
Abstract
Objective
To assess the association between post-balloon angioplasty dissection and the mid-term results of the AcoArt I trial evaluating complex femoropopliteal artery disease.
Methods
The outcome data for 144 patients from the AcoArt 1 trial were reanalysed. These patients were randomly divided into percutaneous transluminal angioplasty (PTA) and drug-coated balloons (DCB) groups. The primary endpoint was the primary patency (PP) rate and clinically-driven target lesion revascularisation at 24 months.
Results
After 24 months of follow-up, the PP rate of dissection cases in the PTA group was lower vs non-dissection cases. In patients receiving a bailout stent for dissection, the PP rate in the PTA group was lower vs the DCB group. Cox regression analysis showed that dissection decreased the PP rate; mild dissection reduced the PP rate as follows: 52%, PTA group and 19%, DCB group. With severe dissection, the PP rate reduction was as follows: 75%, PTA group and 73%, DCB group.
Conclusions
The mid-term follow-up showed that post-balloon angioplasty dissection reduced the PP rate in the PTA group but not in the DCB group. Additionally, in patients receiving a bailout stent for dissection, the DCB group had a better PP rate than the PTA group.
Keywords
Introduction
Although dissection events after uncoated balloon percutaneous transluminal angioplasty (PTA) are common, reports of the results are incomplete, especially regarding the increased use of drug-coated balloons (DCBs) in recent years.1–4
In accordance with our previous study,5,6 we performed a sub-analysis to evaluate the outcome of dissections following different treatments for femoropopliteal arterial disease. A comparison was also performed between the PTA group and DCB group with and without dissection. This study aimed to further investigate the effect of post-balloon angioplasty dissection on primary patency (PP) in a DCB clinical trial evaluating complex femoropopliteal artery disease.
Methods
Ethics statement
This trial was performed according to the requirements of the Helsinki Declaration. The medical device used in the trial complies with the regulations of the China Food and Drug Administration. This study was approved by the Chinese PLA General Hospital Ethics Committee and the local ethics committees of participating hospitals. The approval numbers are as follows: 1. Chinese PLA General Hospital, Beijing, China approval number: (2013), Ethical approval No. (0112). 2. Renji Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China, approval number: RenJi, Ethical approval [2013] No. 77. 3. Xiyuan Hospital, China Academy of Chinese Medical Sciences, Beijing, China, approval number: 2013XL021-2. 4. Zhongshan Hospital Fudan University, Shanghai, China, approval number: 2013-35. 5. The People’s Hospital of Liaoning Province, Shenyang, China. No approval number, (approval date: 2013-06-13). 6. The First Affiliated Hospital of Dalian Medical University, Dalian, China, approval number: LCSY2013-05. 7. The First Affiliated Hospital of Chongqing Medical University, Chongqing, China, approval number: ethical approval No. (26-2) in 2013. 8. The First Affiliated Hospital of Fujian Medical University, Fuzhou, China, approval number: Ethical Medicine/Equipment Approval [2013] No. 11. 9. The Second Hospital of Hebei Medical University, Shijiazhuang, China, approval number: 2013EC08-06-1. 10. The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, China, approval number: Ethical Quick Approval (Mechanical) [2013] No. 02.
Patients were informed of the purpose, treatment methods, and possible results, and provided written consent. The patients had the right to withdraw their consent at any time. For related information, please refer to reference 5.
AcoArt I trial interim results, patients, and post-hoc analysis of dissection
The AcoArt I trial was a prospective, multicentre, randomised, controlled study of local paclitaxel for preventing femoropopliteal artery restenosis. The study was registered on the National Institutes of Health website (ClinicalTrials.gov; identifier: NCT01850056). A total of 200 patients were randomly recruited into the study from 10 clinical centres. Patients had an average age of 66 years and 74% were men, with 100 patients in the PTA group and 100 patients in the DCB group. The continuous change in a single lesion from one leg was selected as the subject of study. Mean lesion length in the DCB and PTA groups was 147 ± 110 mm and 152 ± 109 mm, respectively, and the proportion of total occlusions was 57% and 52%, respectively. The rate of bailout stent implantation in the DCB and PTA groups was 19% and 21%, respectively. Mean late lumen loss (LLL) in the DCB and PTA groups was 0.05 ± 0.73 and 1.15 ± 0.89 (p < 0.001), respectively, at 6 months. One year later, target lesion revascularisation rates were 7.2% and 39.6%, respectively (p < 0.001). At the 24-month follow-up, the PP rate in the DCB group was still higher than in the PTA group (64.6% vs. 31.4%, respectively; p < 0.001). The rate of freedom from clinically-driven target lesion revascularisation (CD-TLR) was higher in the DCB group than in the PTA group (86.5% vs. 58.9%, respectively; p < 0.001). A more detailed description of the results was published previously.5,6
Fifty patients underwent treatment for in-stent restenosis; three patients received a bailout stent for residual stenosis. Two of the three patients received a non-assigned uncoated balloon, and one patient died shortly after the 6-month angiographic control. These three patients were excluded from the current study; therefore, 144 patients were finally enrolled, comprising 86 with post-balloon angioplasty dissection, 27 without dissection and 31 with a stent implantation for dissection (Figure 1). All patients underwent imaging follow-up at 6, 12, and 24 months. Angiography was performed at the 6-month follow-up, while at the 12- and 24-month follow-ups, a trained physician performed ultrasonography.

Patient flow diagram. Two deaths occurred within 6 months.
Dissection analysis
The current study design took the following into account: the anatomical structure of leg arteries differs from that of coronary arteries, with longer lesions in the leg arteries and the possibility of multiple post-angioplasty dissections. The current study evaluated dissections of the highest grade, only; therefore, dissections of only one type were recorded for each patient. Furthermore, there were no type F dissections in this study because all affected patients had been treated with a bailout stent. Finally, because of the limited number of patients, type A/B/C dissections were classified as mild, whereas type D/E dissections were labelled severe.
Endpoints
At 12 and 24 months, the primary endpoint was the PP and CD-TLR rates, where PP was defined as freedom from CD-TLR, and restenosis, determined by a Doppler ultrasonography peak systolic velocity ratio ≥2.4. The secondary endpoints were the following clinical variables: improvement in the Rutherford class and the ankle–brachial index (ABI) of the target leg.
Statistical analysis
Continuous variables are shown as means (standard deviations) for continuous variables, and categorical variables are shown as numbers and proportions. The Mann–Whitney and chi-square tests were used to determine any significant difference between the means and proportions in the two groups. The PP rate was assessed as the time-to-event outcome with Kaplan–Meier curves, and a log-rank test was used to compare the differences between the groups.
Cox proportional hazards models were used to identify associations between dissection, dissection grade, and PP. The results are presented as hazard ratios (HRs) and 95% confidence intervals (CIs). A two-tailed p value of < 0.05 was considered statistically significant in all of the analyses, which were performed with the statistical software packages R (www.r-project.org) and Empower Stats (http://www.empowerstats.com; X&Y Solutions, Inc., Boston, MA, USA).
Results
Baseline demographic and lesion characteristics
There were significant differences (p < 0.05) only for the reference vessel diameter between patients with dissection in the DCB and the PTA groups. Additionally, there were no significant differences between patients without dissection in the DCB group and the PTA group, except for minimal luminal diameter. There were no significant differences between the DCB and PTA groups in baseline characteristics in patients receiving a bailout stent for dissection (Table 1).
Patients’ demographic data and baseline lesion characteristics.
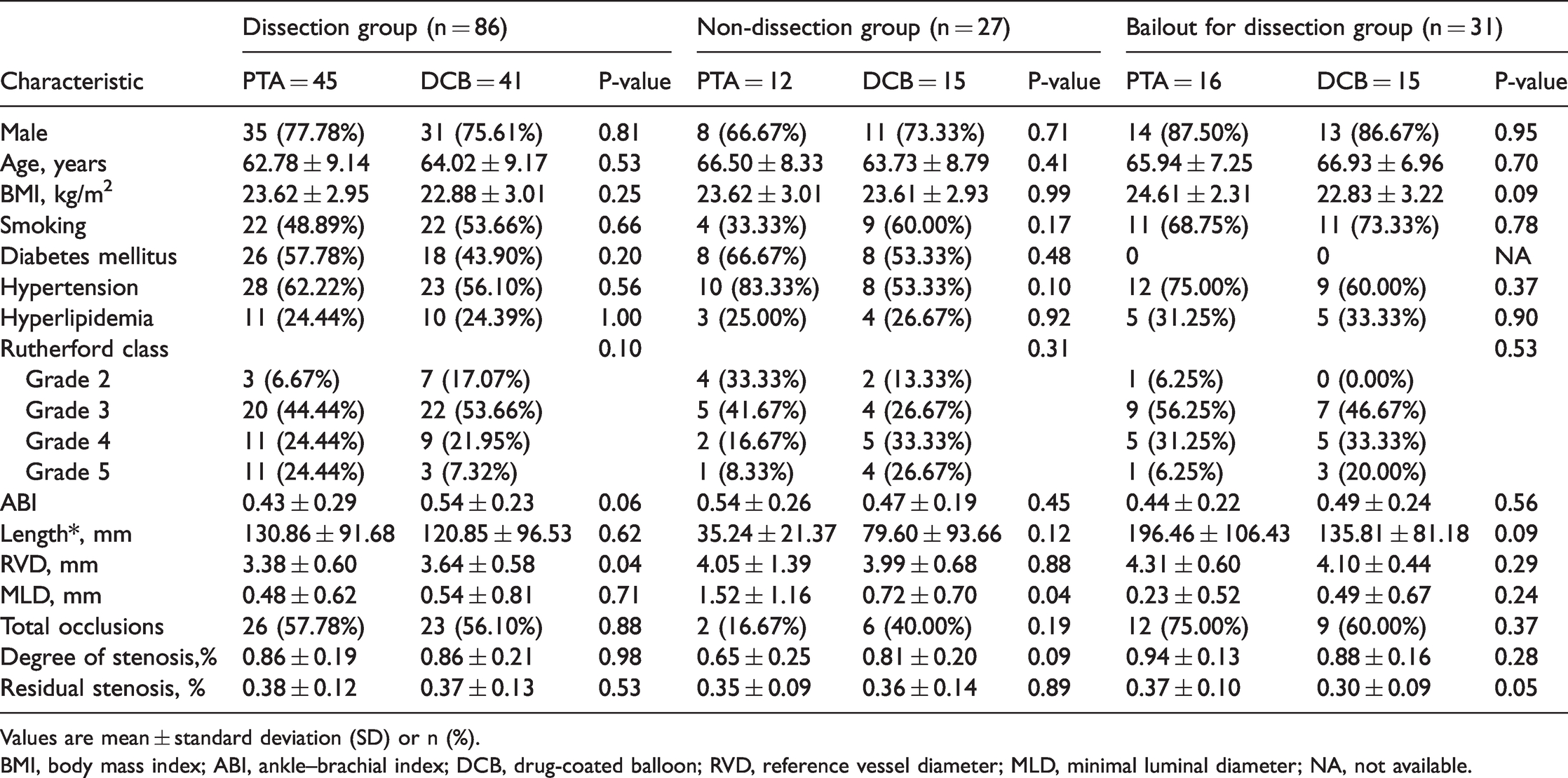
Values are mean ± standard deviation (SD) or n (%).
BMI, body mass index; ABI, ankle–brachial index; DCB, drug-coated balloon; RVD, reference vessel diameter; MLD, minimal luminal diameter; NA, not available.
Interventional outcomes during different follow-up periods for patients with and without dissection
In patients undergoing stent implantation to save the lumen, compared with the PTA group, the PP rate in the DCB group was much better (33.3% vs 84.6%, respectively; p = 0.006), and the CD-TLR rate was only 6.7% in the DCB group vs. 37.5% (p = 0.04) in the PTA group at the 2-year follow-up (Table 2).
Comparison of effective outcomes during the 24-month follow-up of patients with and without dissection.
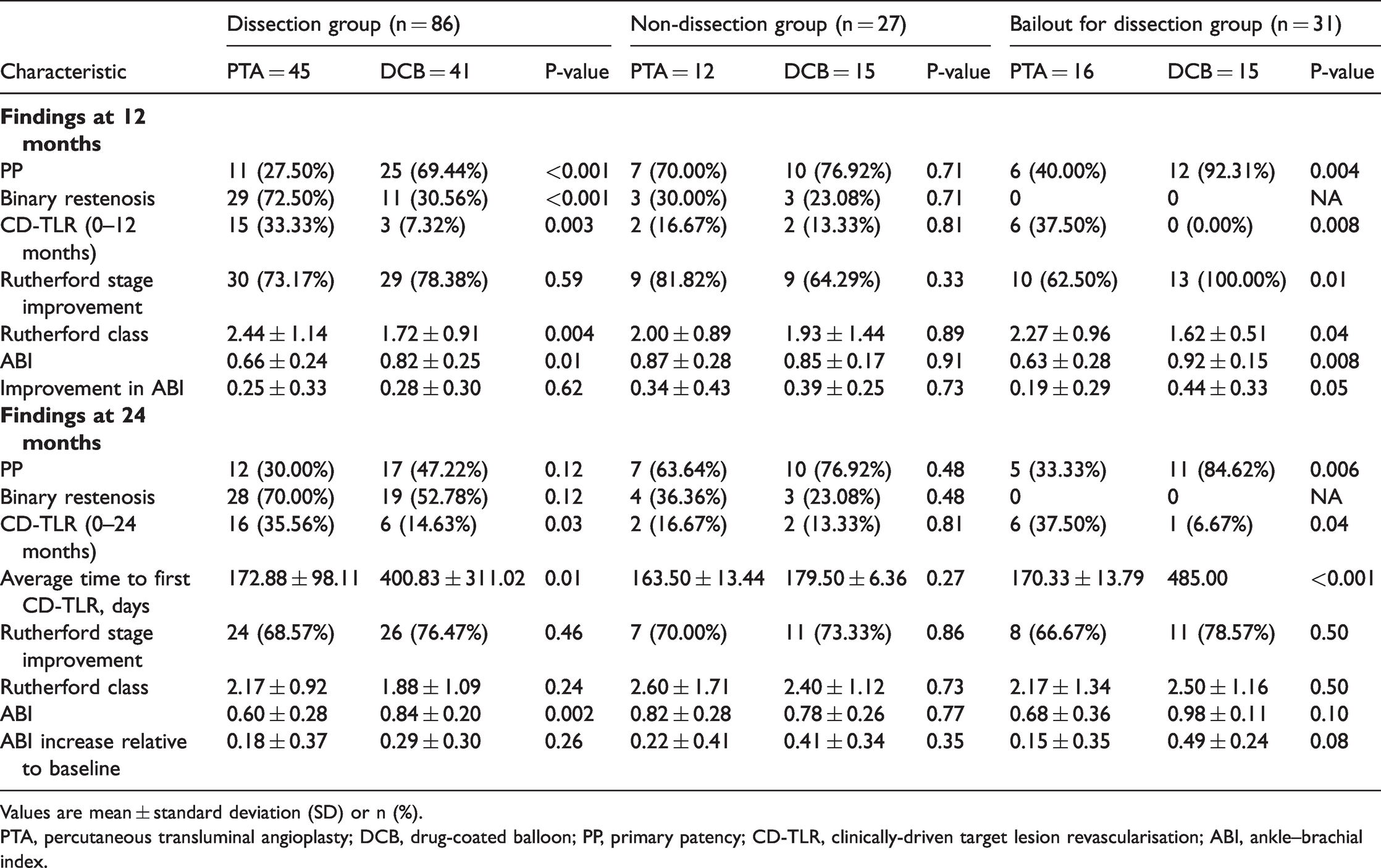
Values are mean ± standard deviation (SD) or n (%).
PTA, percutaneous transluminal angioplasty; DCB, drug-coated balloon; PP, primary patency; CD-TLR, clinically-driven target lesion revascularisation; ABI, ankle–brachial index.
The PP rate was higher for those treated with DCB than those treated with PTA in the dissection group, although the rate was not statistically significant at 24 months. Freedom from CD-TLR indicated better outcomes for DCB patients vs PTA receiving dissection treatment. In addition, the average time to first CD-TLR (days) treatment was significantly longer for the DCB group than the PTA group. A comparison of DCB and PTA patients without dissection treatment showed no statistical differences in clinical outcomes up to the 24-month follow-up. Similarly, patients receiving a bailout stent for dissection in the DCB group had better results compared with the PTA group (Table 2).
Interventional outcomes during different follow-up periods for patients receiving the different treatments
Compared with the non-dissection cases, the PP rate decreased in patients with dissection in the DCB group, but the difference was not statistically significant until the 2-year follow-up. However, compared with the non-dissection cases, the PP rate in patients with dissection in the PTA group decreased significantly at the end of the 2-year follow-up. In addition, in the DCB group, the improvement in ABI remained high regardless of whether patients developed post-treatment dissection, and there was no significant difference between the groups. However, compared with the non-dissection cases in the PTA group, the ABI of dissection cases decreased significantly, and this trend continued during the 2 years of follow-up (Table 3).
Comparison of effective outcomes during the 24-month follow-up in patients receiving DCB vs PTA.

Values are mean ± standard deviation (SD) or n (%).
DCB, drug-coated balloon; PTA, percutaneous transluminal angioplasty; PP, primary patency; CD-TLR, clinically-driven target lesion revascularisation; ABI, ankle–brachial index.
The relationship between dissection and PP
The incidence of dissection in this study was 79.7%. Univariate Cox regression analysis showed a significant association between dissection and the risk of a low PP rate in the PTA group. The PP rate during the 24-month follow-up period was significantly lower in patients with dissection than in patients without dissection (HR = 0.35; 95 CI%: 0.12–1.01; p = 0.05). In the DCB group, the PP rate in dissection cases was lower than that in non-dissection cases, but the difference was not statistically significant (HR = 0.41; 95% CI: 0.12–1.83). Although mild dissection (type A/B/C) reduced the PP rate, this decrease was not significant compared with non-dissection cases in either group. However, severe dissection (type D/E) reduced the PP rate by more than 70% in both the PTA and DCB groups (Table 4). The Kaplan–Meier analysis (Figure 2) examined the clinical outcomes of PP up to 2 years, including a comparison of the DCB group and PTA group in cases with dissection and a comparison of dissection cases with non-dissection cases in the PTA group. Finally, we compared patients with or without post-balloon angioplasty dissection in the DCB group.
HRs (95% CIs) for dissection regarding primary patency over a 24-month period.

The type of dissection was in accordance with the National Heart, Lung, and Blood Institute (NHLBI) classification system. 13
The model was adjusted for age, sex, reference vessel diameter at baseline and minimal luminal diameter at baseline.
PTA, percutaneous transluminal angioplasty; DCB, drug-coated balloon; HR, hazard ratio; CI, confidence interval; ref, reference.

Kaplan–Meier curves for primary patency. a. Kaplan–Meier curves of primary patency at 24 months for the PTA and DCB groups of patients with dissection. b. Kaplan–Meier curves of primary patency at 24 months for cases with and without dissection in the PTA group. c. Kaplan–Meier curves of primary patency at 24 months for cases with and without dissection in the DCB group. d. Kaplan–Meier curves of primary patency in patients without dissection in the DCB and PTA groups.
Discussion
The advantages of DCB in post-balloon angioplasty dissection
The incidence of dissection in this study was 79.7%. In several recent large-scale DCB trials, the incidence of dissection was 56% in the THUNDER 3 trial, 30% in the FemPac study 7 and 47.4% with DCB vs 73.5% with PTA (p = 0.03) in the PACIFIER trial. 4 The high dissection rate in our study was associated with longer lesions and higher occlusion rates. In most cases, the guidewire passage is intraluminal in lesions; balloon angioplasty increases the diameter of the vessel lumen, but it inevitably produces high numbers of non-flow-limiting dissections. This traumatic mechanism inevitably leads to an inflammatory response and medial necrosis; therefore, local drug therapy is a reasonable choice. However, in cases of subintimal passage, it is still not completely clear whether DCBs are as efficient intraluminally as subintimally. 8 Owing to the high proportion of complex femoropopliteal artery disease in the selected cases in this study, there were a number of cases of passage under the intima, and post-balloon angioplasty flow-limiting dissections were also produced. Therefore, the proportion of bailout stents in this study was higher than that in previous reports.
The advantage of DCB regarding a bailout stent for dissection
Stent placement is often used to secure dissections; however, not all dissections require a bailout stent, and this issue has been discussed in previous articles.9–11 There is no clear conclusion regarding the results after implanting a stent for flow-limiting dissection in the two groups (PTA and DCB). Patency in the lumen is generally believed to be obtained immediately after stent implantation, but restenosis still occurs because of the long-term inflammatory effect and intramural stress injury caused by the foreign body reaction. It has been established that neointimal hyperplasia is an excessive healing response to mechanical damage to the arterial wall; larger stent-to-reference vessel diameter ratios result in more obvious intimal hyperplasia. 12 Therefore, although a bailout stent for dissection saves the lumen, it also results in late restenosis. Our study indicated that DCBs inhibit neointimal proliferation. In patients undergoing stent implantation to save the lumen, compared with the PTA group, the PP rate in the DCB group was much better, and the CD-TLR rate was also much lower (6.7% in the DCB group vs. 37.5% (p = 0.04) in the PTA group) at the 2-year follow-up.
Study limitations
This study has certain limitations. First, the AcoArt I trial was the first clinical study in China to examine DCB therapy for femoropopliteal artery disease. Ten institutes participated in this study, and sampling error was avoided. However, inconsistencies in managing dissection with bailout stenting were likely because of differences between physicians in identifying dissection severity. Second, because the appearance of a DCB differs significantly from the appearance of an uncoated balloon, the surgeon inevitably knows the patient’s treatment, and this lack of blinding may have affected the dissection treatment. Third, the dissection classification method used in this study may be more appropriate for angiographically visible dissections because intravascular ultrasonography may be more accurate for determining dissection severity. Therefore, a comparative study of post-balloon angioplasty dissection of femoropopliteal artery disease using angiography and intravascular ultrasonography is required.
Conclusions
In this trial concerning complex femoropopliteal artery disease in the Chinese population, there was no statistical difference between the DCB group and the PTA group regarding the PP rate of patients without dissection after 2 years. However, in patients with dissection and a bailout stent for dissection, the PP rate in the DCB group was still significantly superior to that in the PTA group at 24 months. The PP rate decreased in a stepwise manner with an increase in the dissection level, and when a D-type and above dissection is present, a DCB is recommended even for bailout stent treatment.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Acknowledgments
We thank the participating patients and their families, who made the trial possible. We also thank all of the AcoArt I investigators.