
Abstract
In patients with intermittent claudication and long chronic total occlusions of the superficial femoral artery, a primary surgical bypass or stenting is recommended. However, due to the invasive nature, high complication rates and patient-related comorbidities, surgery is currently not the preferred method and full lesion stenting for long chronic total occlusions has the obvious consequences of permanent metallic implants. We report a case of a patient with a long chronic total occlusion of the superficial femoral artery with intermittent claudication. Endorsing an endovascular-first strategy, he was treated via an antegrade and retrograde approach with a complete recanalization and a stentless treatment with rotational atherectomy and drug-coated balloons. We believe this is a feasible endovascular strategy for the treatment of long chronic total occlusions of the superficial femoral artery for patients refusing open surgery. Further investigations are needed to evaluate long-term clinical outcomes of these novel techniques.
Introduction
Peripheral artery disease (PAD) affects about 27 million people only in Europe and North America. In the majority of patients, the superficial femoral artery (SFA) is frequently affected. Current European Society of Cardiology (ESC) PAD guidelines recommend an endovascular approach for initial treatment of short femoral–popliteal lesions in patients with intermittent claudication despite optimal medical and exercise therapy. 1 Stenting is considered the first choice but is not recommended for longer lesions due to an increased risk of stent occlusions.2,3 Therefore, a surgical bypass using the great saphenous vein is recommended for femoro–popliteal occlusions of more than 25 cm for patients eligible for surgery. 1 Many patients, however, refuse this approach due to longer hospital stays, the invasiveness and high complication rates. In contrast to the ESC guidelines, current American Heart Association/American College of Cardiology (AHA/ACC) recommendations do not define specific criteria regarding endovascular versus open surgery for longer lesions. 4 Data regarding novel treatment modalities for patients refusing open surgery remain scarce.
Case
A 70-year-old male with known PAD presented with claudication of the lower right leg (Rutherford 3). Preinterventional ultrasound revealed a complete atherosclerotic occlusion of the SFA with compromised ankle-brachial index (ABI) of 0.64 of the right leg. The patient refused open surgery and thus an endovascular approach was chosen. Angiography revealed a long chronic total occlusion (CTO, TASC D) of the SFA (Figure 1(a)), notably without proximal stump. Interventional attempts to cross the occlusion via an antegrade access through contralateral common femoral artery (CFA) remained without success using a support catheter (Navicross; Terumo) and a 0.18 wire (V18; Boston Scientific) (Figure 1(b)). Thus, a retrograde approach via the anterior tibial artery was elected and performed with a micropuncture set (Micropuncture Pedal Introducer; Cook Medical) under ultrasound guidance with the patient in supine position. Using a 0.18 support catheter (SureCross; Merit Medical) and a hydrophilic 0.18 wire (Glidewire; Terumo) recanalization succeeded with guide wire entry in the CFA (Figure 1(c)) and externalized to the left CFA. The CTO was then treated through the antegrade approach using a filterless rotational atherectomy device (Rotarexs; Straub Medical) due to severe calcifications (PACSS 4c) and multiple dilations of the entire SFA (3*120 and 4*120; Admiral Medtronic, 180-s inflation time each). Final angiography showed only minor non-limiting dissections and thus a stent-free approach with drug-coated balloons (DCB, 4*120 Passeo-Lux; Biotronik) was elected, concerning the length of the lesion and the immediate proximity to the CFA (Figure 1(d)). Ultrasound, perfusion and clinical examination at 6-months follow-up after the initial procedure revealed a complete recanalization of the SFA and improved claudication symptoms (Rutherford 2, Figures 1(e) and (f) and 2).
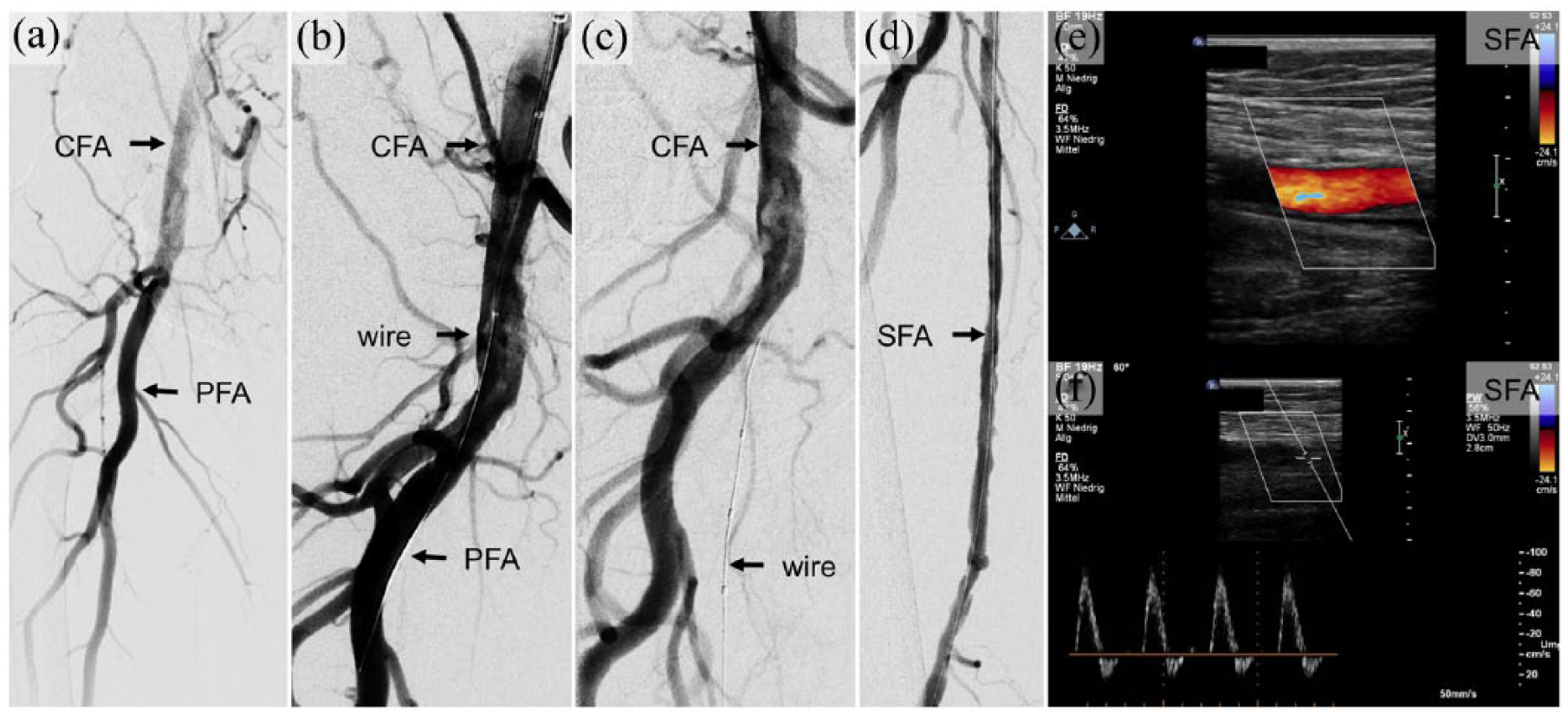
Digital subtraction angiography (DSA) and duplex ultrasound (DUS) images of the right SFA. (a) DSA confirmed an occlusion of more than 25 cm of the right SFA. (b) Attempts to cross the occlusion via an antegrade access remained without any success. (c) Therefore, a retrograde access via the anterior tibial artery was chosen and a wire was brought across the occlusion. The recanalization was performed using a rotational atherectomy device and DCBs without concomitant stent implantation. (d) Final angiography with complete revascularization of the SFA. (e, f) Doppler ultrasound performed at 3 months after the initial procedure confirmed a complete recanalization of the right SFA without evidence of a remaining stenosis.

Ankle-brachial index (ABI) and pain-free walking distance (WD) showed marked improvement with diminished claudication symptoms.
Discussion
Endovascular treatment of PAD has gained widespread acceptance is the first-line treatment in many clinical scenarios as the primary revascularization strategy. 5 However, a primary surgical bypass or stenting is still recommended for long CTOs of the SFA. On one hand, due to the invasive nature, high complication rates and patient-related comorbidities, we believe that surgery should not be the preferred method, and, on the other hand, full lesion stenting for long CTOs has obvious consequences of permanent metallic implants like instent restenoses or stent fractures. 6 Furthermore, a stent strategy implies a mechanical barrier, through stent struts along with the prohibition of potential distal anastomosis for future surgical options. An alternative is the use of DCBs, which combines balloon dilatation with local delivery of an antiproliferative drug. Proof-of-concept evidence has demonstrated the utility of different DCB technologies in reducing both restenosis and the need for reintervention in comparison with percutaneous transluminal angioplasty (PTA). 7 This strategy may thus serve as an alternative to a stent-first approach.8,9 However, in case of massive calcification, PTA and DCB-only strategies do not provide sufficient primary patency rates. 10 Recently, the safety of the combination of atherectomy with concomitant DCB treatment with a 1-year follow-up was shown. While this study was inadequately powered and was prespecified to exclude occlusions >5 cm, a low-dissection and low-bailout stenting rate was observed in severely calcified lesions, although with a higher number of distal embolization and perforation. Thus, an adequate vessel preparation with atherectomy might potentially improve outcomes of DCB treatment and improve patency. 11
Conclusion
In conclusion, we provide a feasible endovascular-first strategy for the treatment of a long CTO of the SFA for patients refusing open surgery. Further randomized investigations are needed to evaluate long-term clinical outcomes of these novel techniques.
Footnotes
Declaration of conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge support by the Open Access Publication Fund of the University of Duisburg-Essen.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.