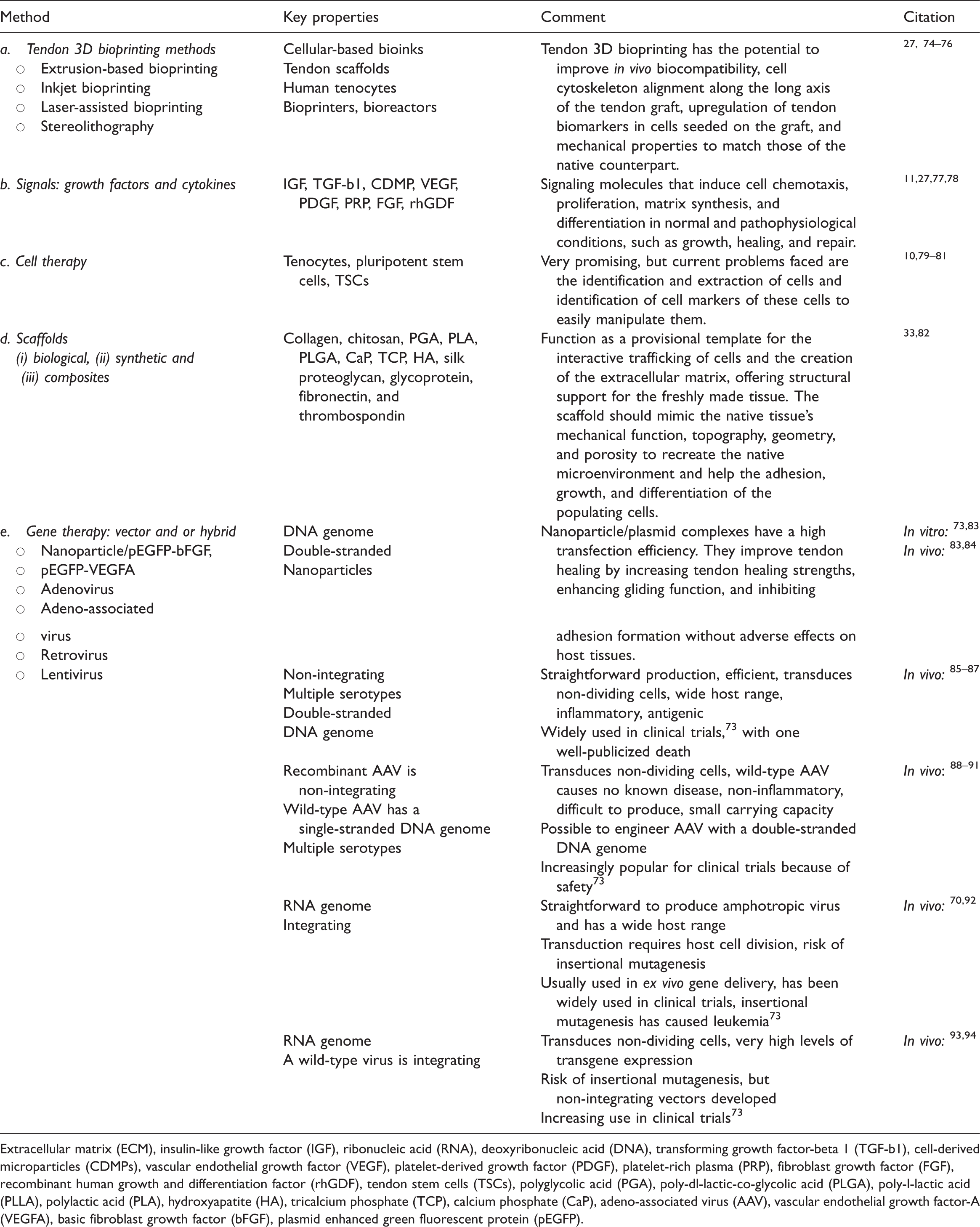
Extracellular matrix (ECM), insulin-like growth factor (IGF), ribonucleic acid (RNA), deoxyribonucleic acid (DNA), transforming growth factor-beta 1 (TGF-b1), cell-derived microparticles (CDMPs), vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), platelet-rich plasma (PRP), fibroblast growth factor (FGF), recombinant human growth and differentiation factor (rhGDF), tendon stem cells (TSCs), polyglycolic acid (PGA), poly-dl-lactic-co-glycolic acid (PLGA), poly-l-lactic acid (PLLA), polylactic acid (PLA), hydroxyapatite (HA), tricalcium phosphate (TCP), calcium phosphate (CaP), adeno-associated virus (AAV), vascular endothelial growth factor-A (VEGFA), basic fibroblast growth factor (bFGF), plasmid enhanced green fluorescent protein (pEGFP).
Cell therapy
Cells are among the three pillar components of TERM. Stem cells, sometimes called “medicinal stem cells,” work effectively as growth factor factories or drugstores in vivo. 95 Stem cells can repopulate the injured tissue and stimulate the body’s healing properties. In tendon TE, tenocytes, TSCs, bone marrow-derived mesenchymal stem cells, MSCs, pluripotent stem cells, and embryonic stem cells are the most commonly used and most promising. The current problems faced in TE cell therapy are the identification and extraction of these cells and the identification of cell markers to easily manipulate them for a better understanding of tendon pathophysiology. A 2010 study reported that TSCs differed from tenocytes in morphology in culture, proliferative potential, stem cell marker expression, and differentiation potential. 30 The application of undifferentiated stem cells for the repair of tendon injuries, such as bone marrow-derived mesenchymal stem cells (MSCs), adipose tissue-derived MSCs, embryonic stem cells, embryonic stem-like cells, adipose-derived nucleated cells, umbilical cord blood-derived MSCs, and peripheral blood-derived mesenchymal stem cells, has been well characterized. 96 Furthermore, the author mentions that MSCs used in tendon regeneration have the potential to recruit other MSCs or progenitor cells to the injury site by producing a variety of cytokines and paracrine factors, thereby improving the regeneration potential.
Challenges with cell therapy mainly include the efficacy evaluation of MSC therapy, which is subject to the use of appropriate control groups, severity and size of the lesion, time between injury and implantation, number of stem cells for implantation, models of tendinopathy (e.g., collagenase or surgical disruption), and opting for single or multiple injections. 96
Signals: growth factors and cytokines
Growth factors are signaling molecules that induce cell chemotaxis, proliferation, matrix synthesis, and cell differentiation in normal and pathophysiological conditions, such as growth, healing, and repair. 11 The regulation of these signals during tendon injury repair is of great importance, especially in controlling the amount of scar tissue production. Extensive scar tissue at the healing attachment site may predispose patients to impingement post-operatively. Important factors to consider when adding growth factors to cell culture media to trigger tenogenic differentiation are incubation time and cell type. In clinical scenarios, several modes for the delivery of growth factors to the injury site can be applied, including direct local injection and the use of impregnated sutures or scaffolds. Impregnated sutures or scaffolds are better at delivering growth factors to the specific area of injury without the overflow loss associated with local injection. However, local injection is comparatively non-invasive, simple, and quick, although growth factors delivered in this way only remain at the site for a short duration. 11
IGF, transforming growth factor β1 (TGF-β1), and cartilage-derived morphogenetic protein growth factor-1, -2, and -3 are equivalent to human bone morphogenic protein (BMP)-14, -13, and -12. PDGF, epidermal growth factor, platelet-rich plasma, VEGF, interleukin-10, recombinant human osteogenic protein-1, connective tissue growth factor, fibroblast growth factor (FGF), and recombinant human growth differentiation factor have all been characterized in terms of their roles in tendon injury repair.
In several studies, PDGF-stimulated DNA and matrix synthesis in tendon cells11,14 increased the expression of cell surface integrins, which play critical roles in tendon repair. 22 IGF-1 also enhances healing by increasing DNA, collagen, and glycosaminoglycan production. In vitro and in vivo studies have elucidated the ability of IGF-1 to decrease swelling and simultaneously increase cell proliferation, collagen synthesis, and DNA content. 70 FGF2 is among the most promising cell signals in tendon augmentation and has been widely reported to increase tendon/ligament revascularization, cell proliferation, and collagen production and stimulate new bone formation, accelerating tendon-to-bone healing.83,97,98
Scaffolding
According to Mota et al., a scaffold is a material that functions as a provisional template for the interactive trafficking of cells and the creation of the extracellular matrix, offering structural support for the freshly made tissue. 82 Tendon scaffolding material comes in three main forms: biological, synthetic, and composite. 33 Table 3 compares the types, sources, strengths, and weaknesses of scaffolding material used in tendon augmentation.
Comparison of scaffolding material.

Poly-l-lactic acid (PLLA), polyethylene oxide (PEO), polyglycolic acid (PGA), polylactic acid (PLA).
Regardless of the type, an effective scaffold should have appropriate biocompatibility, biodegradability, biokinetics, porosity, and biomechanical properties close to the target natural tissue’s predefined geometry and size. 82 From Table 3, it is clear that all three forms of scaffolds have strengths and weaknesses. Synthetics have a great deal of versatility and high mechanical strength and hold a greater potential for high-volume industrial production than others. 100 However, synthetic scaffolds are relatively immunogenic, have low hydrophilic properties, and lack sufficient cell adhesive properties. Biologic scaffolds are harvested from mammalian tissues, such as human, porcine, bovine, and equine, and are the most studied type of scaffolding. 101 Biologics have adequate cell adhesion properties, low immunogenicity, and high hydrophilicity, although their mechanical strength is the lowest. Composite scaffolding attempts to combine the advantages of biological and synthetic scaffolds, offering improved biocompatibility and lower degradability; however, its mechanical properties still present a challenge. 102
The ideal augmenting scaffold would be able to stimulate endogenous tendon tissue regeneration during degradation and reduce in vivo mechanical forces on tendon repair during post-operative healing. Biologics (extracellular matrices) have great potential in achieving this; however, current clinical evidence is limited because there are only a few well-conducted human studies in this area.11,20 Table 4 describes the in vivo and in vitro laboratory studies on scaffolding materials in tendon augmentation.
In vivo and in vitro laboratory studies on scaffolding materials in tendon augmentation.

Carboxyl-functionalized carbon nanotubes (CNT-COOH), N-acetylglucosaminidase (NAG), nitric oxide (NO), poly-l-lactic acid (PLLA), polyglycolic acid (PGA), polylactic acid (PLA), graphene nanoplatelets (GNP), poly(lactide-co-glycolide) (PLGA), bone marrow stromal cells (bMSCs), demineralized bone matrix (DBM), poly(ε-caprolactone) (PCL), l-lactic acid-co-ε-caprolactone (poly(LLA-CL), deoxyribonucleic acid (DNA), tendon-derived stem cells (TDSCs), adipose-derived stem cells (ADSCs), polymerase chain reaction (PCR), phosphate-buffered saline (PBS), scanning electron microscopy (SEM).
Nanotechnology in tendon augmentation
The National Science Foundation defines nanotechnology as “the ability to understand, control, and manipulate matter at the level of individual atoms and molecules, as well as at the “supramolecular” level involving clusters of molecules (in the range of about 0.1 to 100 nm) to create materials, devices, and systems with fundamentally new properties and functions because of their small structure”. 106 In nanomedicine, new advancements in nano-adjuvants, NanoKnife, oncology, orthopedic drug delivery, implantable materials, vertebral disk regeneration, and diagnostic modalities have been described and currently hold a promising future in TERM.46,107–109
The use of nanomedicine in tendon regeneration and repair is related to the individual physicochemical properties of particles and holds promise for improving extrinsic and intrinsic tendon healing with less adhesion compared with post-surgical adhesion.46,110 Nanofibers, such as Poly (caprolactone)-Based Nanofiber Electrospun Scaffolds, have shown promising results in various tissue regeneration applications in bone, cartilage, skin, tendon, ligament, and nerve. 111 Silver nanoparticles (AgNPs) are among the most widely used nanoparticles because they have anti-microbial and anti-adhesion effects, modulate the extracellular matrix composition, and promote the proliferation of primary tenocytes to AgNPs and the production of extracellular matrix components. 112 An earlier study reported that a polylactic-co-glycolic acid nanofiber-based scaffold system showed potential for functional human rotator cuff repair. 103 Nanoparticles can also be used as combination therapies. For example, Zhou et al. delivered a gene therapy to modulate gene expression, enhancing tendon healing and decreasing adhesions. The researchers transfected disrupted digital flexor tendon tenocytes with miRNA plasmids complexed with polylactic-co-glycolic acid [nanoparticles to form nanoparticle/TGF-β1 miRNA plasmid (nanoparticle/plasmid)], with improved efficiency. 84 Thus, nanotechnology remains a pivotal partner of tendon augmentation technology.
3D and 4D printing/additive manufacturing (AM) in tendon/ligament augmentation
AM, loosely called 3D printing, is a computer-assisted fabricating technique that uses precise geometry and computer-aided design to produce structures with complex geometries in a wide variety of fields. This involves the controlled deposition of a binder material laid on a powder layer using various AM techniques, such as inkjet printing and laser sintering, to produce constructs of complex geometry.82,113,114 Bioprinting is a method of AM that combines and assembles biomaterials, bioactive molecules, and cells to generate complex tissue-engineered structures. 113 This technique has been widely used in TERM studies, and its application holds tremendous hope in designing and bio-fabricating organs of complex shapes and microstructures with a high degree of automation, low production cost, high speed and volume, good accuracy, and reproducibility.82,115 Bioprinting has been applied in the manufacturing of various organs and tissues in vitro, including vascular tissues, skin, liver, neural tissue, heart, kidney, cartilage, bone, and skeletal muscles.116–118
Although there are extremely few studies on tendon 3D bioprinting, Merceron et al. managed to bioprint a 3D complex muscle-tendon unit structure using 3D integrated organ printing technology in vitro. 75 In another rabbit model, 3D desktop printers were used to print an anterior cruciate ligament surgical implant. After 4 and 12 weeks, an in vivo assessment of rabbit anterior cruciate ligament models showed that the scaffold was full of MSCs and displayed significant bone ingrowth and bone-graft interface formation within the bone tunnel. 119 Moreover, in an in vivo porcine study, Zhang et al. investigated mechanical and biological properties, fabrication methods for ligament-bone composite scaffolds, and problems between 3D printed ligament grafts and host bones in ligament reconstruction surgery using ligament-bone composite scaffolds. The team concluded that ligament-bone composite scaffolds established using the 3D printing technique accelerated the regeneration of the biomimetic ligament-bone interface. 120 3D bioprinting technology can be classified into three sub-types: inkjet-based, laser-assisted, and microextrusion-based printing. 76
Extrusion-based bioprinting (also called direct ink writing) is the most commonly used type of 3D printing in TE applications and is implemented by most commercially available systems, with several distinct advantages.76,121 Some advantages of this technique include high versatility, affordability, ease of use, multiple print heads allowing for printing multiple materials within a single construct, printability of highly viscous bioinks (30–6 × 107mPa s−1), and printability of structures with high cell densities (including cell spheroids). 27,121,122 The most significant drawback of extrusion-based bioprinting is that cell viability and functions are reduced as cells are exposed to shear stress when passing through the nozzle and pressure while in the syringe before extrusion. 123 In addition, this method has a relatively lower printing speed and resolution, which is highly dependent on setup. Extrusion-based bioprinting has three sub-systems (pneumatic, piston, and screw driven), which makes it versatile and compatible with some hydrogels, including alginate, gelatin, chitosan, hyaluronic acid, Pluronic F-127, and polyethylene glycol.124,125
Inkjet and laser-assisted techniques have tremendous resolutions and cell viabilities. Inkjet bioprinting is fast and cheap and has diverse applicability for different types of materials. Disadvantages of the inkjet technique include limitations to bioinks with a viscosity of 3.5 to 12 mPa s−1 and low cell density (<106 cells mL−1). 27 Laser‐assisted bioprinting is a complex and expensive system with a high degree of precision and resolution that can print a high cell density (∼108 cells mL−1). However, it is a fast-printing system with high applicability in the micropatterning of cells and biomolecules because of its high printing resolution. 126
Stereolithography (including digital light processing) is a complex system with high applicability in multi-material bioprinting, resolution of bioprinting (∼1 µm), and cell viability (>85%). It is equivalent to extrusion bioprinting in these areas but requires a large number of cells as the entire bath volume must be filled. 121 Stereolithography has high printing costs and is restricted to only photo-cross-linkable materials, a single bioink per construct, and a uniformity (both density and distribution of phenotype) of included cells.27,121,125
Process of 3D tendon bioprinting
The process of bioprinting (Figure 1) begins with data acquisition, during which 3D models are acquired indirectly using X-ray, computed tomography, and magnetic resonance imaging techniques to scan and reconstruct or directly using computer-aided design software. Then, bioinks are carefully selected to guarantee biocompatibility, printability, and mechanical properties. The appropriate configuration of printing parameters needs to be confirmed before bioprinting. Finally, after printing, the implanted cells should create bonds and generate some structures and functions of the natural tissue/organ through physical and chemical stimulation of the target (receptors/signals). 125

Illustrating the stages involved in the process of tendon bioprinting.
If 3D bioprinting can create cadaveric tendons, then it is reasonable to think that 4D bioprinting will create “living” tendons owing to automation. While 3D printing still offers more futuristic approaches, its fundamental principle faces the limitation of producing only static, non-animating constructs that lack time-dependent dimensions and ultimately fail to mimic dynamic human tissues.127,128 In contrast, 4D bioprinting uses smart materials that exhibit changes in physical or chemical properties in a controlled and functional manner upon exposure to an external stimulus, such as heat, moisture, light, magnetic field, or pH.
129
Moreover, unlike 3D, 4D printed constructs have the five following unique properties:129,130
Shape memory: material changes into a predefined shape in response to an external stimulus Self-assembly: exposure to external stimulus induces the folding of chains and assembly into a preprogrammed shape Self-actuating: automated actuation of material upon exposure to an external stimulus Self-sensing: material detects and quantifies the exerted external stimuli Self-healing: damage caused in the structure is repaired without any external intervention
4D printing in orthopedics is still rare. In 2018, Haleem et al. 131 postulated the potential application of 4D printing in constructing smart orthopedic 3D implants, smart multi-material printing of organs, and tissue printing. Undoubtedly, 4D bioprinting technology will lead to the development of the orthopedic specialty “smart orthopedics,” which will revolutionize the management of spinal deformities, fracture fixation, joint injuries, cartilage constructs, knee replacements, and other related orthopedic applications.132,133 Unfortunately, we did not find in vitro, in vivo, or clinical research on 4D bioprinted constructs for tendon augmentation.
Challenges faced in translational tendon research and possible solutions
The first challenge of tendon TE is the lack of adequate translational research that enhances multidisciplinary collaboration among laboratory and clinical researchers and integrates the innovative desires of the general public (patients) to form high-quality medical practices. 134 Figure 2 describes the process of translational medicine in tendon research.

Process of translational research in tendon augmentation. T0 to T2 are the translational stages from basic science to human studies. T2 to T4 represent the translation of new data into clinic and health decision making.
Translational research can be divided into five levels (T0–T4), where T0 resembles the conceptual and basic research stage, T1 shapes and provides improved ideas from basic research through early investigations in humans, and T2 encompasses the creation of effective human and clinical guidelines. 134 Finally, T3 involves translating the research to practice, while T4 emphasizes outcomes and effectiveness analysis in populations.135,136
The challenges in the production of commercial products in TERM are stage related. First, the broad diversity of TERM as a research field presents an administrative challenge at translational stage T0 as some projects may require skills from various disciplines. This fundamental barrier feeds secondarily into problems encountered in laboratory studies, such as a lack of proper manipulation and appropriate acquisition of research material (cells, cell source, scaffold materials, nanoparticles, vectors, and bioreactors). 137 In vitro/in vivo studies (T0–T2) on cell therapy may indicate challenges in the lack of specific and reliable markers that can label tendon-derived stem cells (TDSCs) in vitro and tendon stem cells in situ, posing a problem in cell source identification, cell isolation procedures, and cell culture marker expression. This makes it difficult to fully understand the functions of TDSCs.138,139 The lack of sufficient human subjects willing to volunteer in clinical trials affects T1 to T3.
Although 3D bioprinted tendons are promising (T0–T1), considerable work is still expected both in vivo and in vitro. The technology faces challenges in bioprinting resolution, bioprinting speed (especially for vascular structures), and scaling up to large-scale cell-based therapies because of limited oxygen and nutrient supply to the innermost parts of the bioprinted structures and efficient waste product elimination. However, Ramos and Moroni believe that perfusable branched systems with smaller microvessels can help bypass this bottleneck. 113
Currently, 4D bioprinting is largely conceptual (T0) in general, and it is not yet widely applied in orthopedics. There are very few laboratory studies and clinical studies on 4D printing smart orthopedics worldwide. More orthopedic research is needed in this area at all levels. The number of in vitro/in vivo studies (T0–T4) on tendon augmentation is generally limited, and there are even fewer clinical trials, indicating the slow translation of research knowledge to therapeutic products and making the evaluation of available therapeutic options difficult.22,137 This situation is both caused by and results in ineffective therapeutics, mainly because the fundamental mechanisms that underlie the pathogenesis of tendon injuries and impaired healing are not well understood. 21 More research funding and interdisciplinary scientific collaborations are key in TERM research T0 to T4 translation.
Commercially available scaffolds products
Commercial products are the final output of tendon TERM research (T0–T4). The ultimate product quality determines market demand 14 and directly affects the research translation cycle (T0–T4) efficiency. Numerous biological and synthetic scaffolds have been developed and approved by various regulatory bodies globally, and a few studies have investigated their properties.14,140 In general, the mechanical and biocompatibility properties of commercially available products require improvements and new approaches, as discussed in the paper. Table 5 shows a list of the most widely used biologics that are commercially available for tendon scaffolds. Table 6 shows a list of the most widely used non-biologics that are commercially available for tendon scaffolds.
List of most widely used biologics commercially available for tendon scaffolds.

Food and Drug Administration (FDA), small intestinal submucosa (SIS), expanded polytetrafluoroethylene (ePTFE).
List of most widely used non-biologics commercially available for tendon scaffolds.

Poly-4-hydroxybut (P4HB), poly-l-lactic acid (PLLA), Food and Drug Administration (FDA).
Recommendations and future studies
The future of tendon augmentation in TE lies in the strong integration of various disciplines to translate ideas into research, followed by actual therapeutics. Although research is still limited in tendon augmentation, considerable work has been conducted on stem cell biology and functional scaffold materials. These two fields require more clinical trials to improve the available knowledge of current materials. The fields of nanotechnology and 3D/4D bioprinting are key to the future development of TE and tendons in particular 142 and require more attention.
Future researchers should focus more on combined approaches among cell therapy, growth factors, gene therapy, nanotechnology, and AM. A good example is Zhou et al., who used gene-modified sutures loaded with nanoparticles to form nanoparticle/plasmid complexes to promote tendon healing. The outcomes reported by Zhou et al. were superior tendon healing strengths, enhanced gliding function, and inhibited adhesion formation without adverse effects on host tissues. 73 In our review, we found limited research on 3D/4D bioprinting in orthopedics and very few studies on tendon augmentation. Therefore, the authors recommend that future studies should focus on applying 3D/4D bioprinting technologies in orthopedics, especially tendon augmentation, as they hold tremendous potential.
Conclusion
We are presented with an increasing global prevalence of tendon pathologies, especially among manual laborers, the sporting community, and the elderly. However, considerable improvements in techniques of tendon repair in the past decades have not led to clinically significant progress, partly because tendons are poorly perfused, heal slowly, and frequently form scar tissue. These and other factors have led to a high failure rate of treatments, joint stiffness, morbidity, and cost burden for patients. The current tendon TE scaffolds (synthetic, biologic, or composites) on the market are static and non-animating, lacking the time-dependent dimensions and failing to mimic the dynamic tissue environment and biomechanical forces required to promote optimal tenogenic differentiation for endogenous repair and regeneration. In the future, new strategies, such as 3D/4D bioprinting, may provide a rapid and promising solution for the production of smart tendon/ligament scaffolds with self in vivo regulation in response to stimuli, animating ability, and self-healing. This would lead to the development of smart orthopedics. This narrative review reported some successful laboratory studies on cell therapy, scaffolds, 3D/4D bioprinting, gene therapy, cell signals, or their combination. To successfully develop more tendon augmentation therapies via TERM approaches, further research and clinical trial investigations are needed.
Footnotes
Author contributions
RM conceptualized and planned the article and contributed to the writing of the manuscript. MHN, MMT, and LOZ contributed, reviewed, and edited the manuscript. JDW contributed, reviewed, and revised the final work. All the authors read and approved the final version.
Declaration of conflicting interest
The authors declare that they have no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.