
Abstract
Objective
Intracorporeal esophagojejunostomy remains a challenging technique in totally laparoscopic total gastrectomy (TLTG) because of the lack of an established standard anastomosis method. However, π-shaped esophagojejunostomy in TLTG is reportedly safe and feasible. Therefore, we evaluated the short-term surgical outcomes of our modified π-shaped esophagojejunostomy in TLTG.
Methods
This study involved patients without neoadjuvant therapy diagnosed with gastric cancer who underwent TLTG by the same surgeon with modified π-shaped esophagojejunostomy from April 2018 to October 2019. Clinicopathologic data were collected and retrospectively analyzed.
Results
Forty patients diagnosed with gastric cancer were included. The mean operative time and estimated blood loss were 264.6 ± 56.9 minutes and 68.5 ± 53.3 mL, respectively. Postoperative flatus occurred at 4.6 ± 1.7 days. The mean time to resumption of diet was 7.4 ± 1.7 days postoperatively. One patient was diagnosed with anastomotic leakage and managed with conservative therapy. Pleural effusion was the most common complication, occurring in four (10%) patients. One patient developed intra-abdominal bleeding that required reoperation. Other complications were atrial fibrillation and wound infection. No mortality occurred during the 6-month follow-up.
Conclusions
Modified π-shaped esophagojejunostomy is safe and feasible for intracorporeal anastomosis in TLTG and showed favorable surgical outcomes in this study.
Keywords
Introduction
Intracorporeal anastomosis during laparoscopic gastrectomy has been increasingly performed in recent years.1,2 Compared with extracorporeal anastomosis, intracorporeal anastomosis has the advantages of not only reduced postoperative pain, fewer wound complications, and a smaller incision but also better visualization of the operative field during the procedure. 3 However, intracorporeal esophagojejunostomy in totally laparoscopic total gastrectomy (TLTG) is still considered technically challenging. Anastomosis with a circular stapler that resembles conventional open gastrectomy is associated with advanced technical demands in complex purse-string suture and anvil placement during laparoscopic procedures, although various methods have been introduced.4,5 In contrast, a linear stapler has been proven to be more user-friendly, with favorable clinical outcomes in terms of safety and feasibility. 6 However, a standard anastomotic method for esophagojejunostomy during TLTG using linear staplers has not yet been established. Kwon et al. 7 first reported π-shaped esophagojejunostomy, a simple procedure even for inexperienced surgeons. This method provides adequate operative visualization and avoids incomplete stapling while closing the common opening, which is considered the most challenging procedure in laparoscopic anastomosis. Zhang et al. 8 described 11 patients who underwent robotic total gastrectomy with π-shaped esophagojejunostomy and achieved satisfying short-term clinical outcomes. However, evidence regarding the safety and feasibility of this novel approach is still limited.
The present study was performed to analyze consecutive patients who underwent TLTG with modified π- shaped esophagojejunostomy and to demonstrate that modified π-shaped esophagojejunostomy is a safe and feasible approach in TLTG.
Methods
Patients
All patients in this study had histologically confirmed gastric cancer in the mid or upper stomach. All surgeries were performed by one surgeon. Written informed consent was obtained from all patients before participation, and the data collection and analysis were approved by the Medical Ethics Committee of Peking University Cancer Hospital (approval no. 2020KT61). The following demographic and clinicopathologic data were collected: age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) score, tumor size, tumor location, depth of tumor invasion, number of harvested lymph nodes, nodal metastasis and TNM stage, operative time, estimated blood loss, time to resumption of diet, postoperative hospital stay, complications, and mortality. All patients were followed up in the outpatient department at 1, 3, and 6 months postoperatively. The median follow-up time was 21.57 ± 4.46 months. The reporting of this study conforms to the STROBE guidelines. 9
Surgical techniques
The patients were placed in the supine position with legs apart. The operator stood on the left side of the patient, the assistant stood opposite the operator, and the cameraman stood between the patient’s legs. A 10-mm camera port was introduced 2 cm below the umbilicus using the Veress needle technique or open technique. The carbon dioxide pressure was increased to 13 mmHg, and four ports other were then introduced: a 10-mm trocar was inserted in the left anterior axillary line, 2 to 3 cm below the costal margin, as the major operation port; a 5-mm trocar was inserted contralaterally as the main assistant port; and two 5-mm trocars were inserted in the right and left midclavicular lines at the umbilical level as the accessory ports. A Nathanson liver retractor was placed for liver traction.
Gastric mobilization and lymph node dissection were performed laparoscopically in accordance with the Japanese gastric cancer treatment guidelines. The abdominal esophagus was fully mobilized for anastomosis (Figure 1). The duodenum was intracorporeally transected 2 cm distal to the pylorus using a 60-mm linear stapler. The jejunal mesentery 50 cm distal to the ligament of Treitz was adequately divided to avoid possible tension during esophagojejunostomy. The esophagogastric junction was constricted by a nylon band to prevent gastric content spillage and subsequently retracted downward by the assistant. A small incision was made on the right side of the abdominal esophagus. An enterotomy was created on the antimesenteric side of the jejunum 50 cm distal to the ligament of Treitz, and the cartridge fork of the stapler was inserted in the distal direction. The anvil fork of the stapler was then introduced into the incision in the abdominal esophagus with the guidance of a nasogastric tube inserted by the circulating nurse. The stapler was maneuvered to construct a side-to-side esophagojejunostomy in an antecolic fashion (Figure 2). The mucosal-side hemorrhage of the anastomosis was examined through the common opening. A 60-mm stapler was inserted via the previously made division on the jejunal mesentery. After ensuring that both the anterior and posterior sides of the common opening were completely served, the common opening closure, esophageal division, and jejunal division were completed in one stapling procedure (Figure 3). An additional stapling or clipping procedure was required in some patients. Continuous sutures were added at this stapling line for reinforcement because of the existence of overlapping staples, and the esophagojejunostomy was thus completed (Figure 4).

The abdominal esophagus was adequately detached from the surrounding tissues for esophagojejunostomy.

A side-to-side esophagojejunostomy was formed using a 60-mm stapler.

The common opening was closed using a linear stapler, and the division of the esophagus and jejunum was completed during the same stapling procedure.

The actual anastomosis after esophagojejunostomy.
A previously formed entry hole and a small segment of the proximal jejunum were transected, and the specimen was extracted via the small laparotomy. A side-to-side jejunojejunostomy between the proximal jejunal limb and a site on the jejunum 50 cm distal to the esophagojejunostomy was made. The common opening of the jejunojejunostomy was then closed using a 60-mm stapler.
Results
This retrospective study involved 40 patients with gastric cancer who underwent TLTG with modified π-shaped esophagojejunostomy in our department from April 2018 to October 2019. The clinicopathological data of all patients are shown in Table 1. The patients comprised 24 men and 16 women with a median age and BMI of 63 years and 22.8 kg/m2, respectively. Most patients had a preoperative ASA score of 2, followed by an ASA score of 1. The mean tumor size and number of harvested lymph nodes was 3.5 ± 1.5 cm and 30.5, respectively. In total, 28 (70%) patients were diagnosed with cancer in the middle third of the stomach, and 12 (30%) were diagnosed with cancer in the upper third of the stomach. The tumors invaded the mucosal layer in 13 (32.5%) patients, submucosal layer in 5 (12.5%), proper muscle in 11 (27.5%), and serosa in 11 (27.5%). Twenty (50%) patients were pathologically diagnosed with no nodal metastasis; this was the most common finding. TNM stage I was the most common (37.5%), followed by stage II (35.0%) and stage III (27.5%).
Clinicopathological characteristics of all patients.
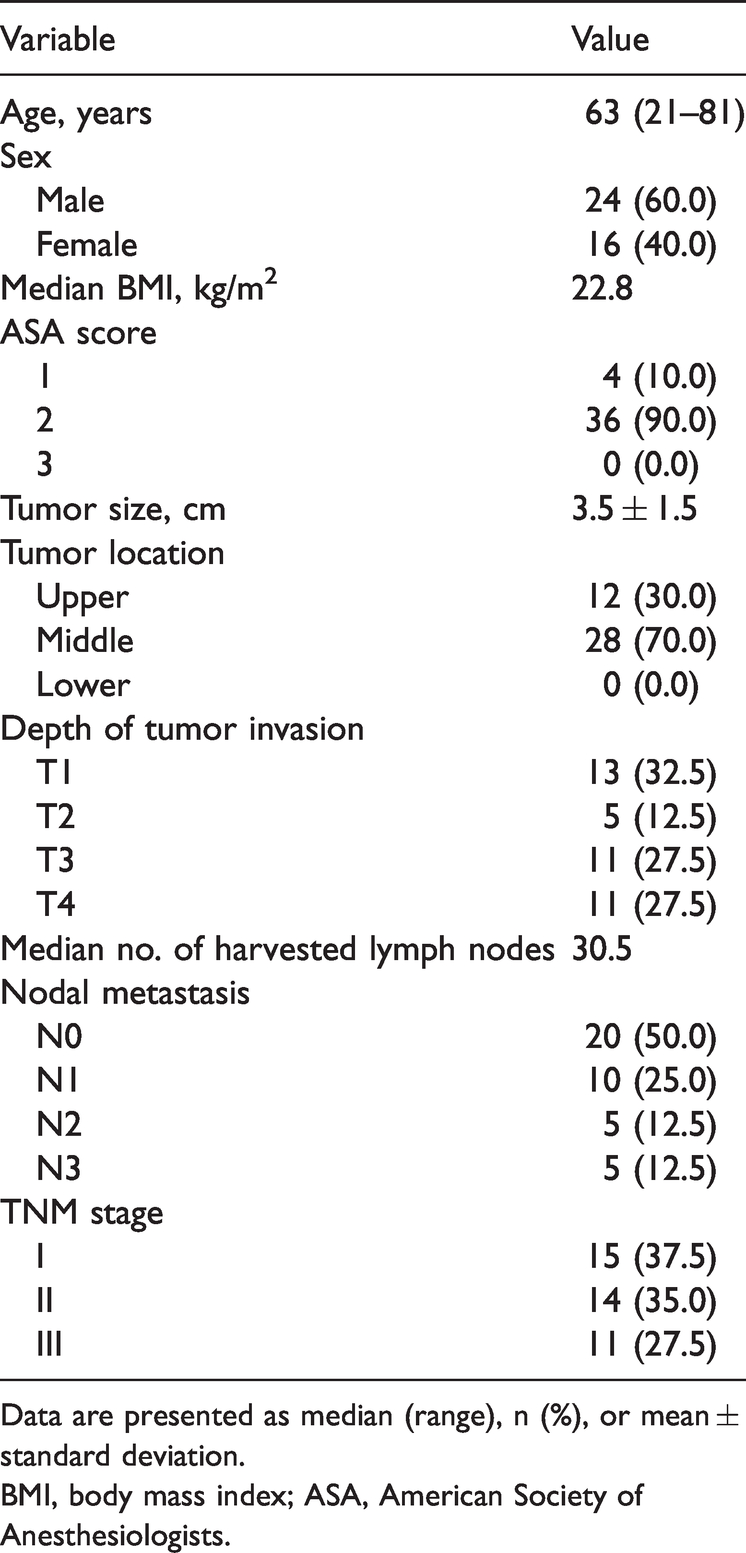
Data are presented as median (range), n (%), or mean ± standard deviation.
BMI, body mass index; ASA, American Society of Anesthesiologists.
The patients’ surgical outcomes are summarized in Table 2. The mean operative time and estimated blood loss were 264.6 ± 56.9 minutes and 68.5 ± 53.3 mL, respectively. Postoperative flatus occurred at a mean of 4.6 ± 1.7 days. The mean time to resumption of diet was 7.4 ± 1.7 days postoperatively. The mean postoperative hospital stay was 9.0 ± 1.3 days. One patient had anastomotic leakage of the esophagojejunostomy diagnosed by upper gastrointestinal radiography. The patient was asymptomatic and managed with conservative therapy. Pleural effusion, observed in four (10%) patients, was the most common postoperative complication. One patient had intra-abdominal bleeding (bleeding in the inferior pole of the spleen) that required reoperation. Other complications were atrial fibrillation and wound infection. No anastomotic stricture was observed on postoperative radiography. No patient died during the 6-month follow-up.
Surgical outcomes of all patients.

Data are presented as mean ± standard deviation or n (%).
Discussion
TLTG has become widely performed in recent years because of advantages such as a wide visual field, short operation time, and short hospital stay.10–12 During the TLTG procedure, meticulous performance of esophagojejunostomy is very important because complications may result in a high morbidity rate and poor prognosis. 13 In this study, modified π-shaped esophagojejunostomy was used to complete the TLTG procedure, and esophagojejunal anastomosis-related complications occurred in 2.5% of patients. This rate is comparable to that in previously published studies,10,14,15 indicating the safety of this procedure.
In esophagojejunostomy using a linear stapler, the two major approaches are the overlap method and the functional method.16,17 Several studies have shown that the incidence of esophagojejunal anastomotic complications ranges from 0.00% to 6.45% when using the functional method,18,19 whereas few reports have described the use of the overlap method.20,21 From our perspective, modified π-shaped anastomosis, an alternative form of the functional method, has three main theoretical advantages. First, after closing the common entry using a linear stapler, several additional sutures are added at the staple line to prevent minor bleeding and potential leakage due to overlapping staples. Second, the jejunal mesentery 50 cm distal to the ligament of Treitz is adequately divided to prevent tension during esophagojejunostomy, thus avoiding anastomotic stricture. Third, adequate mesentery division can also ensure tension-free anastomosis, helping to prevent leakage in modified π-shaped anastomosis.
The mean operative time in the present study was 264.6 ± 56.9 minutes. This duration was slightly longer than that in previously published studies,14,22,23 mainly because dividing the jejunal mesentery is time-consuming. However, the estimated blood loss, postoperative flatus, and postoperative hospital stay were all comparable to those in the above-mentioned previous studies, indicating that this approach is feasible. Anastomotic stenosis is a common complication in esophagojejunal anastomosis, especially when using a circular stapler. 24 In our modified π-shaped anastomosis, a 60-mm linear stapler was used for both the anastomosis and common entry hole closure, as in the traditional π-shaped anastomosis. 7 This procedure can maximally prevent stenosis; indeed, we found no stenosis in the postoperative radiographic examination of our study. Several studies have also shown that the surgeon’s experience is an important factor in the incidence of complications.25–27 In the present study, only one well-experienced surgeon with a similar surgical team performed the surgeries for all 40 patients. This quality control may have contributed to the low incidence of complications, especially esophagojejunal anastomotic complications. We therefore recommend that the surgeon and surgical team who perform this approach are highly experienced. However, this approach also has some drawbacks. First, the division of the jejunal mesentery in some patients with a high BMI is difficult and inefficient. Second, jejunal mesenteric division may result in an inadequate blood supply at the proximal part of the division area (i.e., the anastomotic site in the next step). Injection of indocyanine green to examine the blood supply in the jejunal loop may help prevent this situation.28,29
This study has inherent limitations associated with its retrospective, small-volume, and single-arm design. Well-designed studies are needed to confirm the application of this approach in TLTG.
Conclusions
Modified π-shaped esophagojejunostomy is safe and feasible for intracorporeal anastomosis in TLTG with favorable short-term clinical outcomes.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (Nos. 82171720, 81872022, 81672439), Beijing Natural Science Foundation (No. 7162039), Capital’s Funds for Health Improvement and Research (CFH 2018-2-2153), Beijing Hospitals Authority Clinical Medicine Development of Special Funding Support (No. ZYLX202116), Beijing Municipal Administration of Hospitals Incubating Program (No. PX 2016018), and Beijing Excellent Talent Training Funding (2018000021469G258).