
Abstract
Objectives
To investigate the co-prevalence of coronary artery disease (CAD) and carotid stenosis and to determine predictors related to CAD in Chinese patients with paroxysmal atrial fibrillation (PAF), presenting without previously diagnosed or excluded CAD.
Methods
Consecutive patients with PAF were recruited. CAD was evaluated using multislice computed tomography. Intima–media thickness (IMT) of the carotid artery was evaluated via ultrasonography.
Results
A total of 62/192 (32.3%) patients had CAD. Carotid stenosis was observed in 26/192 (13.5%) patients. The co-prevalence of carotid stenosis and CAD was 7.8% (15/192). The prevalence of carotid stenosis was 8.5%, 16.7%, 25.0%, and 41.7% in patients with zero-, one-, two-, and three-vessel CAD, respectively. Diabetes mellitus, maximal IMT and hyperhomocysteinaemia were independently related to the presence of CAD.
Conclusions
The prevalence of CAD was 32.3% in Chinese patients with PAF. Carotid stenosis and CAD co-occurred in 7.8% of patients, and the prevalence of carotid stenosis correlated with the severity of CAD. Screening of carotid stenosis is recommended, especially in patients with PAF and multivessel CAD.
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia and accounts for a quarter of ischaemic strokes. 1 AF is associated with multiple symptoms, substantial morbidity and mortality and decreased health-related quality-of-life (HRQoL). 2 The mortality rate for patients with AF is almost twice that for individuals with normal sinus rhythm: a fact that has been attributed to increased cardiac death due to underlying heart disease3,4 rather than to thromboembolism. 5
Arterial fibrillation is known to be associated with coronary6–8 or carotid atherosclerosis.9–11 In patients with AF, the presence of atherosclerotic vascular disease is believed to amplify the risk of thromboembolic stroke and vascular death.12–14 Coronary artery disease (CAD) is frequently associated with carotid stenosis and carotid atherosclerosis, 15 but the co-prevalence of CAD and carotid atherosclerosis in patients with AF has not been studied.
The aims of the present study were to investigate the co-prevalence of CAD and carotid atherosclerosis, and to determine predictors related to CAD in Chinese patients with paroxysmal AF (PAF), presenting without previously diagnosed or excluded CAD.
Patients and methods
Study population
The study recruited consecutive patients with drug-refractory PAF who underwent multislice computed tomography (MSCT) for coronary evaluation (due to an elevated risk profile and/or chest pain) at Zhengzhou People’s Hospital, Zhengzhou, Henan, China, between June 2010 and October 2012. PAF was defined as self-terminating episodes of AF lasting ≤ 7 days. Patients with previously diagnosed or previously excluded CAD, dilated or hypertrophic cardiomyopathy or contraindications to MSCT were excluded, in addition to patients who were not in sinus rhythm during MSCT examination.
All patients provided written informed consent prior to enrolment and the study was approved by the ethics committee of Zhengzhou People’s Hospital, Zhengzhou, Henan, China.
Proatherogenic risk factors
Data regarding proatherogenic risk factors were collected before MSCT. These included sex, age, body mass index (BMI), hypertension (systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg or receiving antihypertensive medication), diabetes mellitus, hyperlipidaemia (low-density lipoprotein cholesterol [LDL-C]; triglyceride [TG], high-density lipoprotein cholesterol [HDL-C]), smoking, family history of CAD, estimated glomerular filtration rate (eGFR, calculated using the modification of diet in renal disease formula), 16 hyperhomocysteinaemia (HHcY; total plasma homocysteine [tHcy] ≥12.0 µmol/l), and previous transient ischaemic attack or stroke.
Coronary angiography
Multislice computed tomography coronary angiograms were obtained with 64-slice scanners (LightSpeed VCT, GE Medical Systems, Slough, UK) to determine the presence of CAD. Both the original axial dataset and curved multiplanar reconstructions were used. CAD was defined as lumen diameter stenosis > 50% in ≥ 1 major coronary artery. Patients were classified according to the number of diseased vessels present: one-vessel disease; two-vessel disease (disease in two vessels or left main trunk disease without right coronary artery stenosis); three-vessel disease (disease in three vessels or left main trunk disease with right coronary artery stenosis).
Carotid atherosclerosis
Carotid artery atherosclerosis was evaluated within one month before coronary MCST using duplex ultrasonography with a 10-MHz linear array transducer. Scanning of the extracranial common carotid artery (CCA), the carotid bulb (Bul), and the internal carotid artery (ICA) in the neck was performed bilaterally in three longitudinal and transverse projections, and the site of greatest intima–media thickness (IMT) including plaque lesions was sought along the arterial walls using B-mode and colour Doppler ultrasound. Max-IMT was defined as the largest carotid IMT in the observed areas of the CCA, Bul and ICA. 17 Carotid stenosis was defined as atherosclerotic area stenosis of > 50% or peak systolic velocity of > 200 cm/s on the above carotid arteries. All scans were conducted by experienced laboratory technicians and physicians who had no prior knowledge of the patient’s clinical characteristics.
Statistical analyses
Data were expressed as mean ± SD for continuous variables and n (%) for categorical variables. Normally distributed data were analysed using unpaired Student’s t-test, χ2-test or Fisher’s exact test, as appropriate. Mann–Whitney U-test was used when data deviated from a Gaussian distribution (evaluated via Kolmogorov–Smirnov test). Multivariate stepwise logistic regression analysis was applied to evaluate the relationship between demographic and clinical data and the presence of CAD. Data were analysed using SPSS® version 11.0 (SPSS Inc., Chicago, IL, USA) for Windows®. P-values < 0.05 were considered statistically significant.
Results
Demographic and clinical characteristics of Chinese patients with paroxysmal atrial fibrillation (PAF) with or without coronary artery disease (CAD), included in a study investigating the coprevalence of CAD and carotid stenosis (CS) (n = 192).
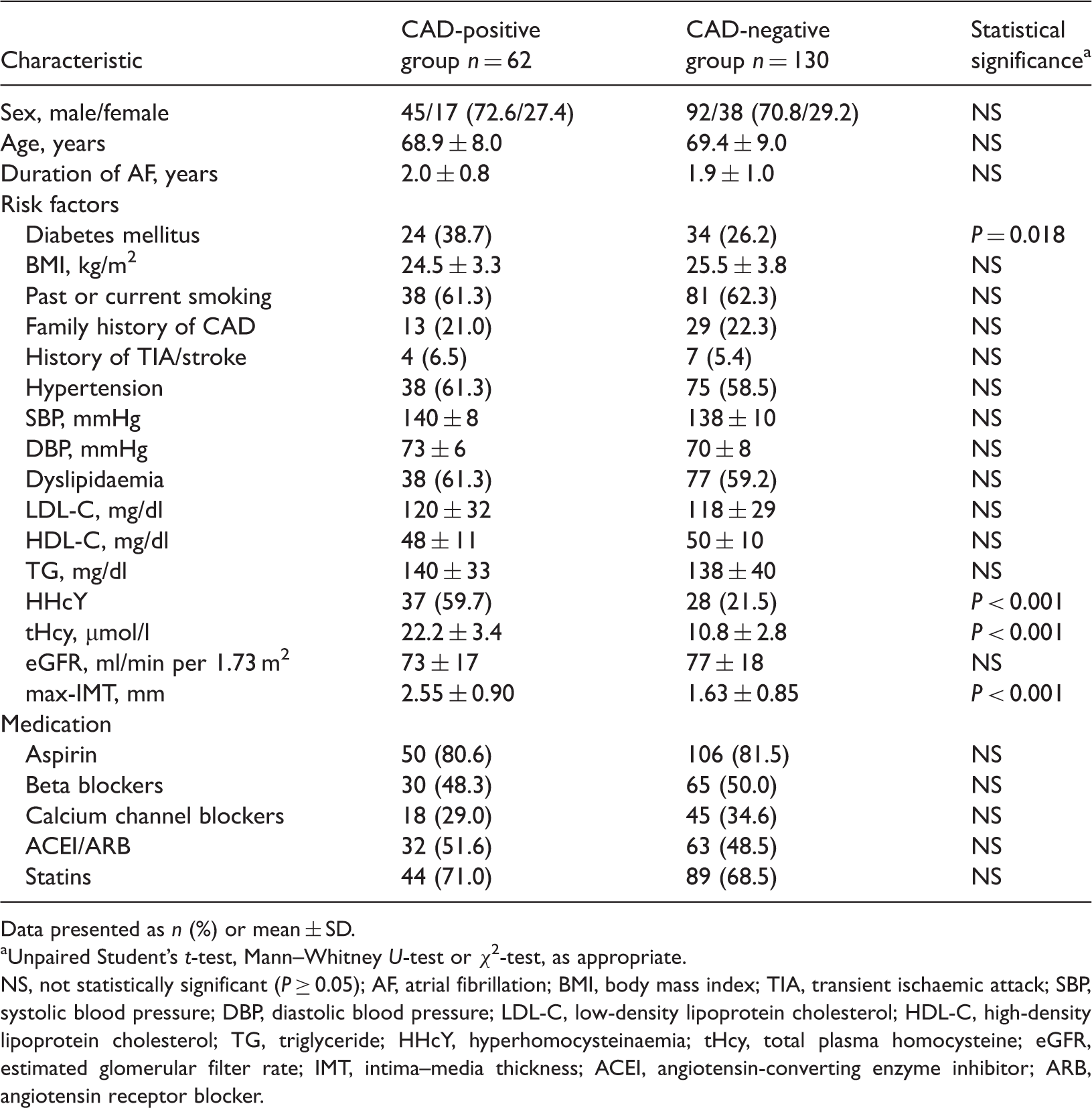
Data presented as n (%) or mean ± SD.
Unpaired Student’s t-test, Mann–Whitney U-test or χ2-test, as appropriate.
NS, not statistically significant (P ≥ 0.05); AF, atrial fibrillation; BMI, body mass index; TIA, transient ischaemic attack; SBP, systolic blood pressure; DBP, diastolic blood pressure; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TG, triglyceride; HHcY, hyperhomocysteinaemia; tHcy, total plasma homocysteine; eGFR, estimated glomerular filter rate; IMT, intima–media thickness; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker.
Of the 62 patients with CAD, 30 (48.4%) had one-vessel disease, 20 (32.3%) had two-vessel disease, and 12 (19.4%) had three-vessel disease. The prevalence of carotid stenosis in patients with CAD was 24.2% (15/62). When stratified according to the number of vessels affected, the prevalence of carotid stenosis was 8.5% (11/130), 16.7% (five of 30), 25.0% (five of 20), and 41.7% (five of 12) of patients with zero-, one-, two-, and three-vessel disease, respectively (P < 0.001). In the study population as a whole, 26 (13.5%) patients had carotid stenosis and 15 (7.8%) had carotid stenosis and CAD.
Multiple logistic regression analysis (using age, male sex, smoking, diabetes mellitus, hypertension, high BMI, high LDL-C, high TG, low HDL-C, low eGFR, HHCY and max-IMT as dependent variables) found that CAD was independently associated with HHcY (odds ratio [OR] 2.12; 95% confidence intervals [CI] 2.12, 5.24), diabetes mellitus (OR 2.08; 95%CI 1.36, 3.06) and max-IMT (OR 3.08; 95%CI 2.34, 5.14).
Discussion
The present study used anatomical assessment to evaluate the prevalence of coexisting CAD and carotid atherosclerosis among Chinese patients with PAF, and found that the prevalence of CAD was 32.3%. In addition, 7.8% of patients in the present study had coexisting carotid stenosis and CAD, and the prevalence of carotid stenosis correlated with the severity of CAD. Moreover, diabetes mellitus, IMT and HHcY were independently related to the presence of CAD.
The prevalence of AF in the US population is expected to increase from 2.3 million in 2001 to 5.6 million in 2050. 18 The prevalence of CAD in patients with AF is 18–41% in Western countries,7,8,19 but only 6.4% in Japan. 20 This disparity may be linked to differences in patients’ backgrounds. The prevalence of CAD in the present study was 32.3%, consistent with that of Western countries, and may be related to the inclusion of patients with suspected CAD elevated risk profiles (including a Western-type lifestyle). Of the 62 patients diagnosed with CAD in the present study, 32 (51.6%) had multivessel disease that may require percutaneous coronary intervention or coronary artery bypass graft (CABG). Once diagnosed with AF, the presence of CAD has been shown to be related to recurrent AF episodes, 21 presence of arrhythmia, heart failure and angina, 22 and increased risk of death.23,24 Epidemiological data have indicated that ischaemic heart disease is one of the most common underlying causes of death among patients with AF. 25
Few studies have investigated the relationship between AF and carotid atherosclerosis.11,26,27 In a population-based survey, subjects with carotid atherosclerosis were more likely to develop AF than those without the condition. 11 Increased IMT and arterial stiffness have been found to be associated with lone AF, 10 and patients with AF have a substantially higher risk of stroke and death after carotid endarterectomy. 26 A prospective study reported that carotid stenosis (40–100%) and AF were significant independent risk factors for new thromboembolic stroke. 27 In the present study, 13.5% of patients with PAF had carotid stenosis, and 24.2% of patients with PAF and CAD had concomitant carotid stenosis. It is well established that patients with ‘significant’ carotid stenosis have an increased risk of stroke after CABG, and CAD is the most common cause of morbidity and mortality following carotid artery endovascular intervention.28,29
Diabetes mellitus, IMT and HHcY were independent predictors of CAD in the present study. Diabetes mellitus is known to be an independent predictor of CAD and is associated with more advanced CAD. 30 CAD is a major cause of death and impaired HRQoL in patients with type 2 diabetes mellitus, and is generally detected at an advanced, symptomatic stage. 17 The early detection of CAD is therefore critical in the management of these patients. Carotid IMT (a marker of early atherosclerosis and vascular remodelling that can be assessed quickly, noninvasively, and cheaply with high-resolution ultrasonography) is correlated with conventional coronary risk factors and is associated with cardiovascular events and extent of CAD among patients with known or suspected CAD or type 2 diabetes.10,11,17 Receiver operator characteristic curve analyses revealed that the area under the curve was higher for max-IMT than for mean-IMT. 31 In type 2 diabetic patients without apparent cardiovascular disease, the addition of max-IMT to conventional risk factors substantially improves the risk stratification for CAD. 17 Studies have indicated that tHcy concentrations are correlated with coronary atherosclerosis and stroke, and can be used to predict mortality in patients with CAD.32,33 In addition, HHcY can predict the presence of CAD and tHcy levels are significantly associated with the extent of coronary atherosclerosis in patients with carotid stenosis. 33
The present study has several limitations. First, the study population included consecutive patients with PAF alone, and our findings may not be applicable to those with nonparoxysmal AF. Secondly, the nonrandomized design of this single-centre investigation may have influenced the comparative analysis. Thirdly, no prognostic data were available. A larger study with follow-up data may provide more conclusive information. While caution is therefore needed in the interpretation of our data, we consider it improbable that these limitations have influenced our main findings.
In conclusion, the prevalence of CAD was 32.3% in Chinese patients with PAF presenting without previously diagnosed or excluded CAD. Carotid stenosis and CAD co-occurred in 7.8% of patients, and the prevalence of carotid stenosis correlated with the severity of CAD. Diabetes mellitus, IMT and HHcY were independently related to the presence of CAD. Screening of carotid stenosis is recommended, especially in patients with PAF and multivessel CAD.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The present study was supported by the Cutting-edge and Basic Research Project of Henan Province (122300410136).