
Abstract
Objective
To explore the influence of apolipoprotein E (APOE) genotypes and blood lipid metabolism on coronary artery disease (CAD) with atrial fibrillation (AF).
Methods
Patients with suspected CAD were consecutively enrolled and divided into groups with or without CAD and/or AF. Blood lipid levels and APOE genotypes were determined and analysed for associations with CAD and AF.
Results
A total of 2048 patients were included (400 patients without CAD or AF [controls], 126 patients without CAD but with AF, 1294 patients with CAD without AF, and 228 patients with CAD and AF). Age and lipoprotein (a) (Lp[a]) levels were significantly higher in patients with CAD and AF versus those with CAD without AF. Among patients with CAD, the E3/E3 genotype and ε3 allele frequencies were significantly lower in patients with AF than in those without AF, and the E4/E4 genotype and ε4 allele frequencies were significantly increased. Multivariate logistic regression revealed that increased Lp(a) levels and age were independent risk factors for AF in patients with CAD.
Conclusion
Among patients with CAD, those with AF had increased age, ε4 frequencies and Lp(a) levels. Age and Lp(a) levels may be independent risk factors for AF in patients with CAD.
Keywords
Introduction
Coronary artery disease (CAD) is currently the most common cardiovascular disease, and with a gradually increasing incidence, it has become the main cause of death in developed and developing countries.1–3 Of the arrhythmias, atrial fibrillation (AF) is the most prevalent type. 4 In addition to increasing the incidence of cardiogenic stroke, AF may significantly increase the risk of heart failure and death in patients with CAD,5,6 bringing a heavy burden to human health.7,8 Thus, AF and CAD have undoubtedly become the two most attention-worthy cardiovascular diseases. While AF is an electrical atrial disease, CAD is a disease of the vascular structure. 9 However, many studies have shown that AF and CAD are closely related,10–12 which may explain the common mechanisms associated with occurrence and development, and their common risk factors, such as dyslipidaemia, fibrosis, inflammation, hypertension, and age.13–15 The correlation between dyslipidaemia and the occurrence and development of AF has received increasing attention, however, many controversies remain,16–20 resulting in the need for further investigation.
The apolipoprotein E (APOE) gene, involved in lipoprotein synthesis and metabolism, has three main subtypes, E2, E3 and E4, encoded by the corresponding ε2, ε3 and ε4 alleles, and has six possible genotypes, E2/2, E2/3, E2/4, E3/3, E3/4 and E4/4. 21 Previous studies have shown that both AF and CAD are related to genetic factors, and there is a strong genetic component for the diseases.22–24 The ε4 allele of APOE is related to the incidence of atherosclerosis and CAD,25,26 and APOE has been shown to be associated with AF in the Alzheimer's disease population.27,28 However, few studies have investigated APOE and AF in patients with CAD. Thus, the aim of the present study was to explore the effects of APOE and blood lipids on CAD with AF.
Patients and methods
Study population
This observational case–control study included consecutively enrolled patients who were admitted to the Affiliated Hospital of Xuzhou Medical University, Xuzhou, China, for suspected CAD between June 2020 and July 2021. Relevant information was collected from the patients’ clinical records and all included patients underwent coronary angiography or coronary computed tomography angiography (CTA) examination. The diagnostic criteria for CAD were as follows: typical angina symptoms and a coronary vascular examination showing that the diameter of the subepicardial coronary artery was >50%, or a noninvasive examination showing that the patient had evidence of myocardial ischemia. 29 AF was defined as the disappearance of P waves on electrocardiogram, the presence of F waves of different sizes, shapes, and amplitudes, an F wave frequency of 350 to 600 beats per min, and a variable R–R interval. 30 The exclusion criteria were as follows: (1) patients with incomplete clinical data, including the lack of basic clinical data, and unsuccessful completion of coronary angiography or coronary CTA; (2) patients with prehospital use of lipid-lowering drugs, such as statins; (3) patients with severe liver and/or kidney dysfunction (significant damage to liver or kidney structure and function); and (4) patients with thyroid disease (abnormal thyroid function) and multiple organ dysfunction (simultaneous or sequential dysfunction of two or more organs). Enrolled patients were grouped according to the presence or absence of CAD and AF, as follows: control group (CAD– AF–, patients without CAD or AF), CAD– AF+ group (patients without CAD but with AF), CAD+ AF– group (patients with CAD without AF) and CAD+ AF+ group (patients with both CAD and AF).
The study was approved by the Ethics Committee of Xuzhou Medical University, and all enrolled patients provided written informed consent. The reporting of this study conforms to STROBE guidelines. 31
Clinical and laboratory data
After hospitalization and study enrolment, the demographic and clinical data of all participants were collected, including sex, age, body mass index (BMI [kg/m2]), smoking status, hypertension, and diabetes. Diabetes and hypertension were defined according to the relevant published diagnostic criteria,32,33 and smoking was defined as continuous or cumulative smoking for more than 6 months. 34
Determination of blood lipids and APOE genotype
Peripheral venous blood was drawn from patients on an empty stomach into tubes containing ethylenediamine tetra acetic acid (EDTA) anticoagulant and used immediately, with 1 ml of the sample used to evaluate blood biochemistry, as follows: total cholesterol and triglycerides were measured using a blood lipid biochemical test kit (TEGEN, Shanghai, China); high-density lipoprotein cholesterol (HDL-C) was determined by a phosphotungstic precipitation method with reagents from Zhongsheng Beikong Bio-technology (Beijing, China); low-density lipoprotein cholesterol (LDL-C) was obtained by formula calculation; and lipoprotein(a) (Lp[a]) was measured using a sandwich enzyme-linked immunosorbent assay kit (Rayzbio Technology, Shanghai, China), with results evaluated in a plate reader by absorbance readings at 450 nm. All assays were performed according to the manufacturer’s instructions.
Single nucleotide polymorphisms in the APOE gene were detected using a commercial kit (Beyotime, Shanghai, China). Briefly, DNA as extracted from 2 ml of the patient’s blood sample in EDTA using a DNA extraction kit (Beyotime) according to the manufacturer’s instructions. Genomic DNA was then subjected to polymerase chain reaction (PCR) with primers specific to the APOE gene: sense, 5′-AACAACTGACCCCGGTGGCG-3′; antisense, 5′-ATGGCGCTGAGGCCGCGCTC-3′; and sense, 5′-CCCACCTGCGCAAGCTGCGC-3′, using thermal cycling conditions according to Hixson and Vernier. 35 In brief, each reaction mixture was heated at 95°C for 5 min for denaturation, then subjected to 30 amplification cycles of primer annealing at 60°C for 1 min, extension at 70°C for 2 min, and denaturation at 95°C for 1 min. An Affymetrix gene chip reader (Subsidiary of Thermo Fisher Scientific; Santa Clara, CA, USA) was used to read the fluorescence curve of the amplified product sample, according to the manufacturer’s instructions.
Statistical analyses
Data were statistically analysed using IBM SPSS software, version 22.0 (IBM, Armonk, NY, USA). Continuous variables are presented as mean ± SD, and were compared between groups with Student’s t-test. Categorical variables are presented as frequencies and were compared using χ2-test or Fisher's exact test. Spearman’s rank correlation coefficient was used to compare the correlation between ε4 and Lp(a). Variables were then incorporated into multiple logistic regression analysis to evaluate the independent risk factors that determine the presence of AF in patients with CAD. A P value <0.05 was considered statistically significant.
Results
Study population characteristics
The study included a total of 2048 patients who were divided into four groups: control group (CAD– AF–, n = 400); CAD– AF+ group (n = 126); CAD+ AF– group (n = 1294); and CAD+ AF+ group (n = 228). The basic clinical and demographic characteristics of the study population are summarized in Table 1. Compared with the control group, patients with CAD and/or AF were significantly older (P < 0.05); and BMI, the proportion of male patients, and those with hypertension, diabetes, and who smoked was significantly higher in patients with CAD (P < 0.05). Patients with both CAD and AF were significantly older than patients with CAD without AF (P < 0.05; Table 1).
Study population characteristics.

Data presented as mean ± SD or n (%) prevalence.
BMI, body mass index; CAD, coronary artery disease; AF, atrial fibrillation.
*P < 0.05 versus controls (CAD− AF−); **P < 0.001 versus controls (CAD−AF−); #P < 0.05 versus CAD+ AF−.
Comparison of blood lipids in the study population
Compared with the control group, levels of total cholesterol, LDL-C, and Lp(a) were significantly increased in patients with CAD, and HDL-C was significantly decreased (P < 0.05); although levels of triglycerides were numerically higher, the difference was not statistically significant. The Lp(a) levels were significantly higher in the CAD+ AF+ group versus the CAD+ AF– group (P < 0.05; Table 2).
Biochemical data of the study population.
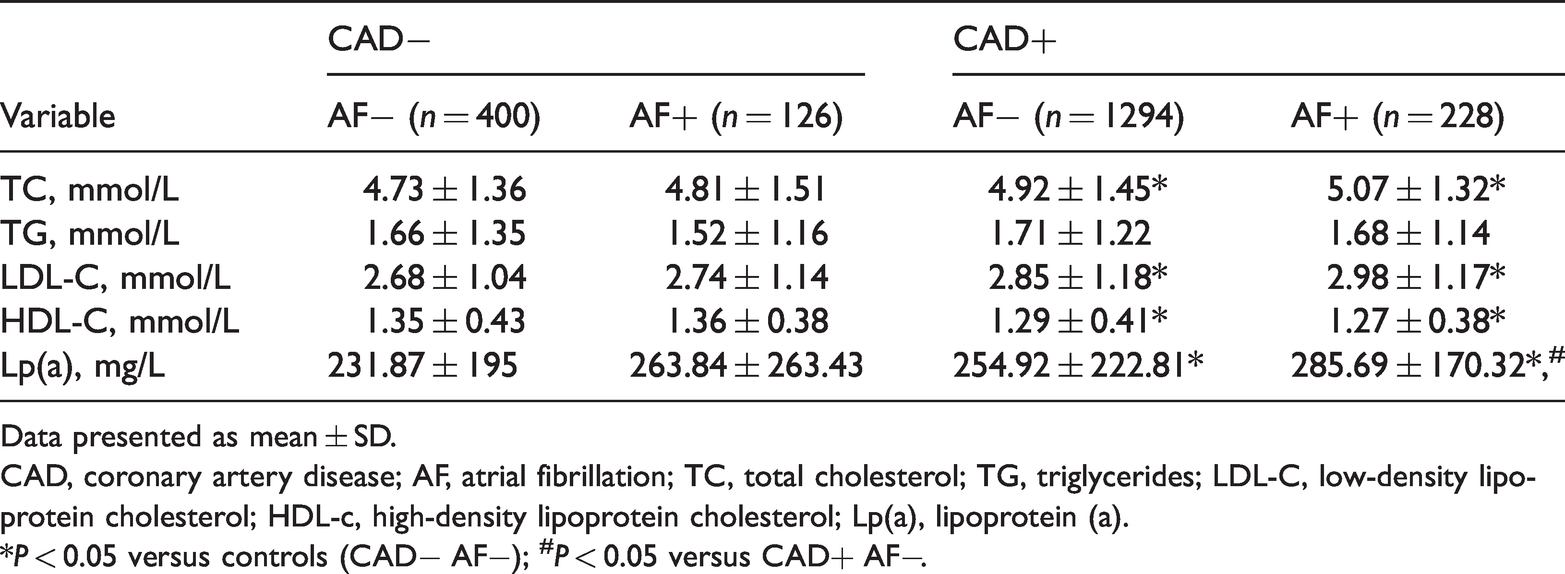
Data presented as mean ± SD.
CAD, coronary artery disease; AF, atrial fibrillation; TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-c, high-density lipoprotein cholesterol; Lp(a), lipoprotein (a).
*P < 0.05 versus controls (CAD− AF−); #P < 0.05 versus CAD+ AF−.
Distribution of APOE genotypes among the study population
Compared with the control group, frequencies of the E3/E4 and E4/E4 genotypes and ε4 allele were significantly increased in patients with CAD, and frequencies of the E3/E3 genotype and ε3 allele were significantly decreased. In addition, among patients with CAD, frequencies of the E3/E3 genotype and ε3 allele were significantly lower in patients with AF than in those without AF, and frequencies of the E4/E4 genotype and ε4 allele were significantly increased (P < 0.05; Table 3).
Prevalence of apolipoprotein E (APOE) gene polymorphisms in the study population.

Data presented as n (%) prevalence.
CAD, coronary artery disease; AF, atrial fibrillation.
*P < 0.05 versus controls (CAD− AF−); **P < 0.001 versus controls (CAD− AF−); #P < 0.05 versus CAD+ AF−; ##P < 0.001 versus CAD+ AF−.
Correlation between the APOE ε4 allele and Lp(a) levels in patients with CAD with or without AF
Analysis by Spearman's rank correlation coefficient revealed that in patients with CAD, although ε4 and Lp(a) levels were correlated, the correlation was weak (r = 0.106 [P < 0.001]; Table 4). In patients with CAD, Lp(a) levels were significantly higher in the ε4 group than in patients without ε4 (P < 0.05; Figure 1).
Correlation between the apolipoprotein E (APOE) ε4 allele and Lp(a) in patients with CAD.a
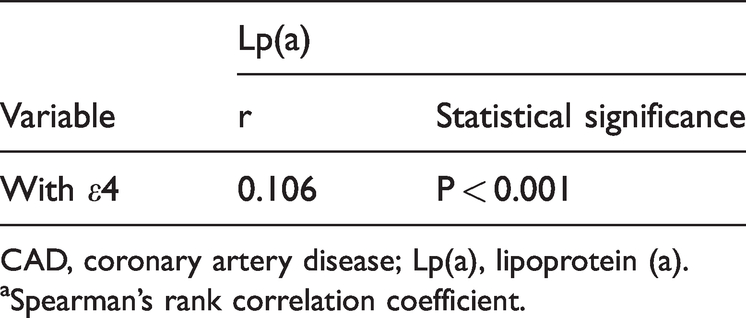
CAD, coronary artery disease; Lp(a), lipoprotein (a).
aSpearman’s rank correlation coefficient.
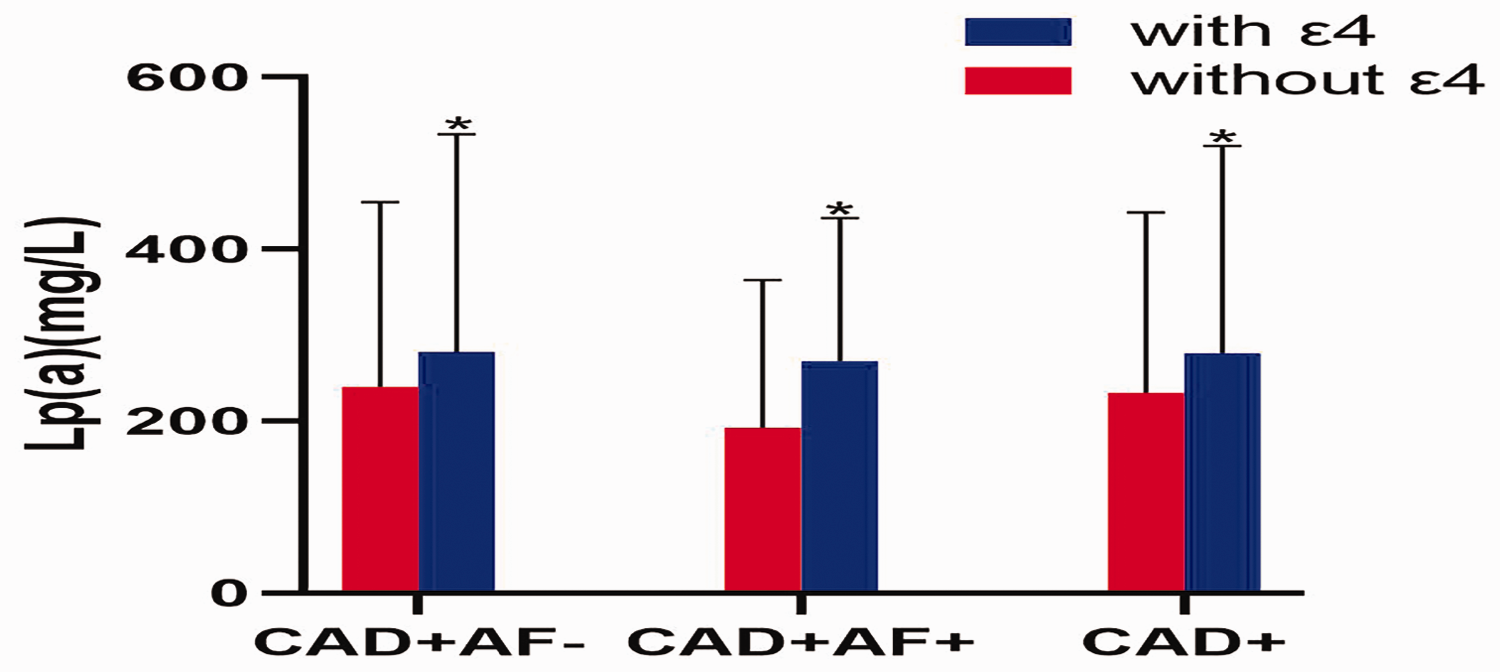
Comparison of Lp(a) between patients with CAD with or without the apolipoprotein E ε4 allele. Lp(a), lipoprotein (a); CAD, coronary artery disease. Data presented as mean ± SD; *P < 0.05 versus patients without ε4.
Multiple logistic regression analysis of patients with CAD with or without AF
The logistic regression analysis included all potential risk factors, and revealed that increased Lp(a) levels (P = 0.041) and age (P = 0.01) were independent risk factors for AF in patients with CAD (Table 5).
Multiple logistic regression analysis of potential risk factors for AF in 1522 patients with CAD.

BMI, body mass index; CAD, coronary artery disease; AF, atrial fibrillation; Lp(a), lipoprotein (a); ε4, apolipoprotein E ε4 allele.
NS, no statistically significant correlation with AF (P > 0.05).
Discussion
Coronary artery disease and AF, the most common cardiovascular disease and arrhythmia type, respectively, have become significant threats to human health, and many studies have shown them to be correlated.36–38 The main risk factors for AF are also risk factors for CAD, and include age, race, blood lipid levels, obesity, hypertension, and certain lifestyle factors.39–41 Blood lipid levels are an established risk factor for CAD, with the relationship between blood lipid levels and AF becoming a research hotspot.16,17 Both CAD and AF show strong genetic correlations, therefore, the present study aimed to explore the internal connection between CAD and AF through assessment of the differences in blood lipid levels and expression of the regulatory gene APOE in patients with CAD and AF.
In the present study, comparison of clinical data showed that patients with AF or CAD were significantly older than controls without CAD or AF, and BMI, the proportion of male patients, and those with hypertension, diabetes, and smoking were significantly higher in patients with CAD. Among patients with CAD, those with AF were significantly older than patients without AF. These results concur with the epidemiological manifestations of CAD and AF.29,30 The present study also showed that, compared with the control group, levels of total cholesterol, LDL-C, and Lp(a) were significantly increased in patients with CAD, and HDL-C was significantly reduced. Since the associations between triglyceride levels and CAD have been controversial, it is worth noting that although patients with CAD in the present study were found to have an increasing trend in triglyceride levels, no statistical significance was found. A previously published report attracted much attention by stating that hypertriglyceridemia should not be regarded as a single entity, but should be regarded according to the multiple conditions of total particle number and composition, 42 which may explain the ongoing controversy over triglycerides in the research of CAD. In addition, research data on the relationship between blood lipid levels and AF remain inconclusive and controversial. Among published research, a more convincing study by Jiang et al., 43 used Mendelian randomization methods to assess the association between blood lipid levels and the risk of AF. Regarding causality, large-scale multivariable Mendelian randomization studies have shown that there is a positive causal relationship between high Lp(a) levels and an increased risk of AF. 43 Among patients with CAD in the present study, levels of Lp(a) in patients with AF were significantly higher than in patients without AF. However, in patients without CAD, there were no significant differences in Lp(a) levels between patients with or without AF. This result may have been due to the relatively low sample size in the present study, or differences in comorbid diseases, and requires more data from larger samples for further investigation.
Next, the prevalence of APOE genotypes were compared between the present study groups. Compared with controls, the frequency of the E3/E4, E4/E4 genotypes and ε4 allele was significantly increased in patients with CAD, and the frequency of the E3/E3 genotype and ε3 allele was significantly decreased. These results are similar to those of previous studies indicating that the APOE genotype is closely related to the occurrence and development of CAD.25,26 It is worth noting that among patients with CAD, the frequency of ε4 was significantly higher in patients with AF than in patients without AF. Published studies on AF and APOE are lacking, and currently available studies mainly focus on cerebrovascular diseases, particularly Alzheimer’s disease.27,28,44,45 Falsetti et al. 44 showed that in Alzheimer's disease, the ε4 allele in patients with AF was associated with a higher risk of rapid cognitive deterioration. A population-based study from Finland, the CAIDE study, 45 showed that AF was an independent risk factor for dementia and Alzheimer's disease, and this association was related to the ε4 genotype. Similar to these results, it seems that ε4 plays an important role in patients with CAD and AF.
Carriers of the APOE gene ε4 allele have been shown to have higher total cholesterol and Lp(a) levels.46,47 The present study found that in patients with CAD, Lp(a) levels were significantly higher in patients with the ε4 allele than in those without ε4. However, subsequent analysis by Spearman’s correlation coefficient showed that, although there was a correlation between ε4 carriers and Lp(a) levels, the correlation was weak. Therefore, Lp(a) levels, the ε4 genotype and other possible risk factors were included in multiple logistic regression analysis. The results suggest that age and Lp(a) levels may be independent risk factors for AF in patients with CAD, which is novel information regarding CAD with AF.
The results of the present study may be limited by several factors. First, this was a single-centre study, and the study population was entirely Han ethnicity, thus, the results may not be representative of the general population. In addition, similar results were not observed when comparing AF in patients with CAD versus patients without CAD, and at present, we cannot provide a satisfactory explanation. Future multicentre, larger sample studies are needed to further clarify the results.
In conclusion, among patients with CAD, patients with AF had increased age, ε4 frequencies and Lp(a) levels. Age and Lp(a) levels may be independent risk factors for AF in patients with CAD.
Footnotes
Acknowledgments
This manuscript is part of a preprint at research square: DOI 10.21203/rs.3.rs-998002/v1.
Author contributions
Lei Chen, Yameng Shao, Min Zhang and Li Zhi performed the experiments and analysed the data. Yong Li and Yuan Lu designed the study and wrote the manuscript.
Data accessibility
The original data supporting the conclusions of this manuscript will be provided by the author to any qualified researcher without reservation.
Declaration of conflicting interest
The Authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.